
Mediation role of cardiorespiratory fitness on the associat ion between fatness and cardiometabolic risk in European adolescents:The HELENA study
2021-05-22 00:27CarlosCrstMonteroJaverCourelnezFransoOrteaJoseCastroneroAlaSantalestraPasasAnelaPoltoeremyVanelstAsensonMarosLusMorenoJonatanRuzonealfofteHELENAstuyroup
Carlos Crst-Montero,Javer Courel-I′a~nez,Franso B.Ortea,Jose Castro-P~nero,Ala Santalestra-Pasas,Anela Polto,J′er′emy Vanelst,Asens′on Maros,Lus M.Moreno,Jonatan R.Ruz,on ealf of te HELENA stuy roup
a IRyS Group,Physical Education School,Pontificia Universidad Cat′olica de Valparai′so,Valparai′so 2530388,Chile
b Department of Physical Activity and Sport,Faculty of Sport Sciences,University of Murcia,Murcia 30071,Spain
c PROmoting FITness and Health through Physical Activity Research Group(PROFITH),Department of Physical Education and Sports,Faculty of Sport Sciences,University of Granada,Granada 18001,Spain
d Department of Physical Education,Faculty of Education Sciences,University of C′adiz,Puerto Real 11003,Spain
e Department of Health and Human Performance,School of Health Sciences,University of Zaragoza,Zaragoza 50001,Spain
f Growth,Exercise,Nutrition and Development(GENUD)Research Group,Zaragoza 50001,Spain
g National Institute for Food and Nutrition Research,Rome 80070,Italy
h Lille Inflammation Research International Center,University of Lille,Lille 59000,France
i Immunonutrition Research Group,Department Metabolism and Nutrition,Institute of Food Science and Technology and Nutrition(ICTAN),Spanish National Research Council(CSIC),Madrid E-28040 Spain
Abstract Purpose:This study was aimed to analyze the mediation role of cardiorespiratory fitness(CRF)on the association between fatness and cardiometabolic risk scores(CMRs)in European adolescents. Methods:A cross-sectional study was conducted in adolescents(n=525;46%boys;14.1±1.1 years old,mean±SD)from 10 European cities involved in the Healthy Lifestyle in Europe by Nutrition in Adolescence study.CRF was measured by means of the shuttle run test,while fatness measures included body mass index(BMI),waist to height ratio,and fat mass index estimated from skinfold thicknesses.A clustered CMRs was computed by summing the standardized values of homeostasis model assessment,systolic blood pressure,triglycerides,total cholesterol/highdensity lipoprotein cholesterol ratio,and leptin. Results:Linear regression models indicated that CRF acted as an important and partial mediator in the association between fatness and CMRs in 12-17-year-old adolescents(for BMI:coefficients of the indirect roleβ=0.058(95% confidence interval(95%CI):0.023-0.101),Sobel test z=3.11(10.0% mediation);for waist to height ratio:β=4.279(95%CI:2.242-7.059),z=3.86(11.5% mediation);and for fat mass index:β=0.060(95%CI:0.020-0.106),z=2.85(9.4%mediation);all p<0.01). Conclusion:In adolescents,the association between fatness and CMRs could be partially decreased with improvements to fitness levels;therefore,CRF contribution both in the clinical field and public health could be important to consider and promote in adolescents independently of their fatness levels.
Keywords:Cardiovascular disease;Children;Fat mass;Fitness;Health;Physical activity
1.Introduction
Obesity in adolescents has increased dramatically in recent decades and has reached worldwide pandemic proportions.1Obese youths are likely to become obese adults and are at higher risk of developing cardiovascular diseases(CVD),dyslipidemia,and type 2 diabetes,2,3which together constitute the main cause of death in adults.4Both unhealthy dietary behaviors and physical inactivity5seem to be the key determinants of obesity in youth;thus,early interventions for preventing the development of obesity-related CVD are needed not only for present health but also for future health.
