
Handgrip strength and health outcomes:Umbrella review of systematic reviews with meta-analyses of observational studies
2021-05-22 00:27PinarSoysalChristophrHurstJaopoDmurtasJosphFirthRubnHownLinYanMarTullyAiKoyanaiPtrCristianIliGuillrmoopzanhz
Pinar Soysal,Christophr Hurst,Jaopo Dmurtas,Josph Firth,Rubn Hown,Lin Yan,Mar A.Tully,Ai Koyanai,Ptr Cristian Ili,Guillrmo F.L′opz-S′anhz,
Lukas Schwingshackll,Nicola Veronesem,*,Lee Smithn,*
a Department of Geriatric Medicine,Bezmialem Vakif University,Istanbul 34093,Turkey
b Institute of Neuroscience,Newcastle University,Newcastle upon Tyne NE1 7RU,UK
c Primary Care Department,Azienda Usl Toscana Sud Est,Grosseto 52100,Italy
d Division of Psychology and Mental Health,University of Manchester,Manchester M13 9PL,UK
e College of Health&Human Services,University of North Carolina at Charlotte,Long Beach,CA 90815,USA
f Department of Cancer Epidemiology and Prevention Research,Alberta Health Services,Holy Cross Centre,AlbertaT5J 3E4,Canada
g School of Health Sciences,Institute of Mental Health Sciences,Ulster University,Newtownabbey BT15 1ED,UK
h Research and Development Unit,Sant Joan de D′eu Health Park,CIBER of Mental Health(CIBERSAM),Barcelona 08003,Spain
i ICREA,Pg.Lluis Companys 23,Barcelona 08010,Spain
j The Queen Elizabeth Hospital King’s Lynn NHS Foundation Trust,King’s Lynn PE30 4ET,UK
k Faculty of Sport Sciences,University of Murcia,Murcia 30100,Spain
l Institute for Evidence in Medicine,Medical Center-University of Freiburg,Faculty of Medicine,University of Freiburg,Freiburg 79085,Germany
m Neuroscience Institute,Aging Branch,National Research Council,Padua 35122,Italy
n The Cambridge Centre for Sport and Exercise Sciences,Anglia Ruskin University,Cambridge CB1 1PT,UK
Abstract Purpose:The aim of the present study was to assess both the credibility and strength of evidence arising from systematic reviews with meta-analyses of observational studies on handgrip strength and health outcomes. Methods:An umbrella review of systematic reviews with meta-analyses of observational studies was conducted.We assessed meta-analyses of observational studies based on random-effect summary effect sizes and their p values,95% prediction intervals,heterogeneity,small-study effects,and excess significance.We graded the evidence from convincing(Class I)to weak(Class IV). Results:From 504 articles returned in a search of the literature,8 systematic reviews were included in our review,with a total of 11 outcomes.Overall,nine of the 11 of the outcomes reported nominally significant summary results(p<0.05),with 4 associations surviving the application of the more stringent p value(p<10-6).No outcome presented convincing evidence.Three associations showed Class II evidence(i.e.,highly suggestive):(1)higher handgrip values at baseline were associated with a minor reduction in mortality risk in the general population(n=34 studies;sample size=1,855,817;relative risk=0.72,95%confidence interval(95%CI):0.67-0.78),(2)cardiovascular death risk in mixed populations(n=15 studies;relative risk=0.84,95%CI:0.78-0.91),and(3)incidence of disability(n=7 studies;relative risk=0.76,95%CI:0.66-0.87). Conclusion:The present results show that handgrip strength is a useful indicator for general health status and specifically for early all-cause and cardiovascular mortality,as well as disability.To further inform intervention strategies,future research is now required to fully understand mechanisms linking handgrip strength scores to these health outcomes.
