
The effects of the COVID-19 pandemic on the physical activity of the Thai population:Evidence from Thailand’s Surveillance on Physical Activity 2020
2021-05-22 00:27PiyawatKatewongsaDyahAnantaliaWidyastariPairojSaonuamNarumolHaemathulinNarakornWongsingha
Piyawat Katewongsa,Dyah Anantalia Widyastari,Pairoj Saonuam,Narumol Haemathulin,Narakorn Wongsingha
a Institute for Population and Social Research,Mahidol University,Salaya,Phutthamonthon,Nakhon Pathom 73170,Thailand
b Thailand Physical Activity Knowledge Development Centre(TPAK),Institute for Population and Social Research,Mahidol University,Salaya,Phutthamonthon,Nakhon Pathom 73170,Thailand
c Healthy Lifestyle Promotion Section,Thai Health Promotion Foundation,Bangkok 10120,Thailand
Abstract Background:The coronavirus disease 2019(COVID-19)pandemic has undoubtedly disrupted the physical activity(PA)of the Thai population.This study examined the effect of the COVID-19 pandemic on moderate-to-vigorous PA(MVPA)of Thai adults and assessed the effects of the national curfew policy and health-promotion campaigns on influencing PA during the pandemic. Methods:Thailand’s Surveillance on Physical Activity(SPA)2019 and 2020 datasets were employed to compare the PA level of Thai adults aged 18-64 years before and during the COVID-19 pandemic.Samples of 4460 respondents from SPA 2019 and 4482 respondents from SPA 2020 were included in the analysis.Global Physical Activity Questionnaires(Version 2.0),were used to measure PA in both periods.Sufficient MVPA for adults was defined based on the recommendation of 75 min of vigorous PA or a combination of 150 min of MVPA per week. Results:The proportion of Thai adults who had sufficient MVPA declined from 74.6%before the pandemic to 54.7%during the pandemic,and that decline was accompanied by a reduction in the cumulative minutes of MVPA from 580 min to 420 min.During the COVID-19 pandemic,male and middle-aged individuals were 1.3 times and 1.2 times more likely to have sufficient MVPA,respectively.Those who were unemployed,resided in an urban area,and/or had chronic disease(s)were 27%,13%,and 27%less likely to meet the recommended level of PA during the pandemic,respectively.Those who were exposed to the Fit from Home campaign were 1.5 times more likely to have sufficient MVPA. Conclusion:The pandemic measures imposed by the government have reduced the cumulative min of work-related PA,transportation PA,and recreational PA and have slowed Thailand’s progress toward its PA goals.Although the Fit from Home campaign has probably contributed to a slight increase in MVPA,it will take some time for Thais to return to the pre-COVID-19 level of PA.Health promotion messages need to be continuously delivered to reduce irrational fear of infection and to boost the PA level of the Thai population as a health-promoting intervention.
Keywords:COVID-19 pandemic;Physical activity;Thailand
1.Introductio n
Thailand reported the first domestic case of the coronavirus disease 2019(COVID-19)on January 13,2020,1after a laboratory-confirmed infection of a traveler.The number of cases started to jump by mid-March2and increased continuously,which was attributed partially to nightclub and boxing stadium clusters.3Responding to the surge of cases,the Thai government followed the World Health Organization(WHO)recommendation for mitigating COVID-19 outbreaks by implementing aggressive measures to halt the infection.A curfew was imposed nationwide,starting on March 28,between the hours of 10 p.m.and 4 a.m.Non-essential businesses were shut down to encourage people to remain in their home neighborhoods and limit social contact.Public facilities that normally also serve as venues for physical activity(PA),including schools,offices,malls,and public parks,were closed,and mass gatherings were prohibited.
In addition to adapting to these stringent measures imposed by the government,the emergence of COVID-19 in Thailand imposed a strain on the entire society.Those in academia and the business sector were strongly recommended to work from home and advised to replace face-to-face interaction with online communication whenever possible.Ordinary community residents were also challenged to modify their leisure activities,such as dining out,leisure traveling,and outdoor PA,with home cooking,home entertainment,and home-based PA.This rather extreme response by the government and by many individuals in Thai society was incited by dramatic super-spreader events and the growing awareness that COVID-19 could be spread by asymptomatic carriers through airborne transmission when in close proximity to susceptible persons.3-5
It is reasonable to posit that PA can play a significant role in boosting the immune system and relieving stress during the COVID-19 pandemic.6-11Other things being equal,if a person is infected with COVID-19,the physically active person will have less severe symptoms and shorter recovery times and may be less likely to infect others.12PA is also beneficial for those who are asymptomatic or experiencing only mild symptoms because it improves the natural immune response to both the influenza and pneumococcal vaccines.12-14Therefore,staying fit during the pandemic has become a major healthpromotion message.Indeed,the Thai government has encouraged the population to stay active during the pandemic by promoting Fit from Home(FFH):Technique and Guidelines,which was issued by the Thai Health Promotion Foundation and released right after the partial lockdown policy was imposed.The FFH campaign was distributed nationwide through various channels,including print and online media,and it served as a guide for the Thai population in an effort to shift their outdoor PA into recommended home-based exercise,12,15,16such as brisk walking,stair climbing,yardwork and housework,and playing active games with the family.12FFH also provides sample videos of various training programs(i.e.,strength,balance,endurance,body weight)and includes activities such as running at home and biking at home.