To date,there has been no absolute clarity regarding the reverse or bidirectional relationship(cause-effect-response)between obesity and physical inactivity because the direction of causality cannot be inferred from cross-sectional associations.6,7There is evidence from longitudinal studies that shows reciprocal associations and synergistic interactions among fatness with motor skill competence,physical activity,and cardiorespiratory fitness(CRF).8-10In contrast,there are other studies that show that fatness leads to inactivity in children.6,7These circumstance expose the ambiguity of the scientific literature in this matter and the need to investigate the interaction between fatness and fitness.
Of note is that physically inactive adolescents have lower CRF levels;11,12and,in turn,this physiological marker is crucial for attenuating the association between fatness and increased cardiometabolic risk from childhood to adolescence.13Hence,nowadays there is a special focus on improving CRF,14especially in obese adolescents.15
An interesting approach to studying the role and importance of a variable over the association between others is mediation analysis,which can determine whether a predictor variable in an outcome is mediated through an intermediate variable(mediator).16This innovative method has been applied in studies of children to examine the mediator role of obesity in the relationship between CRF and cardiometabolic risk17and inflammation.18The authors of these studies reported that,when including body mass index(BMI)as a mediator,the association between CRF and cardiometabolic risk disappears completely in girls and is considerably mitigated in boys.17These results do not fully support the“fat-but-fit”paradigm,which suggests that a person with excess adiposity but with a high CRF(fat-fit phenotype)has a better cardiometabolic profile than a person with excess adiposity but with a low CRF.13,19Accordingly,the role of fitness and fatness as mediators of cardiometabolic health still needs to be clarified,especially in children and adolescents.19
Based on the assumption that fatness leads to inactivity,the purpose of this study was to analyze the mediation role of CRF on the association between fatness markers and cardiometabolic risk scores(CMRs)clustering in European adolescents and to analyze the magnitude of CRF mediation in this relationship.We hypothesized that CRF would only partially mediate the relationship between fatness and CMRs.This investigation contributes to the field of public health by providing evidence about the bidirectional relationship between obesity and CRF.
2.Methods
The Healthy Lifestyle in Europe by Nutrition in Adolescence(HELENA)cross-sectional study was designed to obtain reliable and comparable data on nutrition and health-related parameters from a sample of adolescents aged 12.5-17.5 years from 10 European cities in 9 countries.Data collection took place between 2006 and 2008.A sample of 3528 adolescents met the HELENA general inclusion criteria(age of 13.00-16.99 years,schooling in one of the 10 European cities,informed consent signed,had at least weight and height measured,and completed at least 75% of the other tests).20In the present study,525 adolescents(54%girls)with valid data on the main variables and covariates were included in the analysis:cardiometabolic risk factors,including total cholesterol to high-density lipoprotein cholesterol ratio(TC/HDL-C),triglycerides(TG),homeostasis model assessment(HOMA),and systolic blood pressure(SBP);as well as leptin,CRF,age,sex,pubertal stage,and center(city involved in the study from each country).This subsample was representative to the total sample(assuming an error of 5%,a confidence interval(CI)of 95%,and 50% of heterogeneity).Moreover,there were no differences between the present subsample and the whole sample(boys and girls separately)in terms of age,body mass,height,and BMI(allp>0.05).
