
ST-Segment Depression in Leads I and aVL:Artifactual or Pathophysiological Findings?
2021-06-08 01:47ShrenLeeGryTsePhDFESCFACCFHRSFRCPXinWngAdrinBrnchukMDFACCFRCPCndTongLiuMDPhD
Shren Lee , Gry Tse, PhD, FESC, FACC, FHRS, FRCP , Xin Wng ,Adrin Brnchuk, MD, FACC, FRCPC nd Tong Liu, MD, PhD
1 Cardiovascular Analytics Group, Laboratory of Cardiovascular Physiology, Hong Kong, China
2 Tianjin Key Laboratory of Ionic-Molecular Function of Cardiovascular Disease, Department of Cardiology, Tianjin Institute of Cardiology, Second Hospital of Tianjin Medical University, Tianjin, China
3 Department of Medicine, Kingston General Hospital, Queen’ s University, Kingston, Ontario, Canada
Abstract The 12-lead electrocardiogram (ECG) is a routinely performed test but is susceptible to misinterpretation even by experienced physicians.We report a case of a 72-year-old lady with no prior cardiac history presented to our hospital with atypical chest pain.Her initial electrocardiogram shows an initial ST depression followed by positive deflections leads I and aVL.Non-physiological ST segment and T-wave changes are also observed in the precordial leads V2 to V6.By contrast, these abnormalities are notably absent in lead II.A repeat of the ECG taken 30 minutes later reveals the resolution of most abnormalities seen in the initial ECG on a background of high-frequency noise in the limb leads.She was referred to the cardiology department for further management.An urgent echocardiogram revealed no regional wall motion abnormalities with preserved ejection fraction, and her coronary angiogram revealed no significant coronary stenosis.This case illustrates the importance of understanding different factors that can cause ST segment abnormalities, notably artifactual changes that can mimic ST segment myocardial infarction.
Keywords: ST segment; artifact.
Introduction
The 12-lead electrocardiogram (ECG) is a routinely performed test but is susceptible to misinterpretation even by experienced physicians.This case illustrates the importance of understanding different factors that can cause ST-segment abnormalities.
Case Presentation
A 72-year-old woman with no prior cardiac history presented to our hospital with a long period of atypical chest pain without any predisposing factors.Her initial ECG is shown in Figure 1.An ECG taken 30 minutes later is shown in Figure 2.Her troponin I level was initially normal (< 0.02 ng/mL),and remained normal 6 hours later.
