
Associations of physical activity,sedentary time,and physical fitness with mental health during pregnancy:The GESTAFIT project
2021-05-22 00:28MarRoriguezAyllonPeroAcostaManzanoIreneCollRiscoLiiaRomeroGallaroMilkanaBorgesCosicFernanoEstevezopezVirginiaAparicio
Mar′ıa Roriguez-Ayllon,Pero Acosta-Manzano,Irene Coll-Risco,Liia Romero-Gallaro,Milkana Borges-Cosic,Fernano Est′evez-L′opez,Virginia A.Aparicio
a PROFITH“PROmoting FITness and Health through physical activity”Research Group,Sport and Health University Research Institute(iMUDS),Department of Physical Education and Sports,Faculty of Sport Sciences,University of Granada,Granada 18071,Spain
b Department of Physical Education and Sport,Faculty of Sport Sciences,University of Granada,Granada 18071,Spain
c Sport and Health University Research Institute(iMUDS),University of Granada,Granada 18007,Spain
d Department of Psychology,Faculty of Social and Behavioral Sciences,Utrecht University,CS Utrecht 3584,the Netherlands
e Department of Physiology,Faculty of Pharmacy and Institute of Nutrition and Food Technology,University of Granada,Granada 18011,Spain
Abstract Purpose:This study was aimed to analyze the associations of objectively measured physical activity(PA),sedentary time,and physical fitness with mental health in the early second trimester(16±2 gestational weeks)of pregnancy. Methods:From 229 women initially contacted,124 pregnant women participated in the present cross-sectional study.Data were collected between November 2015 and March 2017.The participants wore Actigraph GT3X+Triaxial accelerometers for 9 consecutive days to objectively measure their PA levels and sedentary time.A performance-based test battery was used to measure physical fitness.Self-report questionnaires assessed psychological ill-being(i.e.,negative affect,anxiety,and depression),and psychological well-being(i.e.,emotional intelligence,resilience,and positive affect).Linear regression analyses were adjusted for age,educational level,accelerometer wear time,miscarriages,and low back pain. Results:Moderate-to-vigorous PA was negatively associated with depression(β=-0.222,adjusted R2=0.050,p=0.041).Higher levels of sedentary time were negatively associated with positive affect(β=-0.260,adjusted R2=0.085,p=0.017).Greater upper-body flexibility was positively associated with better emotional regulation(β=0.195,adjusted R2=0.030,p=0.047).The remaining associations were not significant(all p>0.05). Conclusion:An active lifestyle characterized by higher levels of moderate-to-vigorous PA and lower levels of sedentary time during pregnancy might modestly improve the mental health of pregnant women.Although previous research has focused on the benefits of cardiorespiratory exercise,the present study shows that only upper-body flexibility is related to emotional regulation in early pregnant women.If the present findings are corroborated in further experimental research,physical exercise programs should focus on enhancing flexibility to promote improvements in emotional regulation during early second-trimester of pregnancy.
Keywords:ActiGraph GT3X;Emotional dysregulation;Psychological health;Sedentary behavior;Stretching
1.Introduction
Pregnancy induces multiple physiologic changes affecting the maternal cardiovascular,hormonal,and metabolic systems.1In addition,pregnancy is widely considered to be a period in a woman’s life of increased vulnerability to mental disorders.2Indeed,7%-15% of women during pregnancy are affected by mental disorders.3Mental disorders and poor mental health(also known as psychological ill-being,which involves unpleasant feelings or emotions that impact the level of functioning4,5)impose a negative burden on women during pregnancy.For instance,anxiety and depression are related to more severe nausea and vomiting,extended absences from work,and increased visits to physicians during pregnancy.6Higher levels of psychological ill-being during pregnancy are also linked to adverse events during childbirth;women with high levels of anxiety during the first weeks of gestation have been shown higher probability of suffering a miscarriage and have an increased risk of preterm delivery and caesarean section.7
According to the World Health Organization,mental health is“a state of well-being in which every individual realizes his or her own potential,can cope with the normal stresses of life,can work productively and fruitfully,and is able to make a contribution to her or his community”.8In this context,psychological well-being is the combination of positive affective states and functioning with optimal effectiveness in personal and social life.4,5Therefore,mental health depends not only on the absence of psychological ill-being,but also on the presence of psychological well-being.Interestingly,evidence suggests that psychological well-being during pregnancy acts as a protective factor against mental disorders not only in the mothers,9but also in their children.10Despite substantial efforts in the field,no effective interventions exist that substantially help pregnant women to cope with the psychological impact that the changes brought about by pregnancy have on women.11Thus,the search for readily modifiable intervention targets is ongoing.In this context,more physical activity(PA),fewer sedentary behaviors,and higher levels of physical fitness have been identified as promising targets not only for reducing psychological ill-being,but also for boosting psychological well-being in the general population,12,13which is desirable also for maternal and fetal health during pregnancy and later in life.14
In the last few years,it has been suggested that PA(i.e.,any body movement that increases energy expenditure above the basal metabolic rate15)may be associated with better mental health during pregnancy.16-18Although inspiring,previous research presents caveats.First,the assessment of PA has relied on self-reports.16,17Second,only psychological ill-being has been studied.18Third,there are no previous studies testing the association of sedentary time(i.e.,any waking behavior characterized by an energy expenditure≤1.5 metabolic equivalents while in a sitting,reclining,or lying posture19)or physical fitness(i.e.,a set of attributes that people have or achieve that relate to the ability to do physical activities15)with the mental health of pregnant women.Previous literature has suggested that higher levels of sedentary time and lower levels of physical fitness are related to worse mental health in the general population,13,20a relationship that remains to be corroborated in pregnant women.