The study was performed following the ethical guidelines of the 1964 Declaration of Helsinki(revision of Edinburgh 2000),Good Clinical Practice,and legislation regarding clinical research in humans in each of the participating countries.The protocol was approved by the Human Research Review Committees of the involved centers.Furthermore,all parents and guardians signed an informed consent form,and the adolescents agreed to participate in the study.20
2.1.Physical examination
Adolescents participating in the study were barefoot and dressed in light clothing during anthropometric measurements.Body weight was measured to the nearest 0.1 kg with an electronic scale(Seca 861;Seca GmbH & Co.,Hamburg,Germany),and body height was measured with a telescopic stadiometer(Seca 225;Seca GmbH & Co.)to the nearest 0.1 cm.BMI was calculated as body weight divided by the square of height(kg/m2).21Waist circumference(WC)was measured with a non-elastic tape(Seca 200;Seca GmbH &Co.)to the nearest 0.1 cm.Waist to height ratio(WHtR)was then calculated by dividing WC(cm)by height(cm).Bicipital,tricipital,subscapular,and suprailiac skinfold thicknesses on the left side of the body were measured with a Holtain Calliper(Holtain Ltd.,Crymych,Wales,UK)to the nearest 0.2 mm.All the anthropometric measurements were taken 3 times and the mean was scored.22Percentage of body fat was calculated using the equation of Slaughter et al.,23which has proven to be the most suitable equation for use with adolescents.24Fat mass(kg)was estimated by multiplying body fat percent by weight(kg)and dividing by 100,and fat-free mass(kg)was calculated as the difference between body weight and fat mass.Fat mass index(FMI)was determined by dividing fat mass(kg)by height squared(m2).Identification of pubertal maturation(Stages I-V)was assessed by direct observation by a medical doctor,according to Tanner and Whitehouse.25SBP was measured(OMRON®M6,HEM 70001;Omron,Kyoto,Japan)following the recommendations for adolescent populations,26with participants seated in a separate quiet room for 10 min with their backs supported and feet on the ground.Two SPB readings were taken at 10-min intervals,and the lowest measure was recorded.
2.2.Blood samples
Blood samples were collected as previously described.27TG,TC,and HDL-C were measured using enzymatic methods(Dade Behring,Schwalbach,Germany).All blood parameters were measured after an overnight fast.HOMA index calculation was used as a measure of insulin resistance28using the formula HOMA-index=(insulin(μUI/mL)×glucose(mg/dL))/405.The ratio of TC/HDL-C was also calculated.Leptin concentrations were measured by the RayBio(RayBiotech Inc.,GA,USA)Human Leptin enzyme-linked immunosorbent assay.Leptin assay sensitivity was set at less than 6 pg/mL,with intraclass and interclass coefficients of variation of less than 10% and less than 12%,respectively.29
2.3.CRF
CRF was measured by the progressive 20-m shuttle run test.The test has high validity and reliability in adolescents(test-retest reliability coefficients were 0.89;standard error of estimation was 5.9 mL/kg/min).30,31In the shuttle run test,participating adolescents ran between 2 lines 20 m apart,while keeping the pace with audio signals emitted from a pre-recorded CD with an initial speed of 8.5 km/h and increasing by 0.5 km/h every minute(1 min equals 1 stage).The test ended either when the adolescent failed to reach the end line concurrent with the audio signals on 2 consecutive occasions or when he or she stopped owing to fatigue.The last stage completed(precision of 0.5 stages)was used to calculate the maximal oxygen consumption from the equation developed by L′eger et al.30
2.4.CMRs
A summative cardiometabolic risk index that includes several factors has proven to be a better marker of cardiovascular health in children than an index that only includes a single risk factor.29CMRs were created from the sum of SBP,TG,TC/HDL-C ratio,HOMA,and leptinz-scores.The standardized value(z-scores)of each variable was calculated as follows:(value-mean)/SD,separately for boys and girls,and for each 1-year age group.Lower values are indicative of a better profile.32This risk profile has been used previously in a cross-sectional study of 1732 randomly selected 9-year-old and 15-year-old school children from 3 European countries and in 2015.33Andersen et al.32confirmed that the composite risk score improved substantially in a sample of 15,794 youths aged 6-18 years that included the HOMA index rather than fasting glucose,leptin,the sum-of-4-skinfolds(instead of BMI or WC),and CRF.Both the sum-of-4-skinfolds and CRF were removed from this CMRs because these were part of the mediation analysis and could have generated a methodological bias.
2.5.Statistical analysis
The normality of the distribution of the variables was tested using both statistical(Kolmogorov-Smirnov test)and graphical methods(normal probability plot).Adolescents’characteristics are presented as the mean±SD and the frequency(%)for continuous and categorical variables,respectively.The Studentttest and the Pearson’sχ2test were used to test sex differences in relation to adolescents’CRF,fatness(BMI,WHtR,and FMI),and cardiometabolic biomarkers(TC/HDL-C,TG,HOMA,SBP,and leptin)and pubertal stage.Partial correlation coefficients(r),adjusted for age,sex,pubertal stage,and center,were used as a preliminary analysis to examine the associations between CRF,cardiometabolic,and fatness biomarkers.
