Is the EGFR pathway relevant for the pathogenesis but not for treatment of acute myeloid leukemia?
2021-05-12 02:05LucianaYamamotodeAlmeidaEduardoMagalhesRego
Luciana Yamamoto de Almeida, Eduardo Magalhães Rego,2
1Center for Cell-based Therapy, University of Sao Paulo, Ribeirao Preto, Sao Paulo CEP 14051-140, Brazil.
2Hematology Division, LIM31, Faculdade de Medicina, University of Sao Paulo, Sao Paulo CEP 05403-000, Brazil.
Abstract Despite intense research and the development of several new chemotherapeutics, the prognosis for specific subsets of acute myeloid leukemia (AML) has not improved significantly. Thus, the investigation of signaling pathways associated with the pathogenesis and progression of AML has become a source for the discovery of more effective treatments. The epidermal growth factor receptor (EGFR) belongs to the HER family of tyrosine kinase (TK) receptors and is involved in the progression of a variety of solid tumors. Although the expression of members of the HER family appears to be limited to epithelial tissues and derived neoplasms, there is evidence demonstrating their role in hematopoiesis and hematological neoplasms. In AML, preclinical studies and two anecdotal cases of response to EGFR TK inhibitors (TKI) supported the EGFR signaling pathway as a potential therapeutic target. Indeed, the presence of EGFR ligands in the bone marrow microenvironment has been shown to play pathological and regenerative/protective roles in AML. However, data reporting the expression of EGFR in AML remain controversial and the EGFR pathway inhibition in AML patients has demonstrated limited clinical significance. Further studies are required to determine the relevance of the EGFR pathway in AML biology and which patients may benefit from using EGFR TKI or other drugs that target TK receptors.
Keywords: Acute myeloid leukemia, epidermal growth factor receptor, EGFR ligands, EGFR tyrosine kinase inhibitors, gefitinib, erlotinib
INTRODUCTION
Epidermal growth factor receptor (EGFR) is a type of tyrosine kinase (TK) receptor recognized as an important player in the tumor biology of many solid neoplasms, making it a key target for therapeutic strategies, especially in non-small cell lung cancer (NSCLC). EGFR TK inhibitors (TKI) have demonstrable efficacy in the treatment of patients with EGFR-mutated NSCLC with a favorable impact on progressionfree survival, but not in the subgroup of EGFR wild-type tumors[1,2]. In contrast, EGFR mutations are rarely found in AML[3,4], while their expression has been reported to be associated with poor prognostic outcomes[5]. Accordingly,in vitro,ex vivo, andin vivoresults demonstrate that EGFR TKI induces terminal differentiation and cell death of AML cells[2,6-8]. Moreover, in the bone marrow microenvironment,interactions between leukemia stem/progenitor cells (LSPCs) and immune cells promoted the expansion of leukemia cell subsets, which was associated with the upregulation of interleukin (IL)-3gene expression in LSPCs [Figure 1][9,10]. Of note, Radpouret al.[11]showed that, in favorable-risk AML,IL-3gene expression in CD34+LSPCs was positively correlated withEGF/EGFRgene expression in CD8+T cells. Furthermore, this finding was functionally validated in a co-culture system with CD8+T cells and CD34+LSPC. Accordingly,CD8+T cells promoted the expansion of LSPC by increasingIL-3mRNA and protein. On the other hand,IL-3gene expression and cell proliferation were reduced in LSPC in the presence of the neutralizing antibody to EGFR[11]. Together, these data support the idea that EGFR TKI could be a promising alternative therapy to treat AML. However, EGFR expression is low or absent in most AML samples and cell lines[2,5,12],indicating that the anti-proliferative and pro-apoptotic effects of EGFR TKI may occur by EGFRindependent mechanisms, through interaction with other TK receptors[2,6,7,13,14]. Among them, preclinical data identify SYK (Spleen tyrosine kinase)[15], Lyn[16], other TK of the Src family kinases (SFKs)[17], signal transducer and activator of transcription 5, and Janus kinase 2[2]as off-targets of the EGFR TKI erlotinib and gefitinib in AML cells. However, it needs to be pointed out that no difference in survival or objective response was observed in clinical trials of patients with AML in which EGFR TKI was administered[18-20].