Keywords:Handgrip strength;Health outcomes;Meta-analysis;Umbrella review
1.Introduction
A decline in physical function is a natural phenomenon that is associated with aging.1Such a decline is a public health concern because it has been shown to be associated with increased risk of falls,2health care use,3level of dependency,4and premature mortality.5Indeed,for many independent older adults,everyday tasks,such as climbing stairs,require functioning close to maximal capacity,meaning that further decline could increase their risk of becoming dependent on a carer.6One widely employed measure of physical functioning is handgrip strength.The handgrip strength test is commonly used to evaluate the integrated performance of the muscles by determining the maximal grip force that can be produced in 1 muscular contraction,which further serves as a marker for general muscle strength.7Handgrip strength is a valid measure of physical function and has been widely employed in observational research and clinical settings.8-11Importantly,1 study found that dynamometer-determined handgrip strength could be a useful instrument in geriatric practice to identify the“oldest old”patients(i.e.,those aged over 75 years)at risk of disability.12
In recent years there has been an exponential increase in the literature investigating associations between handgrip strength and health outcomes(e.g.,depression,13cognitive function,14suicidal ideation,15mobility limitations,16falls,17cardiovascular disease,18diabetes,19renal outcomes,20osteoporotic factors,21multimorbidity,22and mortality23);consequently,there has been an increase in systematic reviews with meta-analyses.However,to date,most systematic reviews have focused on a single disease end-point,and there has not been a systematic evaluation of the relationships between handgrip strength and diverse physical and mental health outcomes.Moreover,the strength and reliability of the evidence presented in the literature is unclear.
To address the breadth of the literature of physiological measurements and outcomes,an increasing emphasis has been placed on“umbrella reviews”(i.e.,the syntheses of existing systematic reviews with meta-analyses in order to capture the breadth of outcomes associated with a given exposure).
Given this situation,the aim of the present study was to carry out an umbrella review of existing systematic reviews with meta-analyses of handgrip strength and all health outcomes in order to systematically assess the quality and strength of the evidence across all health outcomes and to identify those studies with the strongest evidence.
2.Methods
This umbrella review was registered in PROSPERO:
https://www.crd.york.ac.uk/PROSPERO/display_record.php?RecordID=158547.
2.1.Data sources and searches
We conducted an umbrella review24by first searching several databases(MEDLINE,Scopus,and Embase)from inception until 20 November 2019.The following search terms were used:(“meta-analysis”[ptyp]OR“metaanaly*”[tiab]OR“meta-analy*”[tiab]OR“systematic review”[ptyp]OR“systematic review”[tiab])AND“handgrip”[tiab]).In addition,we hand-searched the reference lists of eligible articles.
2.2.Study selection
In this umbrella review,we included systematic reviews and/or meta-analyses of observational studies that investigate the relationship between handgrip strength and any health outcome.Specific inclusion criteria included the following:(1)meta-analyses or systematic reviews containing sufficient data for a meta-analysis(as defined by the authors)that measured handgrip strength and ascertained health outcomes using selfreport(e.g.,depression questionnaires),observed(e.g.,clinical diagnoses),or objective(e.g.,biomarkers and mortality)criteria;(2)case control studies or cohort studies(retrospective and prospective cohorts);and(3)meta-analyses of cohort studies that investigated the association between handgrip strength with any health-related outcome(e.g.,cardiovascular disease,cancer,death,obesity/overweight,mental illness,diabetes,and metabolic diseases).Studies had to report these outcomes as odds ratio,relative risk(RR),hazard ratio,or continuous data.Two authors(PS and CH)independently performed title and abstract screening in couples.Disagreements were resolved through consensus with another independent author(LS).
2.3.Data extraction
Four independent investigators(PS,LS,CH,and NV)extracted in pairs the following information for each article:first author name,year of publication,journal,the number of included studies and the total number of participants included in the studies reviewed,the inclusion criteria for the studied populations,the measures by which handgrip strength was captured,how handgrip strength was categorized,the effect sizes used in the review,the subgroupings used in the metaanalysis,the study design(case control,retrospective,and prospective),the number of cases and controls for each study,and health outcomes.
We then extracted the study-specific estimated RR for health outcomes(RR,odds ratio,hazard ratio,standardized mean difference),along with the 95% confidence interval(95%CI),and the number of cases for each study by subjects and controls.If 2 reviews covered the same association,we included the review with the largest number of studies.