To sum up,research that objectively measures PA(e.g.,by means of accelerometry)and considers not only psychological ill-being,but also psychological well-being is required to provide robust evidence.The study of levels of sedentary time(which along with PA occupies all the waking hours of a day)may help us to better understand the relationship between pregnant women’s behaviors and their levels of mental health.Furthermore,taking into account pregnant women’s levels of physical fitness(a robust physiological measure that reflects the amount of PA during the previous 3 months21)may provide a more comprehensive picture of the associations under study.Therefore,the aim of the present study was to analyze the associations of objectively measured PA,sedentary time,and physical fitness with psychological ill-being and well-being in the early second trimester of pregnancy.Based on previous literature,we hypothesized that higher levels of PA and physical fitness would be related to better mental health in pregnancy.We expect increased levels of sedentary time would be related to a worst mental health in pregnant women.
2.Methods
2.1.Participants
The present cross-sectional study was developed in Granada(southern Spain)within the GESTAtion and FITness(GESTAFIT)project framework.22For feasibility reasons,the baseline data collection occurred in 2 waves between November 2015 and March 2017.From the 229 pregnant women initially contacted,161 women in early pregnancy were recruited at their first visit to a hospital(typically during the 12th gestational week).Of the 161 women recruited at the first assessment,a total of 37 were excluded either because they did not meet the inclusion criteria(n=2)or because they declined to participate(n=35).Data for the remaining 124 participants(32.9±4.7 years,mean±SD)were included in these analyses.
A detailed description of the study design and methods has been published elsewhere.22Briefly,the inclusion criteria included the following:(i)participants answered“no”to all questions on the PARmed-X for pregnancy health checklist23and(ii)participants were able to walk without assistance,were able to read and write sufficiently(e.g.,they do not need help to fill out the questionnaires),and were willing and able to provide consent.The exclusion criteria included having an acute or terminal illness,malnutrition,the inability to participate in a physical fitness test,pregnancy risk factors,multiple pregnancies,chromosopathy or fetal malformations,uterine growth restriction,an upper or lower extremity fracture in the past 3 months or registration in any other exercise program.22
The participants provided written informed consent before taking part in this study,which was approved by the Clinical Research Ethics Committee of Granada,Government of Andalusia,Spain(Code:GESFIT-0448-N-15).The study was conducted following the ethical guidelines of the Declaration of Helsinki,last modified in 2013.
2.2.Procedures
After being contacted by the research team during their first gynecological visit to the Hospital in their 12th gestational week,participants were invited to carry out the study at the Sport and Health Research Centre,University of Granada,Spain.Data on the age,weight,height,and phone number of participants were collected during their first visit to the hospital.During the 16th±2nd gestational week,a first assessment was conducted.The assessments were always conducted over 1 day in the same order.First,each participant filled out an initial self-report survey to provide information on her sociodemographic and clinical characteristics.Second,each participant completed the mental health questionnaires(i.e.,the 10-item Connor-Davidson Resilience Scale,the Center for Epidemiological Studies Depression Scale(CES-D)questionnaire,the Positive and Negative Affect Schedule,the Trait subscale of the State-Trait Anxiety Inventory(STAI-T),and Trait Meta-Mood Scale(TMMS)).Third,each participant performed the physical fitness tests(i.e.,back-scratch test,handgrip test,6-min walk test).Afterward,participants were asked to wear the accelerometers for 9 consecutive days.