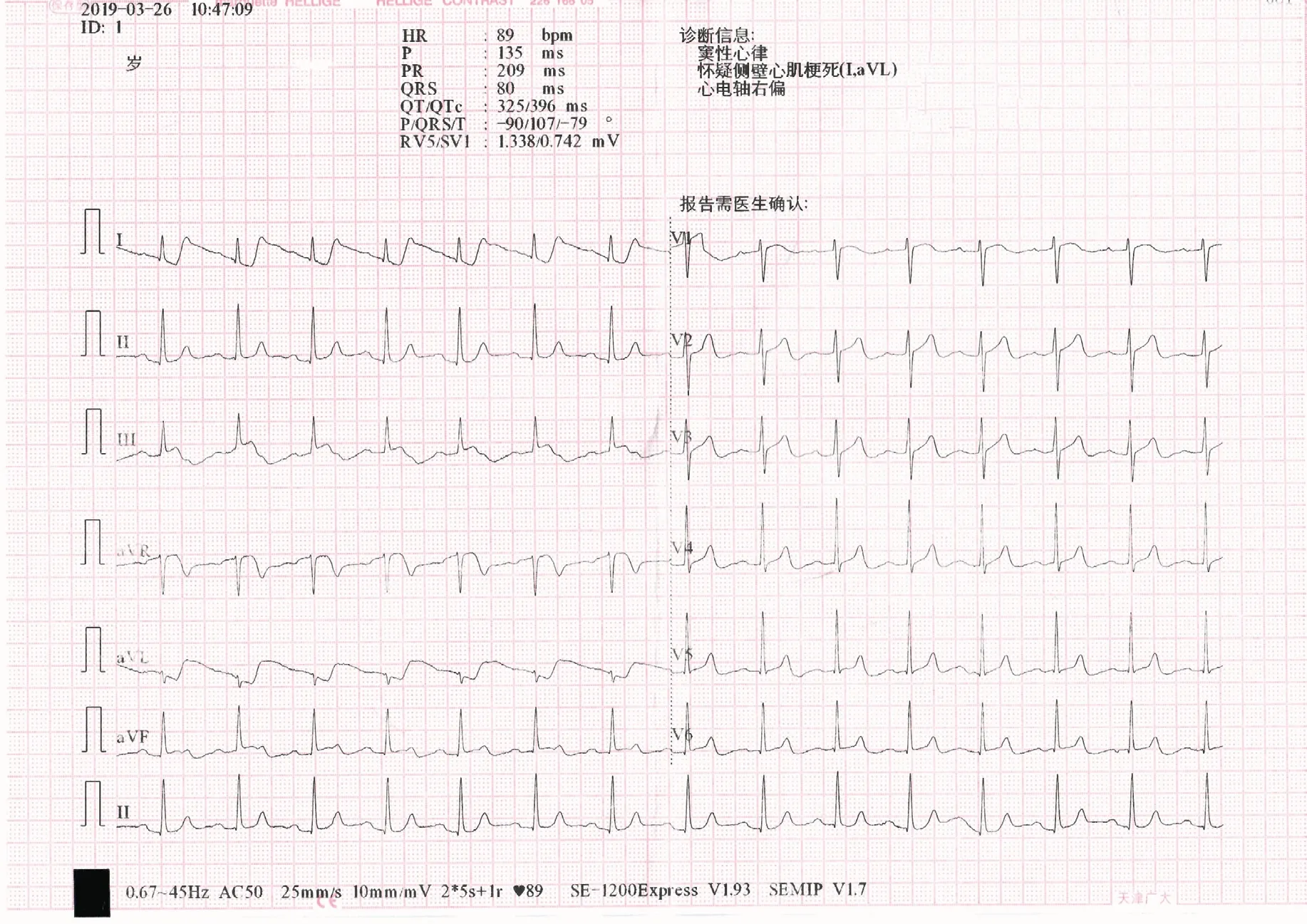
Figure 1 Initial Electrocardiogram of the Patient.
Discussion
The clinical condition presented in the emergency department would be easily misdiagnosed possibly as acute coronary syndrome (ACS).However,the main differential diagnoses include artifactual ST-segment changes and ST-segment elevation myocardial infarction (STEMI) affecting predominantly the inferior wall.Many emergency physicians will likely ignore the interference of artifacts in the ECG and make an incorrect judgement.At that time, careful analysis of the footprints of every ECG contributes to accurate differentiation of ACS from artifactual interference, given the ECG has been noted to be a valuable diagnostic tool.
For this patient, the first ECG (Figure 1) shows an initial ST-segment depression followed by positive deflections in leads I and aVL.Nonphysiological ST-segment and T-wave changes are also observed in precordial leads V2to V6.By contrast, these abnormalities are notably absent in lead II.An ECG taken 30 minutes later (Figure 2) reveals the resolution of most abnormalities seen in the initial ECG on a background of high-frequency noise in the limb leads.The patient was referred to the cardiology department for further management.An urgent echocardiogram revealed no regional wall motion abnormalities with preserved ejection fraction, and her coronary angiogram revealed no significant coronary stenosis.
There are different findings that would suggest artifacts as the cause of the ST-segment elevation in the ECG.The ST segments contained both deviated (80 ms) and nondeviated parts with a sharp transition between them, which is nonphysiological.Moreover, the ST segments completely normalized in the short period of 30 minutes without development of T-wave inversion.The artifact observed in the first ECG has been well described, called a “ pulse-tapping artifact” [1].As the ST-segment changes are most prominent in leads I, aVL, and III, the most likely cause is that the left-sided electrodes were placed inadvertently over a major coronary artery pulse on the left limb, resulting in the aforementioned artifacts appearing in Figure 1.For the second ECG, the high-frequency sharp signals may correspond to somebody noticing movement of the electrode and displacing it to a different spot, without sticking it correctly, leading to multiple sharp signals during poor electrode positioning.