2.4.Risk of bias assessment
Two authors(PS and CH)independently rated the methodological quality of the included systematic reviews using“A MeaSurement Tool to Assess systematic Reviews 2(AMSTAR 2)”,25,26which ranks the quality of a meta-analysis in one of 4 categories ranging from“critically low”to“high”according to 16 predefined items.The review is ranked as high quality if it has no or 1 noncritical weakness(the systematic review provides an accurate and comprehensive summary of the results of the available studies that address the question of interest).The review is ranked as moderate quality if it has more than 1 noncritical weakness(the systematic review has more than 1 noncritical weakness but no critical flaws;it may provide an accurate summary of the results of the available studies that were included in the review).The review is ranked as low quality if it has 1 critical flaw with or without noncritical weaknesses(the review has a critical flaw and may not provide an accurate and comprehensive summary of the available studies that address the question of interest).Finally,the review is ranked as critically low quality if it has more than 1 critical flaw with or without noncritical weaknesses(the review has more than 1 critical flaw and should not be relied on to provide an accurate and comprehensive summary of the available studies).26For further reading relating to the AMSTAR 2 and what constitutes a critical flaw or a critical weakness,and so on,we refer the reader to the following reference.26
2.5.Statistical analysis
For each meta-analysis,we estimated the summary effect size and its 95%CI through random-effects models.27We also estimated the prediction interval and its 95%CI,which further accounts for between-study effects and estimates the certainty of the association if a new study addresses that same association.28Between-study association was estimated with theI2metric;values of 50%or greater are indicative of high heterogeneity,while values above 75% suggest very high heterogeneity.29
In addition,we calculated the evidence of small-study effects(i.e.,whether small studies would have inflated effect sizes compared to larger ones).To this end,we used the regression asymmetry test developed by Egger and co-workers.30Apvalue of less than 0.10,with more conservative effects in larger studies than in random-effects meta-analysis,was considered as indicative of small-study effects.21Finally,we applied Ioannidis’s excess of significance test to evaluate whether there was an excess of studies reporting statistically significant results.31
2.6.Grading the evidence
We used the credibility assessment criteria,which are based on established tools for observational evidence as summarized previously.24,32-35We classified evidence from meta-analyses of observational studies with nominally statistically significant summary results(p<0.05)into 4 categories(Classes I,II,III,and IV).Associations were considered to be convincing(Class I)if they had(1)a statistical significance ofpvalue of less than 10-6,(2)included more than 1000 cases(or more than 20,000 participants for continuous outcomes),(3)had the largest component study reporting a significant result(p<0.05),(4)had a 95% prediction interval that excluded the null,(5)did not have large heterogeneity(I2<50%),and(6)showed no evidence of small study effects(p>0.10)or of excess significance bias(p>0.10).Highly suggestive(Class II)evidence was assigned to associations that(1)reported a significance ofpvalues of less than 0.001,(2)included more than 1000 cases(or more than 20,000 participants for continuous outcomes),and(3)had the largest component study reporting a statistically significant result(p<0.05).Suggestive(Class III)evidence was assigned to associations that reported a significance of apvalue of less than 0.01 with more than 1000 cases(or more than 20,000 participants for continuous outcomes).Weak(Class IV)evidence was assigned to the remaining significant associations with apvalue of less than 0.05.
Due to the inherent limitations of case control studies in examining temporal associations,we had planned to provide the classification of evidence for Class I and Class II based on the following order:(1)meta-analyses of prospective studies and(2)meta-analyses of prospective and retrospective case control studies.However,no outcome had these characteristics.
3.Results
3.1.Literature review
Our search identified 20 potentially eligible reviews.Of the 20 reviews,eight were deemed to be eligible for our umbrella review.The 8 reviews had 11 different outcomes that were included in our umbrella review.
3.2.Meta-analyses of observational studies
The median number of studies of meta-analyses that included observational studies for each outcome was 8(range 4-34),the median number of participants was 23,064(range 2775-1,855,817),and the median number of cases was 1823(Table 1).
The majority of the meta-analyses included studies on the general population or in adults older than 50 years,followed by patients with cardiovascular disease.Overall,nine of the 11 outcomes reported nominally significant summary results(p<0.05),with 4 associations surviving to the application of the more stringentpvalue(p<10-6)(Table 1).Heterogeneity among studies was high in nine of the 11 of the outcomes included,with seven having anI2of 75% or greater.Only 2 associations presented 95% prediction intervals excluding the null value.Evidence for excess statistical significance was present in five of 41 outcomes,and small-study effects were seen in three of 11 outcomes.Bias was present in three of the outcomes included.The largest study,in terms of participants for each outcome,was statistically significant in all the associations,except one.