Multicollinearity was tested before completing the mediation analysis through tolerance value and variance inflation factors.34,35We analyzed the mediation role of CRF on the association of 3 fatness markers(BMI,WHtR,and FMI)with CMRs through bootstrapped(10,000 samples)linear regression analyses36using the PROCESS SPSS script,16adjusted for age,sex,pubertal stage,fat-free mass,and center.Each model included 3 equations.
Equation 1 regressed the mediator(CRF)on the independent variable(BMI,WHtR,and FMI).Equation 2 regressed the dependent variable(CMRs)on the independent variable(BMI,WHtR,and FMI).Equation 3 regressed the dependent variable(CMRs)on both the independent(BMI,WHtR,and FMI)and the mediator variable(CRF),and Equation 3′took into account the indirect(mediating)role.We calculated the percentage of the total contribution that is accounted for by mediation using the standardized coefficients of the Equation 1×Equation 2/Equation 3.A significant“indirect role”(mediation)was established when(a)the independent variable was significantly related to the mediator,(b)the independent variable was significantly related to the dependent variable,(c)the mediator was significantly related to the dependent variable,and(d)the association between the independent and dependent variable(“direct role”)was attenuated when the mediator was included in the regression model.37The Sobel test was used to test the hypothesis that the indirect role was equal to 0.38Point estimates and 95% confidence intervals(95%CIs)were estimated for the indirect role.Complete mediation was established when the independent variable(fatness)was not associated with the dependent variable(CMRs)after mediator(CRF)has been controlled,making path Equation 3′zero.Partial mediation is when the path from fatness to CMRs is reduced in absolute size but is still different from 0 when the mediator is introduced.The percentage of mediation was calculated as 1-(Equation 3′/Equation 3)where Equation 3 is the role for the independent variable in predicting the main outcome and Equation 3′is the role of the independent variable in predicting the dependent variable with the mediator variable.Analyses were completed using the IBM SPSS(Version 21.0;IBM Corp.,Armonk,NY,USA).The level of significance was set atp<0.05.
3.Results
Table 1 shows the characteristics of the sample.The partial correlations coefficients between the fatness variables,CRF,and cardiometabolic biomarkers are presented in Table 2.There was no difference in the CMRs between sex(p=0.992)when both boys and girls were grouped.CRF was negatively associated with all the study measures of fatness as well as with cardiometabolic biomarkers(p<0.05),except for SBP.BMI,WHtR,and FMI were associated positively with all cardiometabolic biomarkers(p<0.05).We observed no multicollinearity.The tolerance value ranged between 0.829 and 0.888 for collinearity tolerance and the variance inflation factor ranged between 1127 and 1206 for collinearity.