2.3.Outcomes
We objectively assessed the PA and sedentary time using ActiGraph GT3X+Triaxial accelerometry(ActiGraph,Pensacola,FL,USA),with an epoch length of 60 s and a frequency rate of 30 Hz.This method has previously been used in pregnancy studies,and the methodology followed in the present study was similar to the one used in previous studies.24The participants wore the accelerometer on their waist for 9 consecutive days,24 h/day,except during water-based activities.Participants had to have data for a total of 7 days of wearing time(5 weekdays and 2 weekend days)with a minimum of≥10 h per waking day to be included in the analyses.The accelerometer wearing time was calculated by deducting the sleeping time and the non-wear time from the total time registered for the whole day.Recordings with values of≥20,000 counts/min were excluded because of potential malfunction.We also excluded from the analyses all 90-min bouts with 0 activity intensity count.The time involved in bouted moderate-to-vigorous PA(MVPA)(periods of≥10 continuous minute of MVPA)was calculated based on a PA recommended vector magnitude cut-point of≥2690 counts/min(up to 2 min below the cut-point allowance),and it was expressed in min/week.25Sedentary time was calculated as the amount of time accumulated below 200 counts/min and was expressed in min/day.26The data download,reduction,cleaning,and analyses were performed using ActiGraph software(ActiLife Version.6.11.9;ActiGraph).Of the 124 remaining participants,22 were excluded because they did not wear the accelerometer(n=5),they had incorrect data owing to accelerometer malfunction(n=5),or they did not have enough wearing days and/or hours(n=12).The accelerometry data of the remaining 102 participants were analyzed.
We evaluated upper-body flexibility by the back-scratch test,a measure of overall shoulder range of motion.The distance between(or overlap of)the middle fingers behind the back was measured with a ruler.27The best score of 2 trials for each arm was recorded,and the average of both arms was used for the analyses.Upper-body muscular strength was evaluated by handgrip strength,as described elsewhere.28The participants performed the handgrip strength test twice,alternately with both hands,using a digital dynamometer(TKK 5101 Grip-D;Takey,Tokyo,Japan).The best value of 2 attempts for each hand was recorded,and the average of both hands was used in the analyses.
We assessed cardiorespiratory fitness by the 6-min walk test.27In this test,the maximum distance(in meters)each participant could walk during 6 min along a 45.7-m rectangular course was recorded.27
Positive affect and negative affect were assessed by the Trait Positive and Negative Affect Schedule.29This questionnaire includes questions on 10 positive and 10 negative emotional states that are answered on a 5-point Likert scale,from 1(very slightlyORnot at all)to 5(extremely).Scores can range from 10 to 50 for both subscales(positive affect and negative affect),and higher scores reflect greater affective well-being.The scales have been shown to be highly internally consistent,largely uncorrelated,and stable in a 2-month period in the adult population.29The time frame adopted was“in general”(i.e.,participants were asked to report how they feel“in general,that is,on the average”).
Anxiety levels were assessed with the STAI-T.30The total score ranges from 20 to 80,with higher values indicating greater levels of anxiety.The STAI-T is one of the most commonly validated self-report questionnaires used to evaluate anxiety in pregnant women.30To measure trait(dispositional)anxiety,participants answer questions such as,“How do you usually feel?”
Pregnant antenatal depression among the participants was assessed using the CES-D.31The revised CES-D,which includes 35 items,was used.However,we calculated the overall score using only 20 items because this is the most accepted calculation method across the literature.The CES-D has been validated and is widely employed in pregnancy studies.31In regard to reliability,Chronbach’sαwas 0.90,with similar coefficients by groups of age and sex and by interviewer.31The CES-D uses the last 7 days as the time frame.
The TMMS32includes 3 subscales to assess participants’beliefs about attending to and valuing their feelings(emotional attention),feeling clear rather than confused about their feelings(emotional clarity),and the degree to which they regulate their moods and repair negative emotional experiences(emotional regulation).Each subscale includes 8 items.The participants rate their responses using a 5-point Likert-type scale,ranging from 1(strongly disagree)to 5(strongly agree).The subscales’scores range from 8 to 40,where higher scores reflect greater attention,clarity,and regulation.The Spanish modified version of the TMMS had appropriate reliability and has been shown to be valid.32Participants were asked to use an“in general”time frame.