Based on the above criteria,no outcome presented convincing evidence.However,3 associations showed Class II evidence(i.e.,highly suggestive):higher handgrip values at baseline,were associated with a minor reduction in mortality risk in the general population(n=34 studies;sample size=1,855,817;RR=0.72,95%CI:0.67-0.78);cardiovascular death in mixed populations(e.g.,diabetes,general,and other conditions)(n=15 studies;RR=0.84,95%CI:0.78-0.91),and incidence of disability(n=7 studies;RR=0.76,95%CI:0.66-0.87)(Table 1).The other outcomes were ranked as suggestive(association between higher handgrip values and chair rise performance over time)or weak(5 outcomes),with only 2 associations not statistically significant(i.e.,the association between handgrip strength and incident hip fracture or cancer mortality)(Table 1).
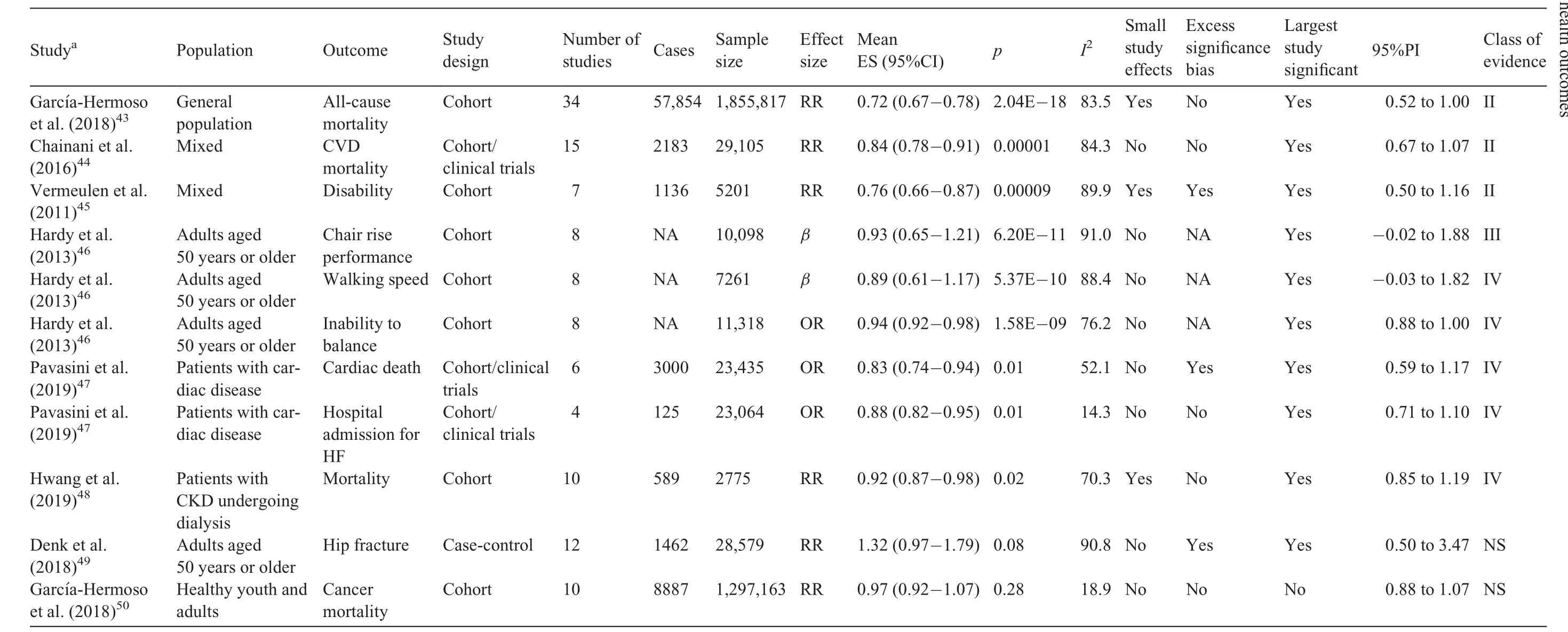
Table 1Health outcomes and evidence class reported in included meta-analyses of observational studies.