Before the COVID-19 pandemic,the Thai government had been progressing toward a key milestone of its 5-Year National Non-communicable Diseases Prevention and Control Strategic and Action Plan(2017-2021):80% of the population would be“active”.17Thailand’s Surveillance on Physical Activity(SPA)survey reported that 74.4%of the country’s entire population and 78.4% of Thai adults were meeting the WHO 2018 recommendation of a cumulative 150 min of moderate or 75 min of vigorous PA per week,18,19whereas 26.2% of Thailand’s children and youth had a total of at least 60 min of moderate-to-vigorous PA(MVPA)daily.20However,the COVID-19 pandemic has undoubtedly slowed Thailand’s progress toward the PA target and perhaps even reversed the improving trend.By essentially being confined to their domiciles and immediate neighborhoods,individuals and families were faced with greatly restricted access to PA facilities.Furthermore,it can be expected that an increased percentage of society engaged more in sedentary activities due to the need to work from home(i.e.,sitting in front of a computer screen)or due to watching more TV or video entertainment than usual.
Several studies have examined the effects of COVID-19 on the PA of other countries’populations.21-23However,there are no published data comparing the levels and patterns of PA before and after the COVID-19 outbreak in Thailand.Thus,this study hopes to fill that void by comparing the PA level(prevalence of sufficient MVPA and average cumulative minutes of MVPA)prior to and during the pandemic in Thailand.Our study also documents the changes in the types and amount of PA among differing groups of the Thai population based on their sociodemographic characteristics.Second,this study assesses whether people exposed to the national campaign,FFH,had better PA outcomes during the pandemic.The results of our study provide the first evidence of the adverse effects of COVID-19 pandemic on PA as it pertains to Thailand,and this information should be beneficial for government officials and policymakers in formulating strategies for elevating the PA level of the population.
2.Methods
2.1.Study population and sample
This study employed Thailand’s SPA 2019 and 2020 datasets to compare the PA level of the Thai population before and during the COVID-19 pandemic.Conducted as an annual surveillance by the Institute for Population and Social Research—Mahidol University,and the Thai Health Promotion Foundation,SPA datasets have been used as the source of reference by the Thai government in formulating Thailand’s National Physical Activity Plans.The SPA 2019 employed a multistage,stratified random sampling to select a nationally representative sample by considering place of residence(urban or rural),gender,and age.Face-to-face interviews were conducted in 5 regions,13 provinces,and 36 villages and involved a total of 7333 people aged 5 years or older.However,to enable a comparison with SPA 2020,only 4460 adults aged 18-64 years who could access the Internet were included in the analysis.
With the confinement and restriction of movement during the COVID-19 pandemic,SPA 2020 was conducted as an online survey,and the population of interest was defined as all Thai adults who had access to an online system.The online method was also chosen because 85% of the Thai population has Internet access.Using data provided by the National Statistical Office,the online population was calculated,classified by province,and represented as a proportion of the actual Thai population.Probability random sampling was applied to draw the samples from Facebook pages.The research team randomly selected Facebook pages by district and invited Facebook users to join the survey by using a systematic random technique.Using the inclusion criteria of having a clear gender specification on the Facebook profile page and being 18-64 years of age,4482 individuals from the SPA 2020 sample were included in the analysis.
2.2.Data collection and measurements
To avoid differing environmental effects(i.e.,climate,season)in relation to PA,the data collection for both surveys was undertaken at approximately the same time of year,between March and May.Three different periods related to the COVID-19 pandemic were defined.SPA 2019 was employed to represent the unrestricted situation,that is,before the national curfew was imposed(March 28,2020).SPA 2020 constituted 2 periods:(1)the period during maximum curfew enforcement(from March 29 to May 2)and(2)during the relaxation of the curfew(after May 2).
Both SPA 2019 and SPA 2020 used the Global Physical Activity Questionnaire(Version 2.0)24to measure PA.Although different data collection methods were employed(face-to-face interviewsvs.online questionnaires,the same core questionnaire was used.The online questionnaires separated the sections by the following PA domains:work-related,transportation,and recreational,with additional questions about COVID-19.To help the online survey participants in understanding the questions,clarification and examples were provided as needed.The LimeSurvey web application(Carsten Schmitz,Hamburg,Germany)was used for SPA 2020 data collection.
As the dependent variable,PA was measured subjectively and expressed as(1)prevalence of sufficient MVPA and(2)accumulated minutes of MVPA.Weekly cumulative minutes of MVPA were calculated as a summation of all PA domains(work-related,transportation,and recreational)at both moderate and vigorous intensity.Sufficient MVPA was defined based on the WHO recommendation of an accumulation of 75 min of vigorous intensity or a 150-min combination of vigorous and moderate PA for adults.25
Gender,age,area of residence(urban or rural),education,occupation,having a chronic disease,and residence by type of epidemic zone(red,orange,or green)formed the independent variables for Objective 1 of the study:differentiating PA before and during the COVID-19 pandemic.Gender was dichotomized as(1)male or(2)female,and age was categorized into 2 groups:(1)young adult(18-39 years old)or(2)middle-age adults(40-64 years old).Education attainment was grouped into 3 levels:(1)lower and primary education,(2)secondary education,or(3)post-secondary education.Occupation was classified into 6 levels:(1)student,(2)formal sector,(3)informal sector,(4)private enterprise,(5)agriculture,or(6)unemployed.Type of resident was defined based on living in an(1)urban or(2)rural area,whereas residence by pandemic zone was categorized into(1)red,(2)orange,or(3)green.Receiving the FFH intervention was added to answer Objective 2 of the study:to assess national policy implementation during the pandemic,differentiated by 3 periods:(1)before the maximum curfew(BC),(2)during the maximum curfew(DC),and(3)after the maximum curfew was relaxed(AC).