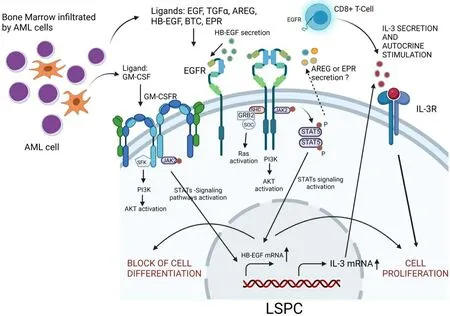
Figure 1. Schematic representation of the EGFR signaling axis and its most important downstream targets in the AML microenvironment.EGFR ligands in the bone marrow microenvironment phosphorylate EGFR receptors on the surface of LSPC or CD8+ T cells, leading to the production and release of IL-3. In turn, IL-3 induces proliferation signals in LSPCs, promoting the expansion of AML cells. Direct arrows represent direct interactions, and the dotted arrow represents indirect effects. AML: Acute myeloid leukemia; LSPCs: leukemia stem/progenitor cells; IL-3: interleukin-3; EGFR: epidermal growth factor receptor; EGF: epidermal growth factor; TGF-α: transforming growth factor-alpha; AREG: amphiregulin; HB-EGF: EGF-like heparin-binding factor; BTC: betacellulin; EPR: epiregulin; SFK: src family kinases; PI3K: phosphatidylinositol 3-kinase; AKT: protein kinase B; JAK2: Janus-activated kinase 2; JAK: Janus-activated kinase; STAT5:signal transducer and activator of transcription 5. Image created using BioRender.com.
Therapeutic strategies that target the EGFR pathway have received considerable attention in other oncologic settings, but it is still unclear which patients with AML may benefit from EGFR TKI therapy. In this review,we summarize the knowledge regarding the role of the EGFR signaling pathway in AML and provide an overview of experimental and clinical studies using EGFR TKI to suppress leukemia progression.
EGFR
EGFR (also described as HER1 and ERBB1) is a transmembrane glycoprotein (170 kDa) that belongs to the HER family of TK receptors, which comprises four members (HER1 or EGFR, HER2, HER3, and HER4)and plays an important role in regulating cell proliferation, survival, differentiation, angiogenesis, and metastatic spread[21-23]. The extracellular domain of this receptor can bind to seven official different types of ligands: EGF, transforming growth factor-alpha, amphiregulin (AREG), EGF-like heparin-binding factor(HB-EGF), betacellulin, epiregulin (EPR), and epigen[24,25]. Moreover, the connective tissue growth factor(CTGF/CCN2) has been identified as a new EGFR ligand[26]. Interestingly, the affinity of EGFR can be varied, depending on the specific ligand, tissue, and physiological and pathological conditions, which cause different cellular responses[27-29]. The interactions of EGFR with its ligands induce the homodimerization or heterodimerization of the receptor with another member of the HER family. Dimerization leads to EGFR autophosphorylation at specific tyrosine residues in the intracellular domain, triggering the activation of downstream signaling pathways, such as mitogen-activated protein kinases (MAPK), phosphatidylinositol 3-kinase/protein kinase B (PI3K/AKT), and Janus-activated kinase/signal transducer and activator of transcription (JAK-STAT)[24,25].
The aberrant expression and/or mutation ofEGFR, as well as the continuous stimulation of this receptor due to the greater presence of its ligands in the tumor microenvironment, have a direct implication in the pathogenesis and progression of cancer since they are associated with increased tumor growth, invasion,and metastasis[30]. For this reason, EGFR has been described as an important therapeutic target in several malignant neoplasms, such as pancreas, colorectal, lung, breast, and head and neck carcinomas[31]. However,in hematological malignancies,EGFRmutations are very rare[3,4,32], and its expression and clinical response to EGFR TKI in AML is still controversial.