3.3.Quality assessment
Based on scores derived from using the AMSTAR 2 tool,a total of four of the meta-analyses included in our review scored“critically low”and four scored“low”(Supplementary Table 1).Notably,most studies did not include a list of excluded studies(n=8)or report the source of funding for the included studies(n=7).Moreover,it should be noted that 1 study did not include a systematic review.
4.Discussion
In this umbrella review of 8 meta-analyses and 11 health outcomes investigating associations between handgrip strength and all health outcomes,a total of 3 outcomes(lower all-cause mortality,lower cardiovascular mortality,and lower risk of disability)were found to have highly suggestive evidence.One outcome(chair rise performance over time)was found to have suggestive evidence.Five outcomes(walking speed,inability to balance,hospital admissions,cardiac death,and mortality in those with chronic kidney disease)were found to have weak evidence.Importantly,2 associations were found to be nonsignificant(incident hip fracture and cancer mortality).Taken together,these findings suggest that handgrip strength is a useful indicator for general health status,early all-cause mortality,cardiovascular mortality,disability,and leg power(chair rise performance).
Several mechanisms may explain the relationship between handgrip strength and early mortality.First,early life factors,such as participation in sufficient levels of physical activity,influence handgrip strength,36and childhood levels of physical activity and handgrip strength have been shown to track into adulthood.37,38Importantly,maintaining adequate levels of physical activity and function over the entire life course likely yields the greatest benefit to health,owing to the reduction of any prolonged exposure from unhealthy behaviors.Next,strength is related to muscle mass and muscle mass is used a protein reserve during cases of trauma.39Finally,other genetic contributions may be at play that result in muscle dystrophy and early mortality.40
When considering the relationship between handgrip strength and disability and leg power,this may be explained by sarcopenia(a progressive reduction in muscle strength and mass,absolute and relative to body size,commonly occurring with aging).41Sarcopenia is associated with a decline in physical function and an increase in disability.8Next,the handgrip strength test is not just a pure measure of strength;and those with joint disorders,who will likely have increased risk of disability and lower leg power,may perform worse when carrying out this task.8
Umbrella reviews provide top-tier evidence and important insights,but there are a number of limitations to our review that should be considered.The meta-analyses contained studies that differed in their designs,populations,and other characteristics.However,we applied anI2of less than 50%as one of the criteria for Class I evidence(convincing)to assign the best evidence grade only to robust associations.Next,meta-analyses have inherent limitations:42their findings depend on which estimates are selected from each primary study and how they are applied in the meta-analysis.Finally,all the meta-analyses included in our review scored low or critically low when appraised through the use of the AMSTAR 2 tool,suggesting that future meta-analyses in this area will require more accurate reporting of methods and will also need to incorporate more robust discussions around findings.
5.Conclusion
Our results show that handgrip strength is a useful indicator for general health status,early all-cause mortality,cardiovascular mortality,disability,and leg power(chair rise performance).Future research is needed to fully understand the mechanisms linking handgrip strength scores to these health outcomes and further inform intervention strategies.
Authors’contributions
PS,CH,NV,and LeeS conceived the idea,wrote the protocol,extracted the data,analyzed the data,and wrote the original draft;JD,JF,RH,LY,MAT,AK,PCI,GFLS,and LS contributed to the protocol and the drafting of the manuscript.All authors have read and approved the final version of the manuscript,and agree with the order of the presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
Supplementary materials
Supplementary material associated with this article can be found in the online version at doi:10.1016/j.jshs.2020.06.009.
 Journal of Sport and Health Science2021年3期
Journal of Sport and Health Science2021年3期
- Journal of Sport and Health Science的其它文章
- A critical review of national physical activity policies relating to children and young people in England
- The evidence for the impact of policy on physical activity outcomes within the school setting:A systematic review
- State laws governing school physical education in relation to attendance and physical activity among students in the USA:A systematic review and meta-analysis
- Is device-measured vigorous physical activity associated with health-related outcomes in children and adolescents? A systematic review and meta-analysis
- Conceptual physical education:A course for the future Charles B.Corbin
- The impact of the coronavirus disease 2019 pandemic on physical activity in U.S.children