The 10-item Connor-Davidson Resilience Scale assesses resilience to stress.33This construct refers to a dynamic process of positive adaptation to adverse changes in life circumstances.Each item’s score ranges from 0(not true at all)to 4(true nearly all the time).The total score ranges from 0 to 40,and higher scores indicate greater resilience.The Spanish version of the 10-item Connor-Davidson Resilience Scale showed good psychometric properties in young adults;thus,it is a reliable and valid instrument for measuring resilience.33Participants were asked to use an“in general”time frame.
An initial self-report survey was used to collect sociodemographic and clinical data,such as,age,educational level(low educational(primary or high school),medium educational level(professional training),and high educational level(universities studies)),and number of miscarriages.Fully trained researchers provided the participants with continuous instructions on how to complete the self-report.Additionally,low back pain was assessed using the Pain Visual Analogue Scale.34This score is determined by measuring the distance(mm)on the 10-cm line between the“no pain”anchor and the participant’s mark,providing a range of scores from 0 to 100.Body weight and height were measured while participants were in their bare feet and wearing underclothes.Weight(kg)was measured with an electronic scale(Seca 861;Seca GmbH& Co.,Hamburg,Germany),and height(cm)was measured with a stadiometer(Seca 225;Seca GmbH&Co.).Body mass index was expressed as kg per square meter.
2.4.Data analysis
All analyses were performed using the SPSS Statistics for Windows(Version 22.0;IBM Corp.,Armonk,NY,USA;withpset at<0.05).Descriptive statistics(mean±SD)for quantitative variables and number of women(%)for categorical variables)were used to describe the baseline characteristics of the participants.First,we explored the association of the potential confounders(e.g.,body mass index)with the mental health outcomes.Number of miscarriages and low back pain were the 2 most strongly correlated confounders to the mental health outcomes.We conducted multiple linear regression analyses with PA,sedentary time,and physical fitness measures as independent variables(predictors)and mental health components(i.e.,psychological well-being and psychological ill-being)as dependent variables(outcomes).Each set separately examined the relationships between 1 predictor and 1 mental health outcome.The linear regression analyses were hierarchically adjusted for 2 different groups of confounders.Model 1 included age,educational level,and accelerometer wear time(only in the case of PA and sedentary time variables).Model 2 was additionally adjusted for number of miscarriages and low back pain.