The SPA received ethical approval from the Institute for Population and Social Research of Mahidol University Certificate of Ethical Approval(#COA2020/04-190),Institutional Review Board(#IRB0001007),Interoperability Review Group(#IORG0002101),and Federal Wide Assurance(#FWA00002882).In both face-to-face interviews and online surveys,all participants provided informed consent prior to their inclusion in the study.Participants in the face-to-face interviews signed the form,whereas online participants indicated their consent by ticking boxes provided after the information about the objectives of the study was given and after their right to join or withdraw from the research at their convenience was made clear.
2.3.Comparability of data and analysis
Although the SPA 2019 was representative of all Thais aged 5 years and older,in order to enable comparison with SPA 2020,only those who had Internet access and were 18-64 years of age were selected for analysis.To validate different instruments and ensure their measurability,the test-retest method was conducted with 30 cases in order to compare responses from the SPA 2019 face-to-face interviews with the self-reports from the online questionnaires used for SPA 2020.The overall correlation showed a value of 0.882,attesting to the validity of the questions for all population characteristics.A pairedttest was employed to evaluate individual items,and the results showed that there was no significant difference between the offline and online responses for all items of interest.Sampling bias was controlled by testing 2 samples that were included and excluded in the SPA 2019.
Descriptive statistics were presented to compare the sample characteristics in both surveys.Attest was employed to compare the cumulative minute of MVPA between SPA 2019 and SPA 2020,whereas anFtest was used to compare MVPA across study periods.Because the data were not normally distributed,multivariate analysis with binary logistic regression was used to determine factors associated with sufficient MVPA of the Thai population during the COVID-19 pandemic.All variables were included in the model,with a significance level of 0.005 or lower used to determine whether a variable had an effect on PA.
3.Results
3.1.Sample characteristics
The study sample comprised Thais aged 18-64 years,with a slight tendency toward younger adults among SPA 2020 respondents.The composition of the SPA 2019 sample was equal between genders,but the proportion of males in the SPA 2020 sample was higher than females(53.4% and 46.6%,respectively).The socioeconomic characteristics of the sample from both years varied;the majority of SPA 2020 respondents(79.1%)had attained a post-secondary education and were employed in the informal and formal sectors,whereas less than half(46.7%)of the SPA 2019 sample had a post-secondary education,and about 33% had only a primary-level education.Most of the respondents in the SPA 2019 sample worked in the formal or private sector.The proportion of the sample with chronic disease(s)was equal in both years(Table 1).
3.2.Changes in PA during the COVID-19 pandemic
The prevalence of sufficient MVPA among Thai adults decreased from 74.6% in SPA 2019 to 54.7% in SPA 2020(Fig.1A).The decrease in the prevalence was also accompanied by a reduction in the average cumulative minutes of MVPA from 580 min to 420 min(Fig.1A).The prevalence of sufficient MVPA was at its lowest during the DC period,when the Thai government imposed strict restrictions to contain the virus by closing public facilities,including public parks and gyms,and by prohibiting late-night travel.Although several measures were relaxed during the shorter curfew period,and there were limited facility openings,the prevalence of the sample with sufficient MVPA remained low,with only a slight increase during the AC period(Fig.1B).The restrictions were intended to contain the spread of the virus by limiting people’s movement,but they also adversely affected all types of PA.The results of thettest analysis suggest that there was a significant difference in the cumulative minutes of MVPA of Thai adults before and during the COVID-19 pandemic(t=11.864,p<0.001).TheFtest analysis also indicates that a significant difference in PA exists in two of 3 periods of the pandemic:BCvs.DC,and BCvs.AC(F=70.610,p<0.001)(Fig.1).
The cumulative minutes of work-related,transportation,and recreational PA also declined during the pandemic period(Fig.2).The detailed changes in the cumulative minutes of MVPA by sociodemographic characteristics,pandemic zones,and FFH intervention,classified by each type of PA(workrelated,transportation,or recreational)are available in Supplementary Table 1.