EGFR EXPRESSION IN AML
Aberrant expression of EGFR has been associated with aggressive behavior in a wide range of solid tumors[31], but the role and pattern of EGFR expression in hematological malignancies are still not well understood. Specifically, in AML,EGFRmRNA was detectable in approximately 35% of patients and correlated with decreased overall (OS) or event-free survival[5,33]. Notably, although acute promyelocytic leukemia (APL) is the most curable form of AML in adults, theEGFRgene expression in 5/29 (17.5%) of the patients was also associated with an adverse clinical outcome[34]. At the protein level, some studies pointed out the absence of EGFR expression in some AML cell lineages and primary cells[2,6,8,35]. However,Mahmudet al.[12]demonstrated that 11% (57/511) and 18% (93/511) of AML patients express high levels of total and phosphorylated EGFR, respectively, when compared to CD34+healthy bone marrow samples,suggesting that this subset could benefit from EGFR TKI therapy. Accordingly, only leukemic cell lines positive for EGFR were responsive to cetuximab-induced cell death[5]. Specifically, in APL samples, our group detected total and phosphorylated EGFR protein in 6/21 (28.5%) and 4/21 (19%) of APL patients,respectively, but not in CD34+healthy bone marrow samples. In addition, we demonstrated that gefitinib enhanced theall-trans retinoic acid (ATRA)-induced differentiation in EGFR-negative APL cells lines NB4 and NB4-R2 (de Almeida LY and Rego EM, own unpublished observation, 15 June 2021).
The reasonEGFRexpression affects the prognosis of patients with AML has not been addressed so far.Interestingly, increased HSC mobilization induced by granulocyte colony-stimulating factor (G-CSF) was achieved in healthy donors after the pharmacological inhibition of EGFR activity through activation of GTPase Cdc42 (cell division control protein-42)[36]. In addition, in a chemotherapy-induced myelosuppression model, the combination of G-CSF and EGF was synergistic for regeneration of the bone marrow compared to either G-CSF or EGF alone, and EGF increased G-CSF receptor expression following exposure to 5-fluorouracil. Conversely, G-CSF treatment increased both EGFR and phosphorylation of EGFR in hematopoietic stem/progenitor cells. Considering that in AML sensitization of leukemic cells with hematopoietic growth factors may enhance the cytotoxicity of chemotherapy, the association of G-CSF and EGFR TKI may be beneficial[37]. Accordingly, a Japanese nationwide retrospective analysis of the outcome of cord blood transplantation for AML showed that the addition of G-CSF-combined cytarabine to a total body irradiation plus cyclophosphamide conditioning regimen resulted in a significantly better disease-free survival and OS and a reduced relapse rate[38]. It is conceivable that the association of EGFR TKI to G-CSF could increase the sensitization of leukemic cells to cytotoxic therapy and further improve the outcome of HCT in AML.
EGFR LIGANDS EXPRESSION IN AML
The mRNA expression ofAREG[39],HB-EGF[40], andEREG[41]genes, whose translational products are EGFR ligands, were previously detected in AML samples, but their prognostic relevance has not been defined. TheAREGexpression pattern has been recognized to be useful to distinguish AML from B-cell lymphoblastic leukemia[39]. Similarly,HB-EGFis expressed in human myeloid and T, but not B, lymphoid cell lines[40].Moreover, the main differentially expressed gene between arginase-resistant and -sensitive AML isEREG,which encodes the protein EPR[41]. Indeed,EREGoverexpression in solid tumors was associated with cancer cell proliferation via EGFR/MAPK/PI3K/AKT signaling[42]. However, more investigation is necessary to understand the biological implications ofEREGsignaling in AML.
Wuet al.[43]evaluated the urine of 18 patients with APL and found that they had significantly elevated levels of EGF when compared to healthy patients. Besides, lower and higher levels of EGF excretion were associated with complete remission and clinical recurrence, respectively, in patients with APL. Thus, these authors suggested that quantifying EGF levels may serve as a means of monitoring this disease. However,the significant correlation between EGF and creatinine detected in the urine did not have a direct relationship with EGF levels in blood serum or plasma[44]. It suggests that EGF is mainly derived from kidney biosynthesis secretion and that the levels of EGF in the urine are probably a reflection of treatment with ATRA rather than that released by the APL cells themselves. In the bone marrow microenvironment,CD8+T cells promoted LSPCs expansion via upregulation of IL-3 through EGF/EGFR signaling in favorable-risk, but not intermediate- or adverse-risk, AML[11].In vitro, the pro-proliferative effect of CD8+T cells on LSPCs was abrogated in the presence of anti-EGFR antibodies[11]. The differential response of LSPC cells to the CD8+T stimuli suggests that LSPCs in favorable-risk AML cases display a higher dependence on the microenvironment to expand [Figure 1]. We found that EGF bone marrow plasma levels were lower in APL patients when compared to healthy control subjects. In addition, AREG was detected in 5/17 APL bone marrow plasma samples and absent in 20 control samples. However, the significance of these ligands in APL development remains to be determined once ourin vivodata show that gefitinib treatment did not provide additional survival benefit in a transgenic mouse model of APL. (de Almeida LY and Rego EM, own unpublished observation, 15 June 2021).