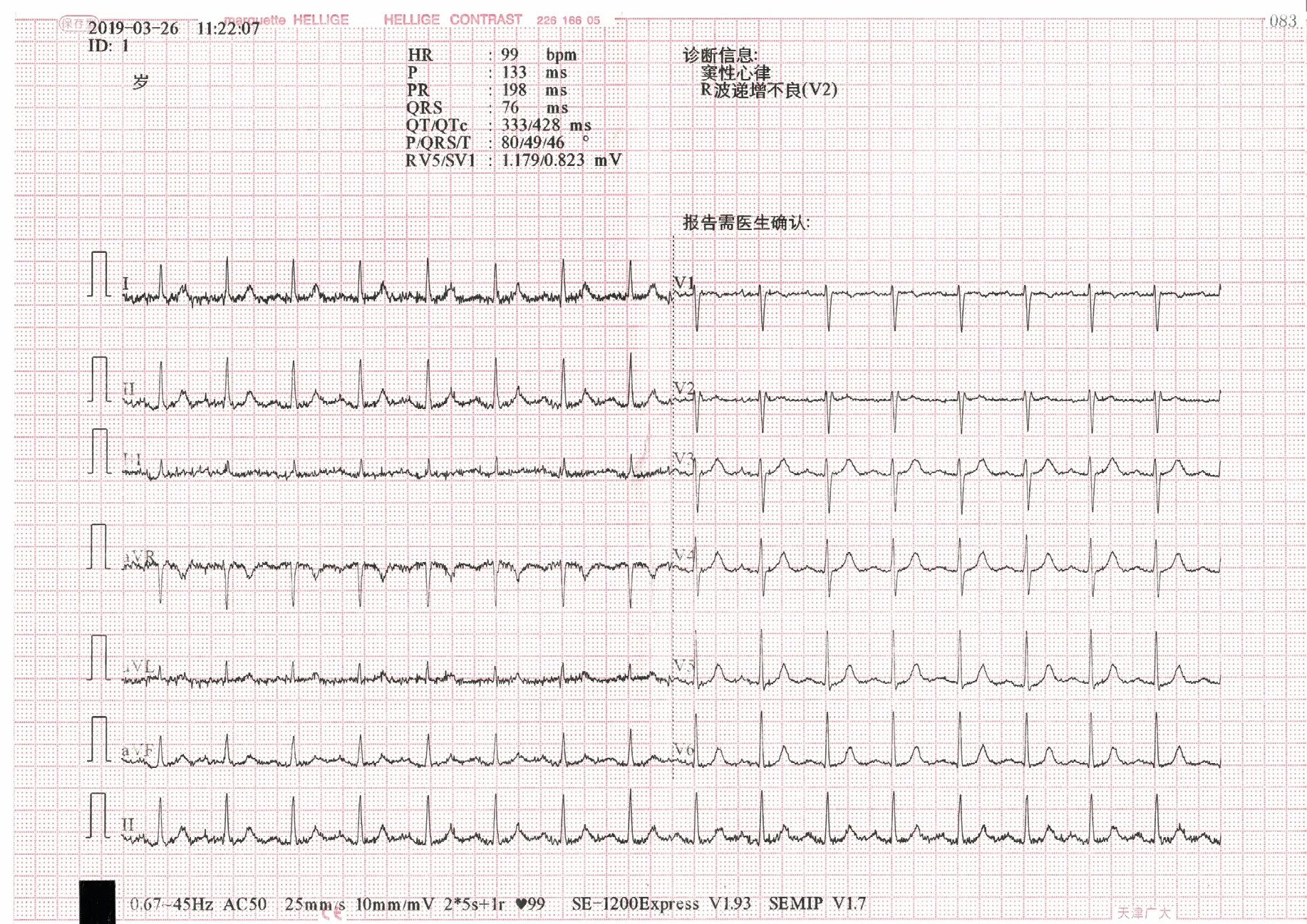
Figure 2 Electrocardiogram Taken 30 Minutes Later.
A study by Bosson et al.[2] suggested that one of the leading causes of false-positive software interpretation for STEMI is an ECG artifact.In patients with an ECG mimicking an STEMI pattern, correct recognition of artifacts on the ECG that may be interpreted by mistake as ST-segment deviations is essentially important, preventing administration of potentially harmful pharmacotherapy and invasive coronary angiography [1].Moreover,inappropriate acquisition of an ECG may result in the wrong diagnosis for the patient, with deleterious consequences.Thus, all physicians should be familiar with abnormal artifacts [3].When one is confused by the differentiation between the two conditions, recognizing them correctly is dependent on a comprehensive assessment of all clinical contexts and ECG records.If necessary, a repeated ECG after the appropriate review of the connection of all leads can exclude the possibility of artifactual interference.
Conflicts of Interest
The authors declare that they have no competing interests or financial interests.
 Cardiovascular Innovations and Applications2021年4期
Cardiovascular Innovations and Applications2021年4期
- Cardiovascular Innovations and Applications的其它文章
- Barriers to the Implementation of Primary PCI in the Management of STEMI in Egypt
- Comparison of a 5 F Microtube-Irrigated Ablation Catheter and a General Ablation Catheter in the Treatment of Resistant Hypertension with Renal Denervation
- Main Renal Artery Plus Branch Ablation in the Treatment of Resistant Hypertension with Renal Denervation
- Clinical Significance of Angiographically Detectable Neovascularity in Patients with Cardiac Myxoma
- A Case Report of Radiofrequency Ablation of Typical Atrial Flutter Combined with Atrial Tachycardia