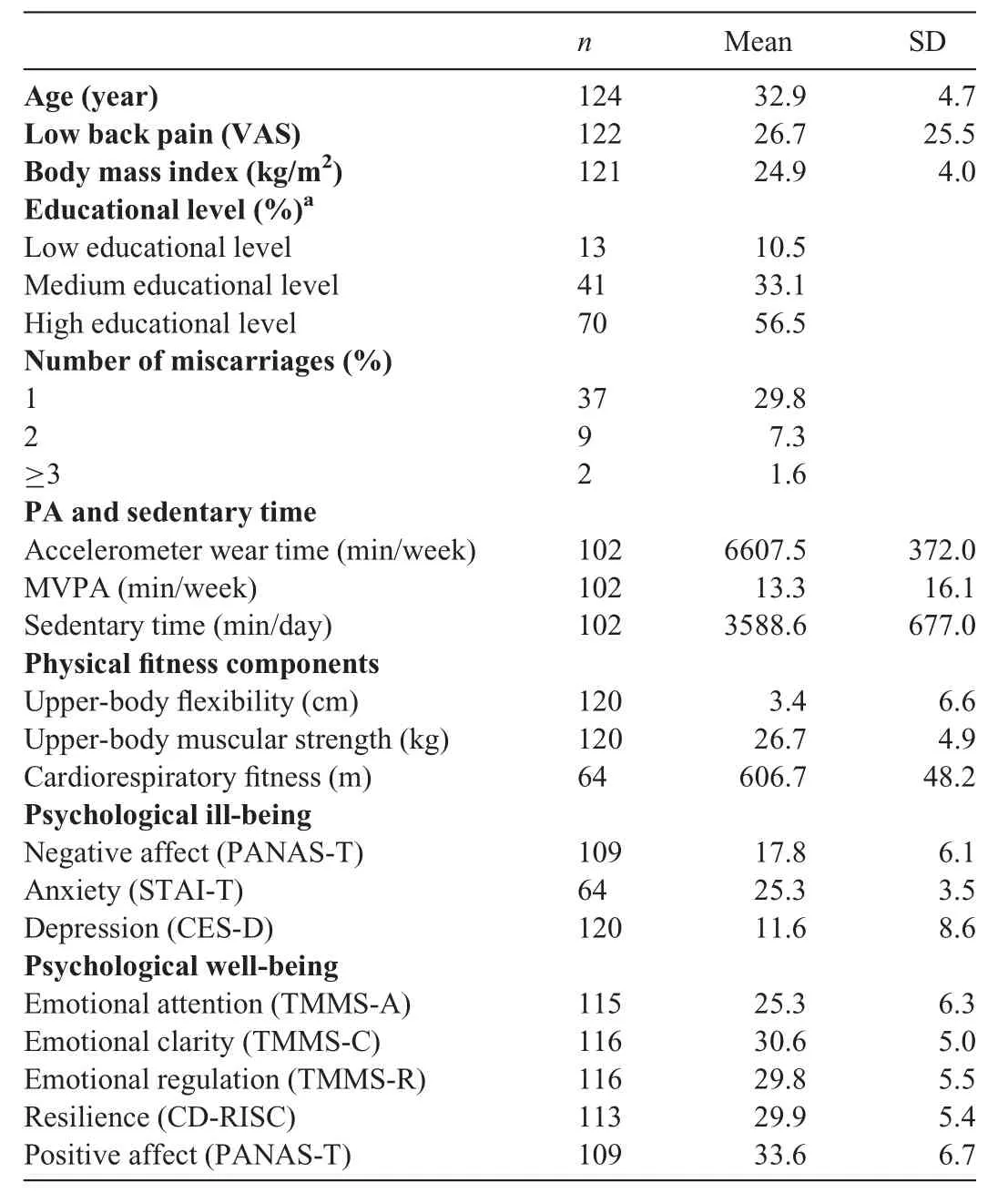
Table 1Sociodemographic and clinical characteristics of the study participants.
3.Results
The descriptive characteristics of the final study sample are presented in Table 1.Briefly,29.8% of the pregnant women had at least 1 miscarriage in the past.Additionally,it was found that 56.5% of the women had a high educational level.Briefly,these results remained similar when only participants with no missing data were analyzed(n=51).
Associations of PA,sedentary time,and physical fitness with psychological ill-being indicators(i.e.,negative affect,anxiety,and depression)are shown in Table 2.MVPA was inversely associated with depression(β=-0.227,adjustedR2=0.060,p=0.035)when the model was adjusted for age,educational level,and accelerometer wear time(Model 1).After performing the analysis with Model 2,the association remained significant(β=-0.222,adjustedR2=0.050,p=0.041).The results were virtually the same when MVPA(in Model 2)was additionally adjusted for sedentary time(data not shown).No associations were found with the rest of the psychological ill-being outcomes(allp>0.05).
The associations found between PA,sedentary time,and physical fitness and psychological well-being indicators(i.e.,emotion regulation,resilience,and positive affect)are shown in Table 3.Sedentary time was inversely associated with positive affect(β=-0.255,adjustedR2=0.019,p=0.022)when the model was adjusted for age,educational level and accelerometer wear time(Model 1).Subsequently,when the number of miscarriages and low back pain were added to the model(Model 2),the association remained statistically significant(β=-0.260,adjustedR2=0.085,p=0.017).The results were virtually the same when sedentary time(Model 2)was additionally adjusted for MVPA(data not shown).Upper-body flexibility was positively associated with emotional regulation(β=0.195,adjustedR2=0.030,p=0.047)when the model was additionally adjusted by number of miscarriages and low back pain(Model 2).No associations were observed for the rest of the psychological well-being outcomes(allp>0.050).