EGFR ligands exert distinct functions depending on the biological context and on what type of cell they originate. Ramadanet al.[45]experimentally demonstrated that a specific T cell subtype [T9IL-33(interleukin-9-producing T cells activated via the ST2-IL-33 pathway)], responsible for graft-vs.-leukemia reactivity,express high levels ofAREG, and the AREG blockade on T cells increased graft-vs.-host disease severityin vivo, but it did not affect their ability to kill myeloid leukemia cellsin vitro. In chronic myeloid leukemia(CML), CML cell-derived exosomes carrying AREG activated the EGFR signaling in stromal cells, which in turn secreted IL-8, stimulating the proliferation of leukemic cells[46]. Furthermore, in the context of myelosuppression, EGF promoted survival and regeneration of hematopoietic stem cells following irradiation[47], thereby providing a beneficial improvement for myeloid reconstitution. Together, these findings suggest that EGFR ligands have important pathological and protective functions in myeloid leukemogenesis.
THE ROLE OF EGFR TKI IN THE TREATMENT OF AML
Since EGFR activation is involved in cancer progression, a variety of drugs targeting this signaling pathway have been developed and proven to be effective in the treatment of solid tumors and, particularly, in NSCLC[48]. The main classes of FDA-approved drugs that act on the EGFR pathway are monoclonal antibodies (e.g., cetuximab and panitumumab), which bind to the EGFR extracellular domain competing with endogenous ligands, and the TKI (e.g., gefitinib, erlotinib, and afatinib), which block the intracellular domain of this receptor, impairing the activation of cell signaling cascades that promote the proliferation of malignant cells[49-51]. EGFR-based therapies were also tested in leukemic settings, demonstrating to induce apoptosis and differentiation of AML cell lines and primary blasts at low micromolar concentrations that are achievable in clinical practice, as summarized in Table 1. Noteworthy, unlike healthy CD34+cells,erlotinib particularly induced AML-derived CD34+cells apoptosis in a time- and dose-dependent manner[2]. In addition, a complete remission of AML in two adult patients with concurrent NSCLC was obtained after treatment with erlotinib[35,52]. AlthoughEGFRgene expression may be clinically useful for predicting AML outcomes[5,33,34], the receptor was not detected in the blasts of these patients, suggesting that erlotinib probably acted via EGFR-independent mechanisms. Thus, based on the controversial data regarding EGFR expression in AML samples, further studies analyzed the cross-pharmacological interactions of EGFR TKI to predict potential off-targets. In this regard, preclinical data demonstrate that erlotinib induces apoptosis in AML cells by inhibiting JAK-2 and STAT-5[2]and reduced the activation of SFK and mTOR signaling pathways[17], which are constitutively activated in AML blasts. In addition,proteomic and genetic approaches identified SYK as a gefitinib target for AML differentiationin vitro[15]. It is particularly noteworthy that increased expression of phosphorylated SYK in AML samples, especially in those harboring internal tandem duplication mutations in theFLT3gene (FLT3-ITD), was related to unfavorable clinical outcomes[53,54]. Recently, Caoet al.[16]demonstrated that erlotinib plays a dual role targeting FLT3 in FLT3-ITD mutant AML cells and SYK and Lyn, another TK associated with leukemia proliferation, in FLT3-ITD negative AML cells, thereby showing a potential advantage of erlotinib use to overcome the cellular heterogeneity that exists in AML.