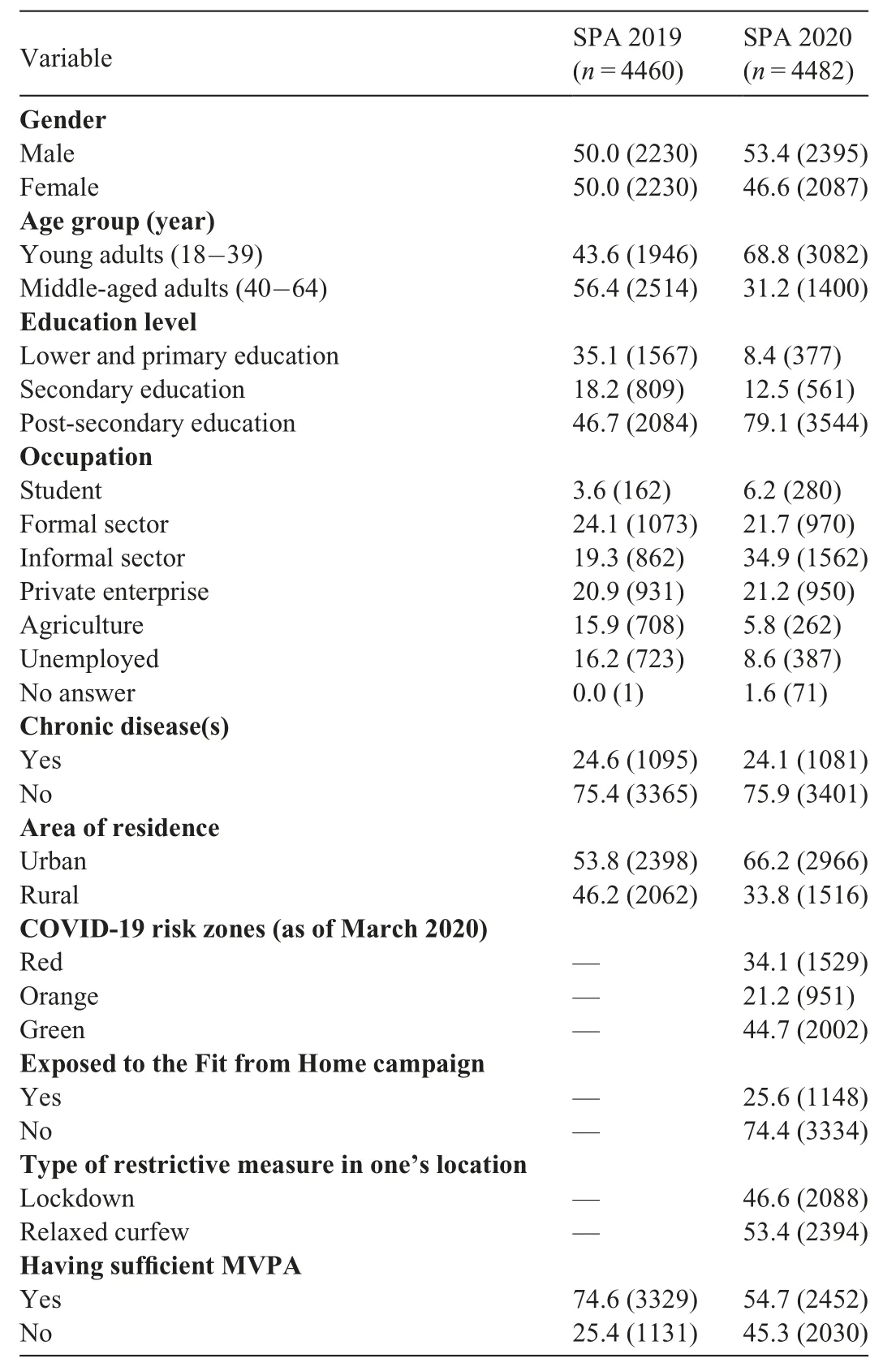
Table 1Demographic and other characteristics of participants in the Thailand’s SPA 2019 and SPA 2020.
The COVID-19 pandemic has affected the PA of the Thai population in both genders and all age groups.As was the case in the pre-pandemic period,Thai males accumulated a higher level of PA than their female counterparts during the pandemic(Table 2).Likewise,the proportion of middle-aged adults who had sufficient MVPA was consistently higher than that of the younger adults in both the pre-pandemic and the pandemic periods.The proportion of Thai adults who met the recommended level of MVPA was lowest among those who had completed their secondary education and were unemployed,whereas the highest proportion was found among agricultural workers and those with primary(SPA 2019)and post-secondary educations(SPA 2020).Surprisingly,the proportion of respondents with sufficient MVPA was slightly higher among those with chronic diseases in both years as compared to those without chronic diseases(Table 2).
Results of the multivariate analysis suggest that gender,age,occupation,the presence of chronic diseases,the area of residence,and exposure to the FFH campaign had statistically significant associations with MVPA sufficiency among Thai adults during the COVID-19 pandemic.When controlling for other factors,males were 1.3 times more likely to have sufficient MVPA during the pandemic compared to their female counterparts.Middle-aged adults were 1.2 times more likely to meet the recommended MVPA,whereas those residing in urban areas and having chronic diseases were 13% and 27%less likely to meet the recommended MVPA during the pandemic,respectively.Compared to individuals employed in the agricultural sector,those who were unemployed were 27%less likely to have sufficient MVPA(Table 3).
Given that behavior is influenced partly by knowledge,our study included the FFH campaign in the model as one of the interventions provided by the Thai Health Promotion Foundation.As one of the key findings of the study,the effect of the FFH campaign is evidenced by the higher proportion and greater likelihood of having sufficient MVPA(Table 3).Those who received the FFH techniques and guidelines were 1.5 times more likely to have sufficient MVPA compared to those who did not receive the information(Table 3).There was no significant effect on MVPA sufficiency by educational level or residence in or outside of an epidemic zone.Also,living in an area with a lockdown policy had no significant effect on sufficient MVPA of Thai adults.