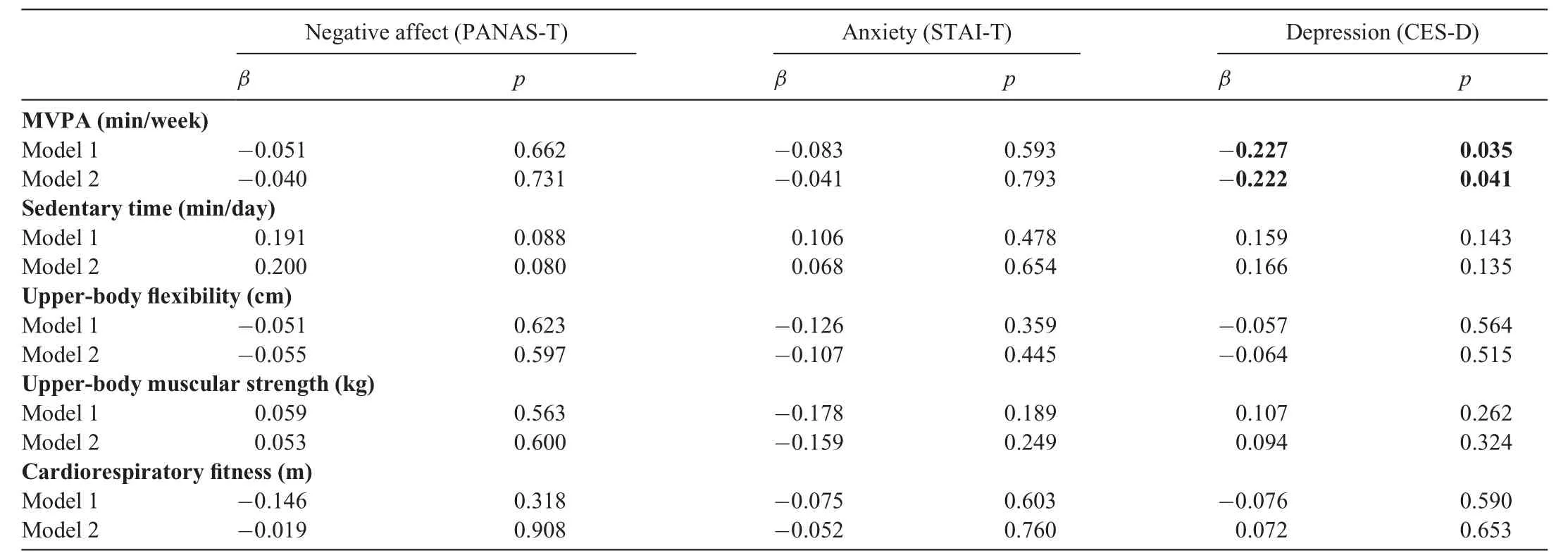
Table 2Associations of PA,sedentary time,and physical fitness with psychological ill-being in early pregnant women.
4.Discussion
The aim of the present study was to analyze the association of objectively measured PA,sedentary time,and physical fitness with psychological ill-being and well-being in early second trimester of pregnancy.The present study indicated that higher MVPA and lower sedentary time were modestly associated with lower depressive symptoms and higher positive affect,respectively,in the early second trimester of pregnancy.Furthermore,upper-body flexibility was positively associated with emotional regulation.Upper-body muscular strength and cardiorespiratory fitness were not related to mental health.
In line with the pregnancy literature,16,17the findings in the present study suggest that higher MVPA is associated with lower depressive symptoms in pregnant women.The crosssectional design of the present study does not allow us to rule out the possibility of a bidirectional association between MVPA and depressive symptoms in pregnancy,an association that remains unclear in the literature.For instance,another cross-sectional study found that obese pregnant women with lower depressive symptoms spent 85% more time in MVPA compared with women with higher depressed mood.35Other studies found that a lack of motivation or self-confidence was related to a worse attitude toward PA.36Interestingly,a 2-sample Mendelian randomization study observed that,in the general population,higher baseline MVPA was associated with lower depressive symptoms over time,although the reverse association did not emerge.37Similarly,a longitudinal study of pregnant women found that higher baseline MVPA(i.e.,17-22 weeks of gestation)predicted lower depressive symptoms in the 24-29 weeks of gestation.14This result14may be explained by the fact that MVPA might have a positive impact on depression by increasing endorphin levels and modulating the response to stress on the hypothalamic-pituitary-adrenal axis.38
A literature review suggests that pregnant women who more frequently engage in PA experience lower anxiety and mood disorders during pregnancy,17,18which was not corroborated in the present study.A plausible explanation for this discrepancy might lie in the fact that the present study and other studies used different approaches to evaluate PA:accelerometers in the present study(i.e.,an objective measure)and selfreports in other studies(i.e.,a subjective assessment).17For instance,previous studies have suggested that using methods with lower accuracy for assessing PA(i.e.,self-reports)often result in an overestimate of the time that a person engages in PA and tend to produce higher(potentially inflated)effect sizes when associations with health outcomes are tested.39Another possible explanation for the null findings might be that pregnant women in our sample experienced low levels of anxiety.Given that symptoms of anxiety fluctuate over the pregnancy(i.e.,the greatest anxiety is often experienced during the first and last trimesters40),further research in the second trimester of pregnancy is warranted to corroborate our findings.