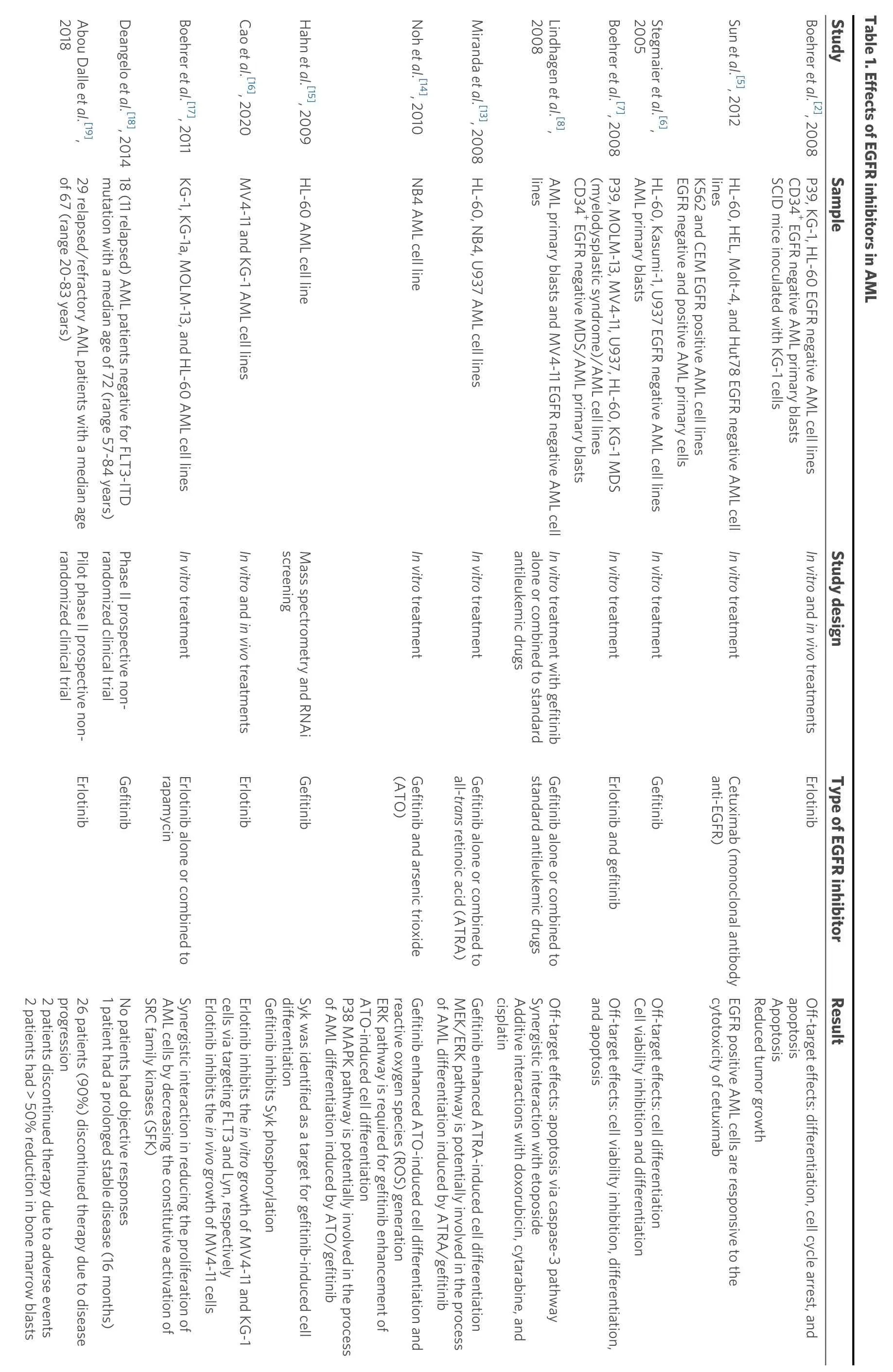
2018 Abou Dalle et al.[19],2008 Lindhagen et al.[8],2005 Stegmaier et al.[6],of 67 (range 20-83 years)29 relapsed/refractory AML patients with a median age mutation with a median age of 72 (range 57-84 years)Deangelo et al.[18], 2014 18 (11 relapsed) AML patients negative for FLT3-ITD Miranda et al.[13], 2008 HL-60, NB4, U937 AML cell lines lines AML primary blasts and MV4-11 EGFR negative AML cell CD34+ EGFR negative MDS/AML primary blasts(myelodysplastic syndrome)/AML cell lines AML primary blasts HL-60, Kasumi-1, U937 EGFR negative AML cell lines EGFR negative and positive AML primary cells K562 and CEM EGFR positive AML cell lines lines SCID mice inoculated with KG-1 cells CD34+ EGFR negative AML primary blasts Study Sample Table 1. Effects of EGFR inhibitors in AML randomized clinical trial Pilot phase II prospective nonrandomized clinical trial Phase II prospective nonscreening Mass spectrometry and RNAi antileukemic drugs alone or combined to standard In vitro treatment with gefitinib In vitro treatment In vitro treatment Erlotinib Gefitinib rapamycin In vitro and in vivo treatments Erlotinib Gefitinib(ATO)In vitro treatment Gefitinib and arsenic trioxide all-trans retinoic acid (ATRA)In vitro treatment Gefitinib alone or combined to standard antileukemic drugs Gefitinib alone or combined to In vitro treatment Gefitinib anti-EGFR)Cetuximab (monoclonal antibody In vitro and in vivo treatments Erlotinib 2 patients had > 50% reduction in bone marrow blasts 2 patients discontinued therapy due to adverse events progression 26 patients (90%) discontinued therapy due to disease 1 patient had a prolonged stable disease (16 months)No patients had objective responses SRC family kinases (SFK)AML cells by decreasing the constitutive activation of Erlotinib inhibits the in vivo growth of MV4-11 cells Boehrer et al.[17], 2011 KG-1, KG-1a, MOLM-13, and HL-60 AML cell lines In vitro treatment Erlotinib alone or combined to Synergistic interaction in reducing the proliferation of cells via targeting FLT3 and Lyn, respectively Gefitinib inhibits Syk phosphorylation Cao et al.[16], 2020 MV4-11 and KG-1 AML cell lines Erlotinib inhibits the in vitro growth of MV4-11 and KG-1 differentiation of AML differentiation induced by ATO/gefitinib Hahn et al.