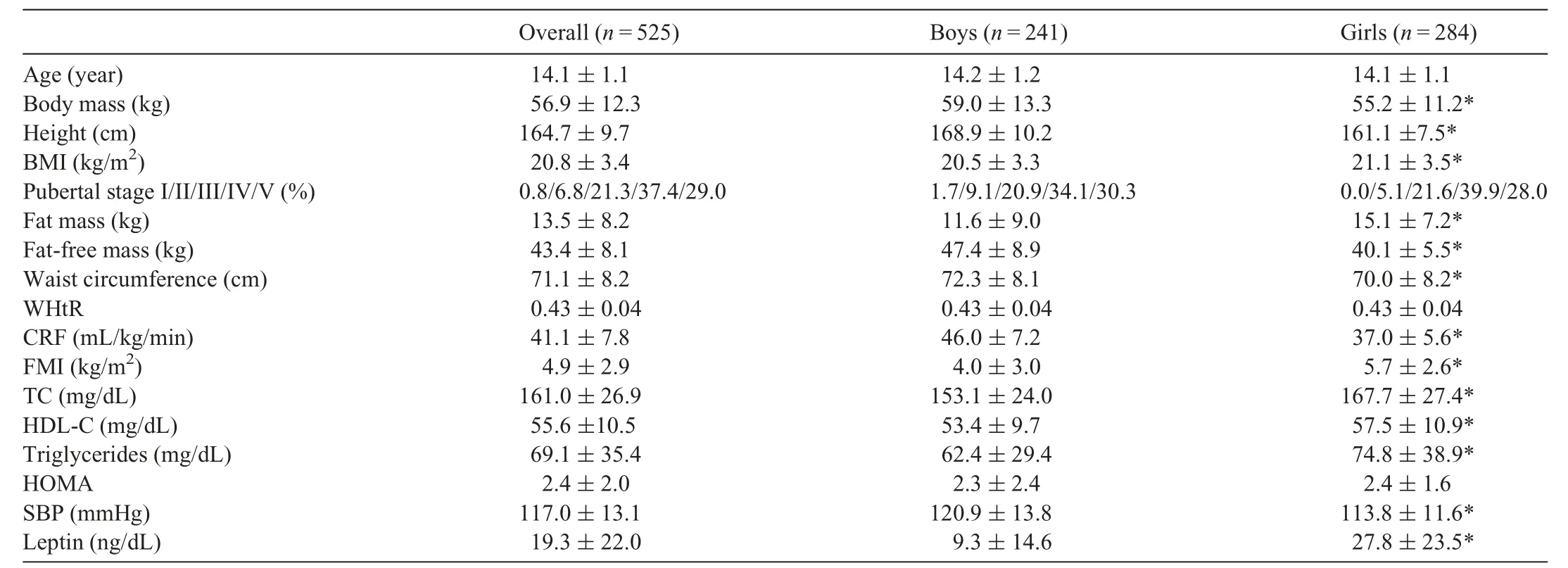
Table 1Characteristics of adolescents.
The results from mediation analysis are shown in Fig.1.Overall,fatness(BMI,WHtR,and FMI)was positively associated with CMRs.Mediation analysis including CRF revealed that the association between fatness and CMRs was mediated via CRF.The role of this mediation adjusted for potential confounders accounted for around 10%.More precisely,CRF mediates 10.0% of CMRs for BMI(z=3.11;indirect role=0.058(95%CI:0.023-0.101);p=0.001),11.5% for WHtR(z=3.86;indirect role=4.279(95%CI:2.242-7.059);p<0.001),and 9.4% for FMI(z=2.85;indirect role=0.060(95%CI:0.020-0.106);p=0.004)parameters.
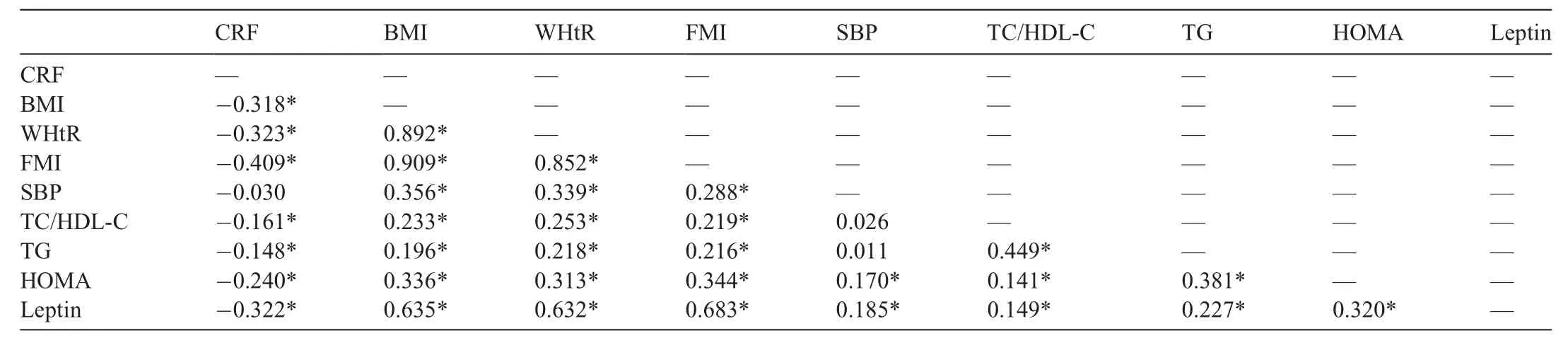
Table 2Partial correlations coefficients(r)among fatness,CRF,and cardiometabolic biomarkers.