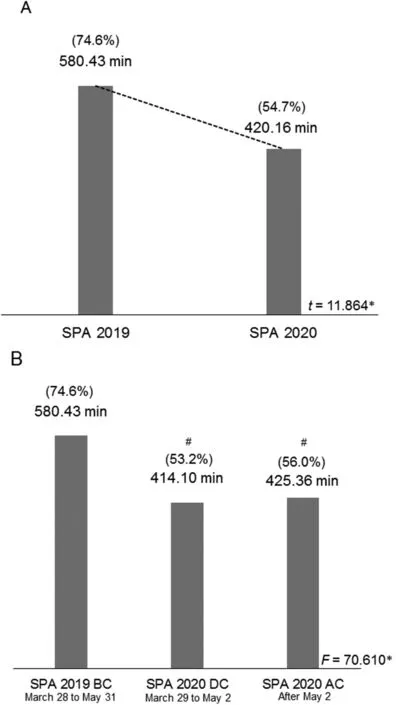
Fig.1.Differences in the physical activity of Thai adults before and during the COVID-19 pandemic:(A)percentage of sufficient MVPA and average cumulative minutes of MVPA per week;(B)percentage of sufficient MVPA and average cumulative minutes of MVPA per week classified by the period of COVID-19 pandemic.*p<0.001.compared with all groups;#p<0.001,compared with SPA 2019 BC.AC=after the maximum curfew was relaxed;BC=before the maximum curfew;COVID-19=coronavirus disease 2019;DC=during the maximum curfew;MVPA=moderate-to-vigorous physical activity;SPA=Surveillance on Physical Activity.
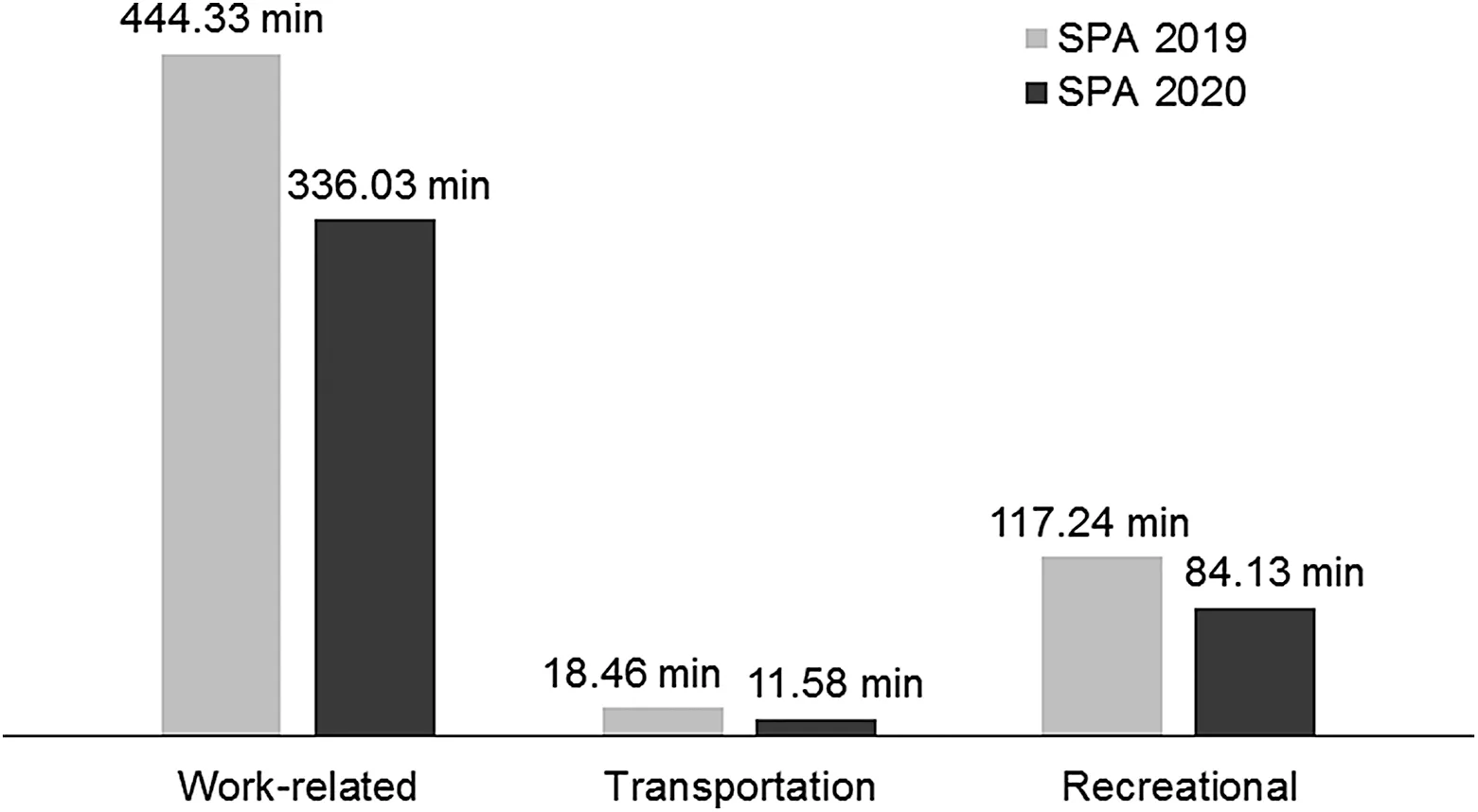
Fig.2.Average cumulative minutes of MVPA per week classified by type of PA.MVPA=moderate-to-vigorous physical activity;SPA=Surveillance on Physical Activity.