[15], 2009 HL-60 AML cell line Syk was identified as a target for gefitinib-induced cell P38 MAPK pathway is potentially involved in the process ATO-induced cell differentiation ERK pathway is required for gefitinib enhancement of reactive oxygen species (ROS) generation of AML differentiation induced by ATRA/gefitinib Noh et al.[14], 2010 NB4 AML cell line Gefitinib enhanced ATO-induced cell differentiation and MEK/ERK pathway is potentially involved in the process Gefitinib enhanced ATRA-induced cell differentiation cisplatin Additive interactions with doxorubicin, cytarabine, and Synergistic interaction with etoposide Off-target effects: apoptosis via caspase-3 pathway and apoptosis Cell viability inhibition and differentiation Boehrer et al.[7], 2008 P39, MOLM-13, MV4-11, U937, HL-60, KG-1 MDS Erlotinib and gefitinib Off-target effects: cell viability inhibition, differentiation,Off-target effects: cell differentiation cytotoxicity of cetuximab Reduced tumor growth Sun et al.[5], 2012 HL-60, HEL, Molt-4, and Hut78 EGFR negative AML cell EGFR positive AML cells are responsive to the Apoptosis apoptosis Study design Type of EGFR inhibitor Result Boehrer et al.[2], 2008 P39, KG-1, HL-60 EGFR negative AML cell lines Off-target effects: differentiation, cell cycle arrest, and
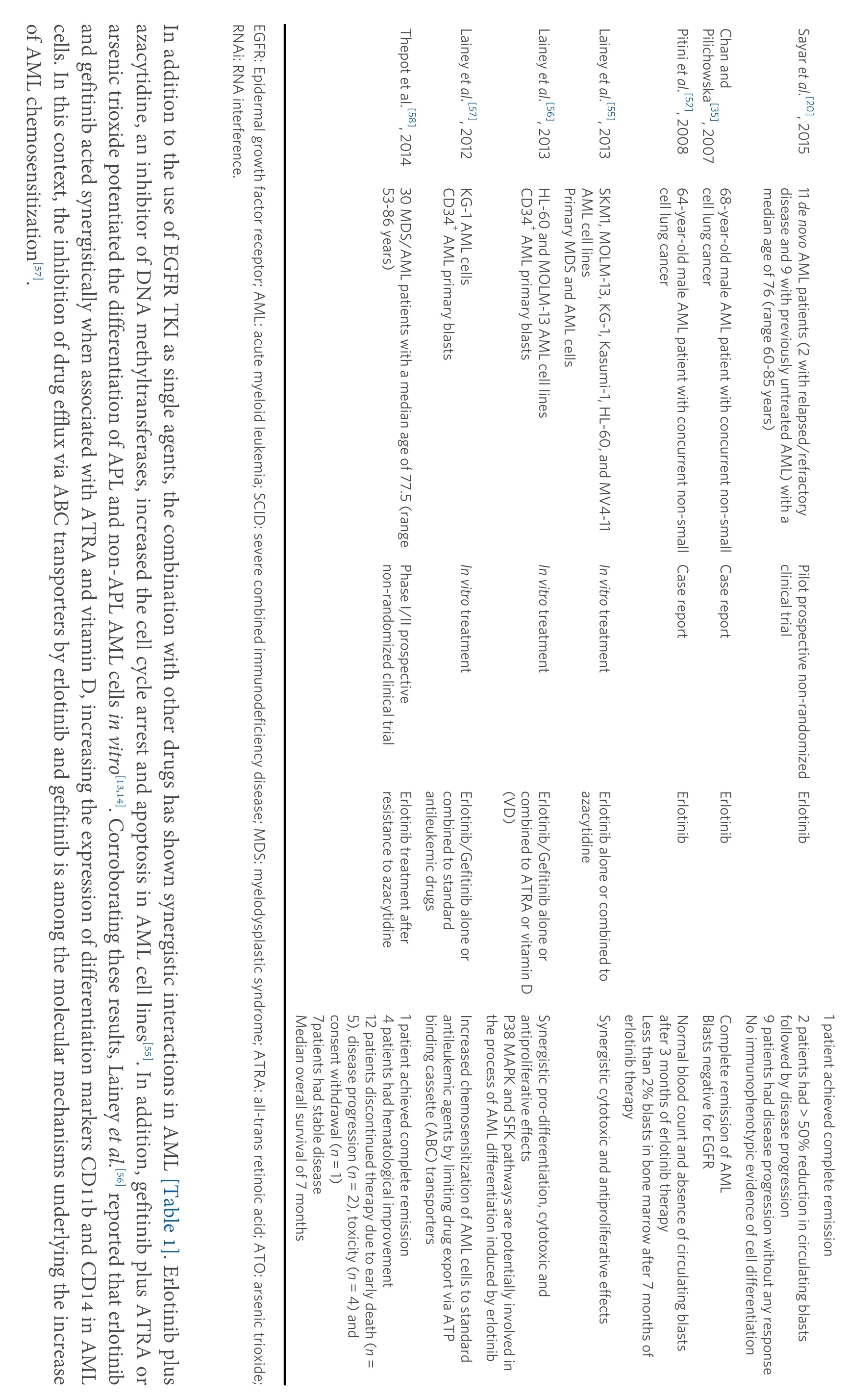
of AML chemosensitization[57].cells. In this context, the inhibition of drug efflux via ABC transporters by erlotinib and gefitinib is among the molecular mechanisms underlying the increase and gefitinib acted synergistically when associated with ATRA and vitamin D, increasing the expression of differentiation markers CD11b and CD14 in AML arsenic trioxide potentiated the differentiation of APL and non-APL AML cells in vitro[13,14]. Corroborating these results, Lainey et al.[56] reported that erlotinib azacytidine, an inhibitor of DNA methyltransferases, increased the cell cycle arrest and apoptosis in AML cell lines[55]. In addition, gefitinib plus ATRA or In addition to the use of EGFR TKI as single agents, the combination with other drugs has shown synergistic interactions in AML [Table 1]. Erlotinib plus RNAi: RNA interference.EGFR: Epidermal growth factor receptor; AML: acute myeloid leukemia; SCID: severe combined immunodeficiency disease; MDS: myelodysplastic syndrome; ATRA: all-trans retinoic acid; ATO: arsenic trioxide;Pilichowska[35], 2007 Chan and 53-86 years)CD34+ AML primary blasts CD34+ AML primary blasts Lainey et al.