In the present study,MVPA was not associated with psychological well-being during pregnancy.Although MVPA often boosts psychological well-being,12it also might have negative effects on psychological well-being in certain contexts and circumstances.41For instance,when people do not experience increased physical competence or perceived appearance(e.g.,by not gaining strength,not experiencing weight loss,or losing games all the time),PA has a negative influence on physical self-concept,which in turn may impact negatively on psychological well-being.41Therefore,a possible explanation for our nonsignificant findings may be that changes in perceived appearance42and perceived competence43during pregnancy might mediate the positive role that MVPA usually plays in psychological well-being.
It is well-known that increased levels of sedentary time during pregnancy are associated with poorer physical health,for example,the development of cardiometabolic complications.44However,there is little knowledge about the association between sedentary time and mental health during pregnancy.44In the present study,sedentary time was inversely associated with positive affect among women in the early second trimester of their pregnancies.No statistically significant results were obtained for the remaining mental health outcomes.Positive affect may buffer against the harmful consequences of exposure to a challenging life event such as pregnancy.45A possible mechanism for explaining this might be that sedentary activities(such as lying on the couch)can limit social interaction with others,which in turn can limit the possibilities of having positive emotional experiences.46
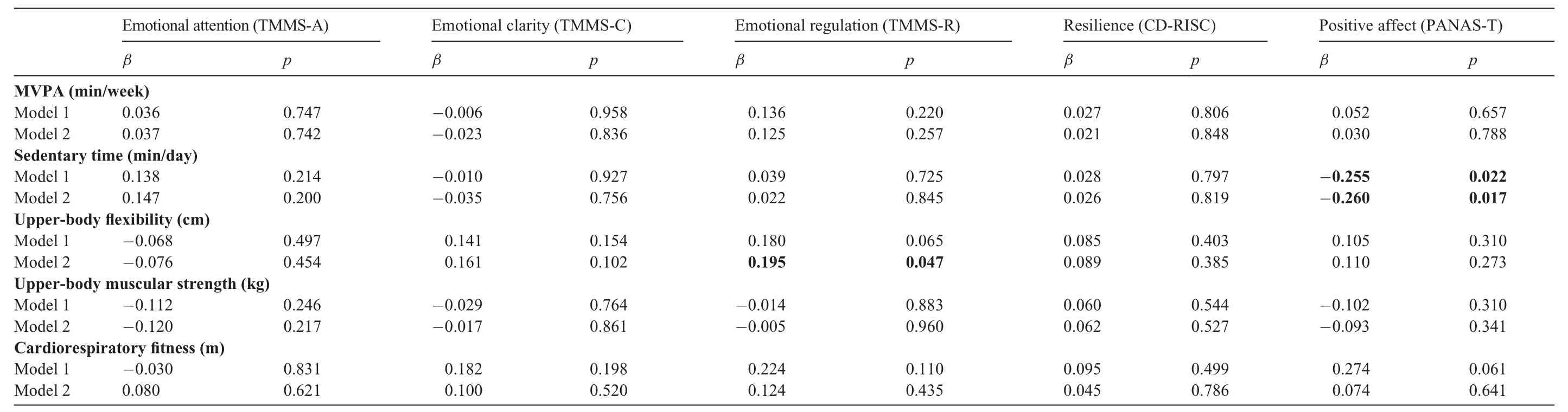
Table 3Associations of PA,sedentary time,and physical ftiness with psychological well-being in early pregnant women.
The current study found that better upper-body flexibility was associated with better emotional regulation(i.e.,how well moods are regulated and negative emotional experiences are repaired).To the best of our knowledge,the association between flexibility and psychological well-being indicators in pregnant women has not been explored previously.Consequently,although direct comparisons with other studies cannot be made,we speculate that changes in levels of relaxin,which is a neuropeptide that increases during pregnancy and is related to greater flexibility in joints and tissue,might be a possible physiological mechanism that explains our finding.47It has recently been suggested that relaxin is involved in regulating aspects of physiological and behavioral stress responses and the integration of sensory inputs.48Therefore,relaxin may be a physiological mechanism that explains why flexibility is related to better emotional regulation during pregnancy.In line with findings from other studies,flexibility seems to be a key player in the successful appraisal of stress,especially when stress is hardly avoidable,such as during pregnancy or chronic pain,and is consequently related to better mental health.49Surprisingly,although muscular strength and cardiorespiratory fitness are widely recognized as protectors of physical health(e.g.,abdominal adiposity,cardiovascular disease events,or skeletal health),13they were not related to mental health outcomes in the present study.Because this study is,to the best of our knowledge,the first to analyze the association of physical fitness with mental health in pregnant women,it is not possible to compare our results with previous studies.Thus,it is important to conduct observational studies and other research in this area.Consequently,if the present findings are corroborated in further experimental research,physical exercise programs might be developed to focus on enhancing flexibility to promote improvements in emotional regulation during pregnancy.