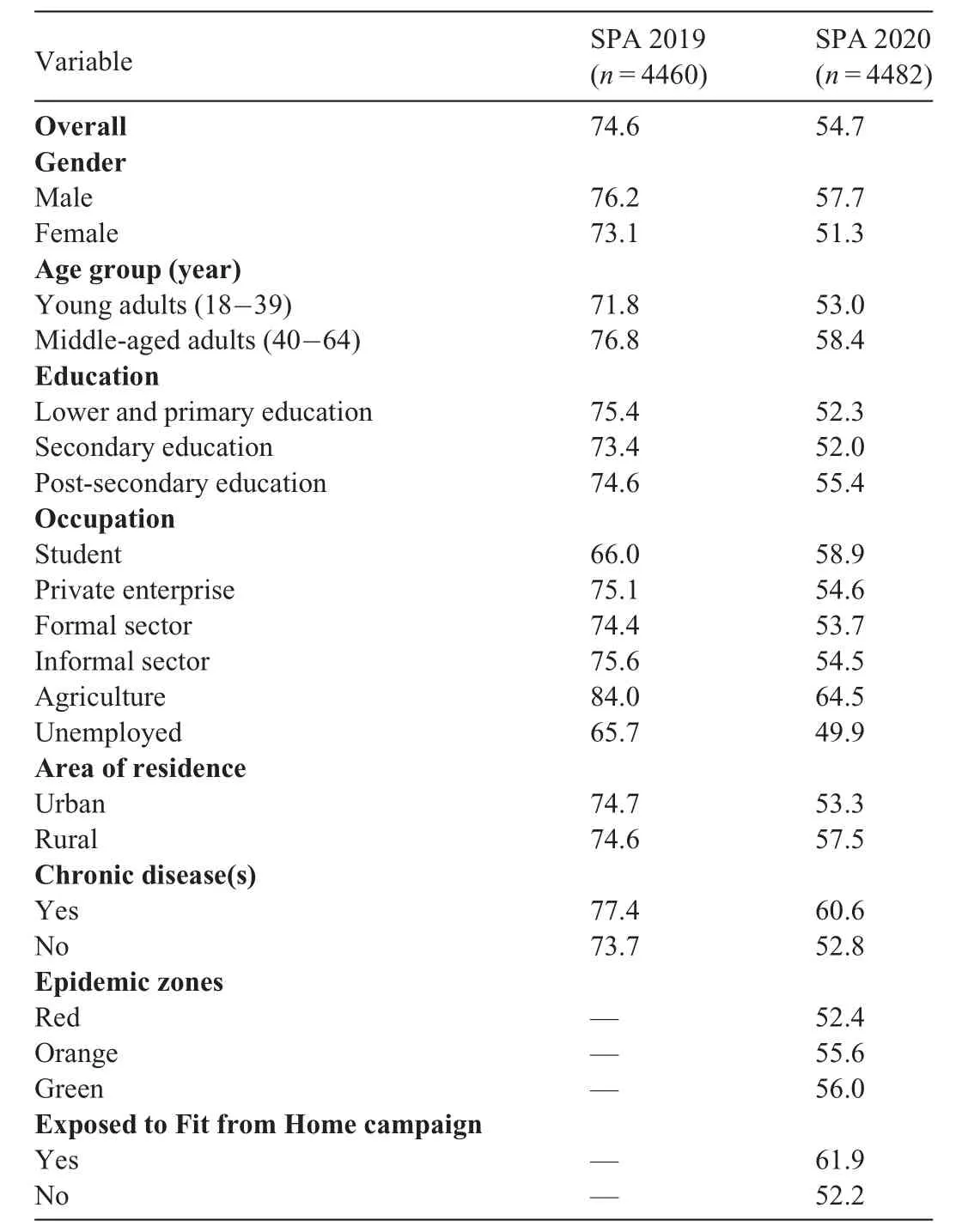
Table 2Percentage of Thai adults with sufficient MVPA(%).
4.Discussion
There is no doubt that the COVID-19 pandemic adversely affected the PA of the Thai population.PA was at its peak at the early stage of the COVID-19 pandemic and then began a decline as the government imposed several measures to contain the virus by restricting people’s movement in society at large.Schools,offices,and public facilities were closed so as to encourage people to stay at home from March 28 to May 2,2020;limited movement was allowed through July 1,2020.The fear of infection also motivated Thais to self-isolate by working from home and replacing face-to-face interactions with online socializing or teleconferencing.As a consequence,the cumulative min of PA for workrelated and transportation purposes declined because the majority of office work was performed at home.The closure of public parks,gyms,and other sports facilities also reduced the opportunity for Thais to engage in their regular recreational PA outside the home.