[56], 2013 HL-60 and MOLM-13 AML cell lines Primary MDS and AML cells AML cell lines cell lung cancer cell lung cancer median age of 76 (range 60-85 years)disease and 9 with previously untreated AML) with a non-randomized clinical trial Phase I/II prospective Case report 68-year-old male AML patient with concurrent non-small Case report clinical trial Pilot prospective non-randomized resistance to azacytidine Erlotinib treatment after antileukemic drugs combined to standard In vitro treatment Erlotinib/Gefitinib alone or(VD)combined to ATRA or vitamin D In vitro treatment Erlotinib/Gefitinib alone or azacytidine In vitro treatment Erlotinib alone or combined to Erlotinib Erlotinib Erlotinib Median overall survival of 7 months 7patients had stable disease consent withdrawal (n = 1)5), disease progression (n = 2), toxicity (n = 4) and 12 patients discontinued therapy due to early death (n =4 patients had hematological improvement binding cassette (ABC) transporters Thepot et al.[58], 2014 30 MDS/AML patients with a median age of 77.5 (range 1 patient achieved complete remission antileukemic agents by limiting drug export via ATP the process of AML differentiation induced by erlotinib Lainey et al.[57], 2012 KG-1 AML cells Increased chemosensitization of AML cells to standard P38 MAPK and SFK pathways are potentially involved in antiproliferative effects Synergistic pro-differentiation, cytotoxic and erlotinib therapy Lainey et al.[55], 2013 SKM1, MOLM-13, KG-1, Kasumi-1, HL-60, and MV4-11 Synergistic cytotoxic and antiproliferative effects Less than 2% blasts in bone marrow after 7 months of after 3 months of erlotinib therapy Blasts negative for EGFR Pitini et al.[52], 2008 64-year-old male AML patient with concurrent non-small Normal blood count and absence of circulating blasts Complete remission of AML No immunophenotypic evidence of cell differentiation 9 patients had disease progression without any response followed by disease progression 1 patient achieved complete remission Sayar et al.[20], 2015 11 de novo AML patients (2 with relapsed/refractory 2 patients had > 50% reduction in circulating blasts