Our study has several limitations.First,given the cross-sectional design of the present study,future longitudinal and experimental research is warranted to address the causality of our findings.Second,the missing data in our study are another limitation,despite the fact that similar dropout rates have occurred in other studies of pregnant women.24,25Third,although the questionnaires used to assess mental health and the physical fitness tests in this study were valid and reliable for the general population,their psychometric properties have not been extensively tested among pregnant women,except for the STAI-T,whose validity has been previously corroborated at this stage of a woman’s life.30Fourth,psychological ill-being and well-being indicators were only reported during the second trimester of pregnancy.Given that psychological ill-being fluctuates during pregnancy,our findings are not generalizable to the first and third trimesters of pregnancy.Fifth,the effect sizes for the association of PA,sedentary time,and physical fitness with mental health seem to be small.To date,however,there is no well-established cutoff point for evaluating the clinical relevance of effect sizes in the context of mental health.Finally,the difference in the time frame for obtaining the accelerometry data and the mental health measures was approximately 1 week.
Despite these limitations,our present study has several strengths.First,we used objective measurements of PA,sedentary time,and physical fitness.Additionally,we studied not only psychological ill-being,but also psychological well-being,which provides a more comprehensive understanding of mental health among pregnant women.
5.Conclusion
This study has shown that greater MVPA and lower levels of sedentary time were modestly associated with less depressive symptoms and better positive affect,respectively.Furthermore,better upper-body flexibility was related to better emotional regulation.If the present findings are corroborated in further experimental research,an active lifestyle characterized by higher levels of MVPA and lower levels of sedentary time during pregnancy might improve the mental health of women in the early second trimester of pregnancy.In addition,physical exercise programs might be developed to focus on enhancing flexibility to promote improvements in emotional regulation during second trimester pregnancy.
Acknowledgments
The present study was developed within the GESTAFIT project framework,which is part of a Virginia A.Aparicio fellowship approved by the Andaluc′ıa Talent-Hub Program and co-funded by the European Union’s Seventh Framework Program,Marie Skłodowska-Curie actions(COFUND-Grant Agreement No.291780).This study was also partially funded by the Ministry of Health of the Junta de Andaluc′ıa(PI-0395-2016)and the University of Granada,Unit of Excellence on Exercise and Health(UCEES).Maria Rodriguez-Ayllon was supported by the Research Initiation Grants for Master’s Degree Students.Irene Coll-Risco and Milkana Borges-Cosic were supported by the Spanish Ministry of Education(Grant No.FPU14/02518 and Grant No.FPU13/01993,respectively).Fernando Est′evez-L′opez was supported by the Spanish Ministry of Economy and Competitiveness(Grant No.BES-2014-067612).We are grateful to Ms.Carmen Sainz Quinn for English-language assistance.
Authors’contributions
MRA had full access to all of the data in the study,took responsibility for the integrity of the data and the accuracy of the data analyses,conceptualized and designed the study,collected and interpreted the data,and drafted the initial manuscript;PAM,ICR,LRG,and MBC conceptualized and designed the study,collected and interpreted the data.FEL and VAA conceptualized and designed the study,and interpreted the data.All authors were involved in drafting the article and revising it for important intellectual content.All authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
 Journal of Sport and Health Science2021年3期
Journal of Sport and Health Science2021年3期
- Journal of Sport and Health Science的其它文章
- A critical review of national physical activity policies relating to children and young people in England
- The evidence for the impact of policy on physical activity outcomes within the school setting:A systematic review
- State laws governing school physical education in relation to attendance and physical activity among students in the USA:A systematic review and meta-analysis
- Handgrip strength and health outcomes:Umbrella review of systematic reviews with meta-analyses of observational studies
- Is device-measured vigorous physical activity associated with health-related outcomes in children and adolescents? A systematic review and meta-analysis
- Conceptual physical education:A course for the future Charles B.Corbin