4.Discussion
The main findings of the current study indicate that CRF acts as a partial mediator in the association between 3 different fatness variables and clustered CMRs in European adolescents.Therefore,although it is true that CRF is an important health biomarker,it does not seem to completely counteract the negative role of fatness on cardiometabolic health.To our knowledge,this is one of the few studies that have used CRF as a mediator,39,40and the first to establish the mediation role of CRF on the relationship between fatness and cardiometabolic risk in European adolescents.

Fig.1.Mediation analysis.Contribution of fatness on CMRs through CRF,adjusting for potential confounders(age,sex,pubertal stage,center,and fat-free mass).BMI=body mass index;CMRs=cardiometabolic risk scores;CRF=cardiorespiratory fitness;FMI=fat mass index;WHtR=waist to height ratio.
The evidence shows a close relationship among fatness,low CRF,and cardiometabolic health in youths.41-43Thus,CRF and obesity as predictors of CVD should be monitored to identify children and adolescents with potential CVD risk.44,45Despite the importance of both markers on cardiometabolic health,mediation analysis studies have frequently used fatness as a mediator,17,18,46assuming a possible unique association way(physical inactivity as causal of fatness).However,there is also literature showing otherwise.6,7Thus,looking at the 2 sides of the coin seems to be adequate for achieving a broader and objective understanding of this problem to improve the effectiveness of intervention programs in this population.
The results of the present mediation analysis show that CRF is capable of partially attenuating the association between fatness and a cluster of cardiometabolic risk factors in adolescents.In this sense,the magnitude of the mediation of CRF could support—up to a point—the fat-but-fit hypothesis,19,47because a high level of CRF would not fully protect the independent action of fatness(BMI,WHtR,and FMI)on cardiometabolic risk in adolescents.However,the independent and beneficial role of high CRF may indeed offset more of the fatness risk than indicated by the mediator analysis—just by mechanisms not related to fatness.It should be noted that this mediation role is around 10% for the 3 fatness variables studied in this approach,which gives it an important role both in public health strategies and for clinical purposes.
This outcome is in line with previous prospective research reporting that in schoolchildren(aged 7-11 years)the association of CRF with change in CVD risk factor levels after adjustment for adiposity(total body fat,BMI,and WC)was less strong and concluding that the association of CRF with CVD risk factors was largely explained by adiposity.48Another study of schoolchildren(aged 10-14 years)showed that children with low fitness levels had increased odds of presenting both individual and clustered cardiometabolic risk factors,but these associations no longer remained after adjusting for abdominal adiposity.49The authors suggested that abdominal adiposity may be a more important determinant of adverse cardiometabolic health in this age group,49and especially in obese children.15,50Notwithstanding the foregoing,childhood CRF seems to decrease the long-term(20-year follow-up of 1792 adults)cardiometabolic risks associated with childhood obesity.51Therefore,more studies exploring the symbiotic interaction between fatness and CRF on cardiometabolic health are warranted to establish insight into the bidirectional causality between these variables.6,7
The physiological interpretation of these findings is complex because fatness and CRF are separately and independently associated with cardiometabolic risk factors,52possibly exerting their effects through different causal pathways.53,54For example,obesity may result in the development of a chronic,low-grade inflammatory state caused by an increased expression of pro-inflammatory adipokines and diminished expression of anti-inflammatory adipokines.54Moreover,obesity has been associated with elevated oxidative stress,which can lead to endothelial dysfunction.55It has also been related to a decrease in oxygen respiration in skeletal muscle associated with an impairment of mitochondrial function.56