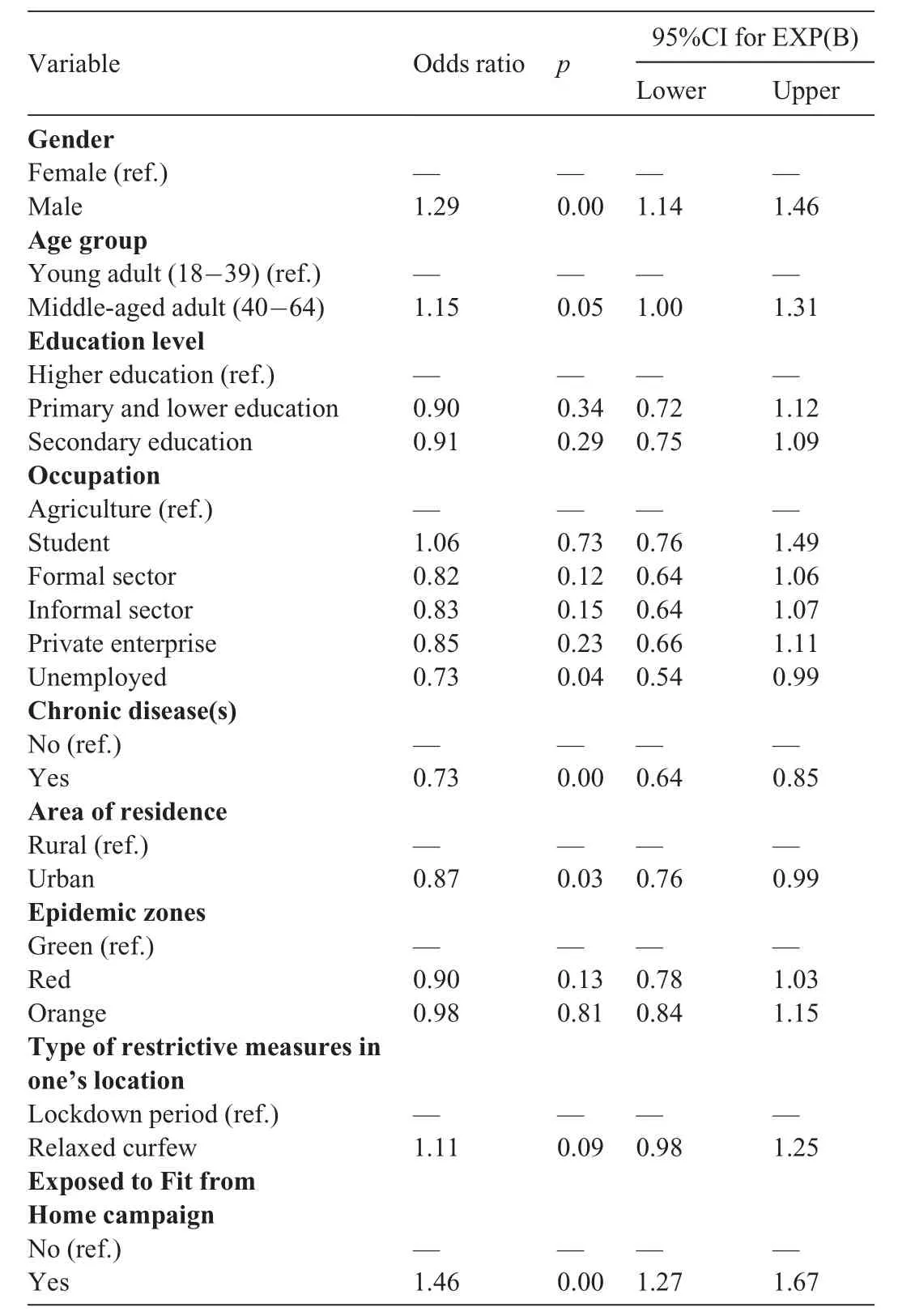
Table 3Determinants of sufficient MVPA of the Thai population during the COVID-19 pandemic.
It is also worth noting that,in the earliest stage of the pandemic,the government focused on containing the spread of the virus,and health promotion was relegated to a lower priority.Anticipating a prolonged period of restrictions,the Thai Health Promotion Foundation issued a series of guidelines(i.e.,FFH)about how to stay fit during the pandemic so as to help Thais maintain or regain good health status.Although the amount of MVPA slightly increased after the maximum curfew was relaxed,it remained lower than the level of MVPA before the COVID-19 lockdown.
Behavior theory suggests that a common emotional response to a pandemic is an exaggerated feeling of fear or anxiety.26-28Thus,persuading people that they need to engage in more PA may be difficult in the current environment.The boxing stadium cluster of COVID-19 infections(which was traced to a single super-spreader)has perhaps instilled a fear of mass gatherings to observe sports events or even engage in outdoor PA.Thus,it may take months or years for people to let their guard down and resume their pre-COVID-19 PA routine.On the other hand,although there has been a loosening of restrictions on movement and gradual reopening of public recreational facilities,the Thai government is being extremely cautious about the need to avoid a second outbreak.Although the Thai Ministry of Public Health has recommended social distancing of at least a 2-m radius,research suggests that running more than 2 m behind a(possibly infectious)person could still be dangerous because micro-droplets containing viable COVID-19 virus can remain airborne for minutes.29
Our study found similar patterns of MVPA before and during the pandemic as well as an absolute decline in the amount of time spent in PA.Most MVPA was work-related,whereas the least PA was related to traveling from place to place.Reductions in cumulative minutes of work-related,transportation,and recreational MVPA imply that the COVID-19 pandemic has disrupted the pattern of PA of Thai adults in most aspects of their daily lives.As more Thais attempt to work from home,the opportunity for MVPA is limited if they are confined to their domiciles or immediate neighborhoods.Also,working from home often means sitting for prolonged periods in a stationary position in front of a computer screen or other electronic device.In the pre-COVID-19 situation,it was assumed that people moved around more when working at the office,including commuting to and from the workplace.The partial lockdown policy also inhibited travel outside the home for dining,shopping,or leisure PA,all of which accumulate as more sedentary time passes.