Despite the strong experimental evidence that EGFR inhibitors have an anti-leukemic activity in AML,erlotinib and gefitinib have shown limited clinical efficacy. Erlotinib monotherapy failed to induce differentiation[20]and avoid disease progression in 26/29 (90%) patients with refractory or relapsed AML[19],while a response rate of 20% was achieved in azacytidine-resistant patients with AML/MDS(myelodysplastic syndromes)[58]. Moreover, the use of gefitinib as a single agent in a phase II trial conducted in 18 patients with advanced AML did not promote an objective response, except for one patient who had stable disease for 16 months[18]. Similarly,in vitrotreatment with gefitinib showed no difference in terms of cytotoxic activity in leukemic blasts from patients with newly diagnosed or relapsed AML[8]. Nevertheless,these studies have potential limitations. Some hypotheses that could explain the failure of EGFR TKI treatment in AML are the small number of patients, the lack of criteria for selection of patients expressing EGFR or other biomarkers suitable for EGFR TKI therapy, an inadequate dose, and drug administration only as monotherapy. Overall, the administration of gefitinib and erlotinib as single agents appears to be well-tolerated, without significant organ/systemic toxicity[18-20,51,58], encouraging further exploration of EGFR TKI in combination with other drugs already used to treat AML in larger clinical trials.
CONCLUSION
EGFR signaling appears to support leukemogenesis or hematopoietic regeneration, depending on the cell type and biological context in which the pathway is activated, but the complete characterization regarding the expression and function of EGFR and other EGFR TKI responsive targets in the different compartments of the leukemia microenvironment remains largely unknown. Therefore, the determination of predictive biomarkers in the AML setting is necessary to guide which patients could benefit from selective targeted TKI.
DECLARATIONS
Authors’ contributions
Made substantial contributions to conception and design of the study and performed bibliography review and writing of the manuscript: de Almeida LY, Rego EM
The Prince and his bride set free all the Christian folk who were imprisoned27 there, and took away with them all the gold and silver that they could carry, and moved far away from the castle which lay east of the sun and west of the moon
Availability of data and materials
Not applicable.
Financial support and sponsorship
This work was supported by FAPESP grant# 2013/08135-2 and FAPESP fellowship for de Almeida LY(grant No. 2016/02713-2).
Conflicts of interest
Both authors declared that there are no conflicts of interest.
Not applicable.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2021.