Each condition mentioned(chronic low-grade inflammatory state,diminished antioxidant capacity,and decrease in oxygen respiration in skeletal muscle)can be improved or even reversed,to some extent,by adequate levels of physical activity and exercise54-56and by enhancing CRF.19,47,57A meta-analysis showed that high-intensity interval training seems to be more effective for improving cardiometabolic risk and CRF than other forms of exercise in overweight and obese youth.58High-intensity activities,particularly among adolescents,seems to be more effective in reducing a clustered metabolic syndrome for both fit and unfit individuals.39However,our results contribute to the existing evidence by suggesting that if younger individuals maintain adequate CRF levels,this can play a protective role that partially counteracts the harmful role of obesity.6,7,48-50
This work has some important strengths,such as the size of the European sample used(multicentric study)and the use of high-quality harmonization methods.It also seems to be the first study that has used CRF as a mediator to analyze CRF’s role in relation to a cluster of cardiometabolic risk factors in adolescents.However,this study also has certain limitations.The present mediation analysis should be interpreted as exploratory given the cross-sectional nature of our study;thus,it does not allow conclusions about the causality relationships to be drawn.Future longitudinal and experimental studies are needed to confirm our results.
Although it is true that CRF was measured with a validated and reliable test,this variable depends heavily on body weight.This situation could lead to underestimations of CRF values in people with overweight and obesity59and underestimate the benefit of the fat-but-fit hypothesis.60Moreover,the use of clustered CMRs is specific to the study sample,and each factor is equally weighted in predicting future disease.Finally,the sample used in this study was made up of relatively healthy youths,which could hamper the sensitivity in detecting associations.
5.Conclusion
CRF in adolescents seems to act as a significant and partial mediator of the relationship between fatness and CMRs,which supports,to a certain extent,the fat-but-fit paradigm.These results suggest that the independent role of CRF is associated with other mechanisms that are not directly linked to fatness.However,these findings also indicate that maintaining adequate CRF levels among adolescents can counteract the development of harmful obesity-related CVDs and thus is an important public health strategy.
Acknowledgments
We thank the adolescents who participated in the study and their parents and teachers for their collaboration.We also acknowledge the HELENA study members involved in fieldwork for their efforts.The HELENA project was supported by the European Community 6th Framework Programme for Research and Technological Development(contract FOODCT-2005-007034).The data for this study were gathered under the aegis of the HELENA project,and further analysis was additionally supported by the Spanish Ministry of Economy and Competitiveness(Grants RYC-2010-05957 and RYC-2011-09011),the Spanish Ministry of Health:Maternal,Child Health and Development Network(Grants RD08/0072 and RD16/0022),the Fondo Europeo de Desarrollo Regional(MICINN-FEDER),and the University of Granada,Plan Propio de Investigaci′on 2016,Excellence Actions:Units of Excellence;Unit of Excellence on Exercise and Health(UCEES).The content of this article reflects the authors’views alone,and the European Community is not liable for any use that may be made of the information contained herein.
Authors’contributions
CCM and JRR had full access to all of the data in the study and took responsibility for the integrity of the data and the accuracy of the data analysis;CCM and JCI conceived and designed the study and drafted the manuscript;FBO,JCP,ASP,AP,JV,AM,LMM,and JRR carried out critical revisions of the manuscript for important intellectual content.All authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
 Journal of Sport and Health Science2021年3期
Journal of Sport and Health Science2021年3期
- Journal of Sport and Health Science的其它文章
- A critical review of national physical activity policies relating to children and young people in England
- The evidence for the impact of policy on physical activity outcomes within the school setting:A systematic review
- State laws governing school physical education in relation to attendance and physical activity among students in the USA:A systematic review and meta-analysis
- Handgrip strength and health outcomes:Umbrella review of systematic reviews with meta-analyses of observational studies
- Is device-measured vigorous physical activity associated with health-related outcomes in children and adolescents? A systematic review and meta-analysis
- Conceptual physical education:A course for the future Charles B.Corbin