In both the pre-pandemic and the pandemic periods,Thai males were more physically active than females.Both in terms of cumulative minutes and the proportion achieving sufficient MVPA,Thai males exceeded their female counterparts.Other things being equal,men are evolutionarily wired for more vigorous PA,given their historical role as the“hunter”,and they have a predilection for competitive physical challenges.30The male body is also physiologically constructed for a larger skeletal frame and muscle mass,which can influence duration of exertion in performing PA.31Additionally,the cultural belief in the importance of fair skin for Thai females may have played a significant barrier to outdoor PA.32During the pandemic,although the restrictive measures applied to all Thais,males were still able to accumulate more minutes of MVPA than females.Furthermore,other studies have found that females are more likely to practice social distancing,27,33-35whereas males are reported to be less compliant with self-isolation guidance.33Female psychological distress36and greater compliance with COVID-19 restrictive measures may have led many women to be more housebound and,thus,they may have had fewer opportunities for PA.
Middle-aged adults(40-64 years)were more active than their younger counterparts,both before and during the pandemic.Middle-aged adults include those in the peak earning years,so most of their PA was work-related.Younger adults,on the other hand,are more likely to record more recreational PA because some of them are students.A previous study reported that older adults participated in less PA during the pandemic due to their inability to find substitutes for their outdoor PA,22but the reasons the middle-aged Thai population in our study was more physically active than their younger counterparts in both pre-pandemic and pandemic periods was unclear.
During the pandemic,urban residents were less likely to have sufficient MVPA compared to their rural counterparts.Urban dwellers also recorded fewer cumulative minutes of MVPA than the rural sample in all PA domains.This may be because during the pandemic many urban dwellers were occupied with screen-related activities and had fewer opportunities for PA due to working-from-home policies,whereas rural residents were still able to work in the fields.The containment policy was also more strict for urban residents because an urban setting is a better environment for the spread of aerosolized virus because there is more crowding among strangers.Indeed,at the beginning of Thailand’s COVID-19 epidemic,most of the positive cases were found in cities with high population densities.The nightclub party and boxing stadium clusters related to COVID-19 transmission serve as examples of how the urban lifestyle poses a greater risk of infection.
The central and provincial government restrictions on population movement and the closing of facilities and outlets have almost certainly contributed to the absolute decline in MVPA detected in our study.However,Thai adults who received FFH messages were more likely to have sufficient MVPA during the pandemic.This finding suggests that national health-promotion interventions reached their target audience with information about exercising indoors and contributing to the containment of the epidemic.That said,as the Thai society and economy emerge from self-imposed isolation,many Thais have shifted their outdoor movement into home-based PA and may be gradually resuming their regular PA routines.
The limitations of our study should be acknowledged.The differing methods of data collection(face-to-face interviewsvs.online self-reporting)could have affected our overall results,particularly because online surveys tend to overestimate certain data.PA levels among children and the elderly also could not be documented and compared to the previous surveys due to the limitations of these 2 populations in accessing the Internet.
5.Conclusion
The pandemic measures imposed by the government reduced the cumulative minutes of work-related,transportation,and recreational PA and slowed Thailand’s progress toward its PA goals.Although the FFH campaign probably contributed to a slight increase in MVPA,it will take some time for Thais to return to pre-COVID-19 levels of PA.Health promotion messages need to be continuously delivered as a health-promoting intervention in order to reduce irrational fear of infection and boost the PA level of the Thai population.
It is important to note,however,that the COVID-19 pandemic is one of many public health threats,and it takes an unpredictable path.Although in Thailand the current trend is toward a continuous decline in new cases,there is always the possibility of subsequent waves of transmission,especially as the country enters the annual flu season in October.The pandemic has also placed the population at a double risk because physical inactivity and sedentary lifestyles may worsen the impact of future epidemics or exacerbate noncommunicable disease threats(e.g.,obesity,hypertension,and diabetes),which are also risk factors for complications of COVID-19 infection.Thus,the decreasing prevalence of sufficient MVPA among Thai adults should be a matter of concern for the government and policy makers as they consider strategies for protecting the health of the population in the months and years ahead.
Acknowledgment
The authors gratefully acknowledge funding support from the Thai Health Promotion Foundation with grant#63-0030.
Authors’contributions
PK conceived the study,performed the data compilation and formal data analysis,interpreted the findings,and wrote the manuscript;DAW conceptualized,drafted and wrote the manuscript,and interpreted the findings;NW conceived the study;NH performed the data analysis;PS conceptualized the manuscript.All authors reviewed and contributed to the final manuscript.All authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
Supplementary materials
Supplementary material associated with this article can be found in the online version at doi:10.1016/j.jshs.2020.10.001.
 Journal of Sport and Health Science2021年3期
Journal of Sport and Health Science2021年3期
- Journal of Sport and Health Science的其它文章
- A critical review of national physical activity policies relating to children and young people in England
- The evidence for the impact of policy on physical activity outcomes within the school setting:A systematic review
- State laws governing school physical education in relation to attendance and physical activity among students in the USA:A systematic review and meta-analysis
- Handgrip strength and health outcomes:Umbrella review of systematic reviews with meta-analyses of observational studies
- Is device-measured vigorous physical activity associated with health-related outcomes in children and adolescents? A systematic review and meta-analysis
- Conceptual physical education:A course for the future Charles B.Corbin