
Chinese Association for the Study of Pain: Experts consensus on ultrasound-guided injections for the treatment of spinal pain in China(2020 edition)
2021-04-08 08:49YunWangAiZhongWangBaiShanWuYongJunZhengDaQiangZhaoHuiLiuHuaXuHongWeiFangJinYuanZhangZhiXiangChengXiangRuiWang
World Journal of Clinical Cases 2021年9期
Yun Wang, Ai-Zhong Wang, Bai-Shan Wu, Yong-Jun Zheng, Da-Qiang Zhao, Hui Liu, Hua Xu, Hong-Wei Fang, Jin-Yuan Zhang, Zhi-Xiang Cheng, Xiang-Rui Wang
Yun Wang, Department of Anesthesiology, Beijing Chaoyang Hospital, Capital Medical University, Beijing 100020, China
Ai-Zhong Wang, Department of Anesthesiology, The Sixth Affiliated People's Hospital,Shanghai Jiao Tong University, Shanghai 200233, China
Bai-Shan Wu, Department of Algology, Xuanwu Hospital, Capital Medical University, Beijing 100053, China
Yong-Jun Zheng, Department of Algology, Huadong Hospital Affiliated to Fudan University,Shanghai 200040, China
Da-Qiang Zhao, Department of Anesthesiology, Jiahui International Hospital, Shanghai 200233,China
Hui Liu, Department of Algology, West China Hospital, Sichuan University, Chengdu 610041,Sichuan Province, China
Hua Xu, Department of Anesthesiology, Yueyang Hospital of Integrated Traditional Chinese and Western Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai 200437, China
Hong-Wei Fang, Jin-Yuan Zhang, Xiang-Rui Wang, Department of Algology, East Hospital,Tongji University, Shanghai 200120, China
Zhi-Xiang Cheng, Department of Algology, The Second Affiliated Hospital, Nanjing Medical University, Nanjing 210011, Jiangsu Province, China
Abstract Spinal pain (SP) is a common condition that has a major negative impact on a patient’s quality of life. Recent developments in ultrasound-guided injections for the treatment of SP are increasingly being used in clinical practice. This clinical expert consensus describes the purpose, significance, implementation methods,indications, contraindications, and techniques of ultrasound-guided injections.This consensus offers a practical reference point for physicians to implement successfully ultrasound-guided injections in the treatment of chronic SP.
Key Words: Spinal pain; Ultrasound-guided injections; Facet joints; Spinal nerve roots;Posterior spinal nerve; Experts consensus
INTRODUCTION
Spinal pain (SP) is a common condition that has a major negative impact on patient’s quality of life[1]. Targeted injections in the spine guided by imaging devices are advantageous over conventional injection techniques as they can be delivered with improved accuracy and reduce the risk of complications[2,3]. The recent development of portable ultrasound systems has led to the increased clinical implementation of ultrasound-guided spine injections[4]. These techniques can significantly reduce the requirements for radiation-guided treatments and avoid unnecessary radiation exposure[5]. However, the standard clinical practice of ultrasound-guided injections in the spine has yet to be clearly defined in terms of the application process, indications,and technical operations[6]. To establish clinical standards for ultrasound-guided SP injections, this expert consensus was proposed by domestic experts working on ultrasound-guided pain treatments to guide clinicians and medical experts on the correct use of ultrasound-guided injections for SP.
PURPOSE AND SIGNIFICANCE OF ULTRASOUND-GUIDED SP INJECTIONS
SP is a frequently occurring condition that manifests clinically with pain in the head and neck, the extremities, the chest wall, and the back, requiring pain management[7,8].The curative treatment of SP remains challenging, often resulting in patients experiencing chronic pain with severe impact on their quality of life. Ultrasound can be used to provide real-time information during SP targeted injections. Ultrasoundguided SP injections can be used to eliminate inflammation and to treat pain through direct injection of drugs into areas of pain origin, such as the facet joints, spinal nerve roots, or the medial branch of the posterior spinal nerve[2].
BASIC REQUIREMENTS OF MEDICAL INSTITUTIONS
Medical institutions delivering SP injection techniques should be matched with their respective functions and clinical expertise.
Secondary and tertiary hospitals should have pain-relating services approved and registered by health administrative departments such as surgery, pain management,and anesthesiology departments. Also, hospitals should have all of the required devices and facilities necessary to deliver SP injections.
The basic requirements of facilities at medical institutions using SP injections are as follows: (1) Basic facilities for clinical SP injections including a preparation, operation,and postoperative observation rooms or wards; (2) Basic devices for SP injections including a nerve stimulator, ultrasound machine, and a C-arm X-ray machine (as some procedures may need to be performed using both ultrasound and the C-arm Xray machines). The operation room for SP injections should be equipped with the following devices: A tracheal intubation device, a multi-functional anesthesia machine,a monitor device, and a defibrillator; (3) Basic drugs for SP injections and emergency drugs that may be required during accidents or complications; and (4) Sterilization devices, adequate infection control, and management measures should exist within the hospital.
Doctors delivering ultrasound-guided SP injections should be specialist clinicians who work on pain management and have received ultrasound training.
IMPLEMENTATION CONDITIONS FOR ULTRASOUND-GUIDED SP INJECTIONS
Common parameter settings of the ultrasound device
The following common parameter settings should be applied during ultrasoundguided SP injections[9,10]: (1) Regulation of imaging depth: Proper depth refers to the target structure placed in the center of the ultrasound image or at 1 cm deeper than the target structure; (2) Gain regulation (gain of time/distance compensation): Ultrasound signals attenuate as they pass through tissues. Gain regulation and compensation for attenuation can allow structural echoes in different tissues to be distinguished; (3)Focus regulation: A suitable focus number should be chosen and depth adjusted to ensure the focus depth is in line with the depth of the target structure; and (4) Proper use of Doppler function: The Doppler effect should be utilized to identify vessels and the direction of drug diffusion.
Patient preparation
Patients undergoing SP injections are not required to fast, except when intravenous anesthesia is required[11]. In these circumstances, patients should fast for 8 h before treatment. Generally, an access to the peripheral venous is established before puncture and injection. The monitoring of basic vital signs (non-invasive blood pressure,electrocardiogram, and oxygen saturation) is required during operation. Before puncture, midazolam can be injected intravenously at a dosage of 0.02-0.06 mg/kg.For pediatric patients, ketamine can be delivered by intramuscular injection at a dose of 0.5-1 mg/kg[12]. For patients with breathing difficulties, a nasal catheter or oxygen mask should be used.
Rescue facilities
Ultrasound-guided SP injections should be performed in an operation or treatment room that has the necessary conditions for treatments. The onset time of injection is dependent on the target nerve, patient-specific characteristics, and the use of local anesthetics. Doctors performing the injections should have sufficient time and space to undertake the injection and also for post-operative follow-up. Rooms used for the injection procedure should be equipped with monitoring facilities, an oxygen supply,rescue drugs, and all other relevant materials.
Aseptic principles
Proper sterile practices and draping are recommended before puncture. The transducer and cable should be covered with a sterile plastic sleeve to ensure the injection is performed under sterile operating conditions to prevent infection in the puncture area and to avoid damage to the ultrasound probe by disinfectant.
Probe selection
The probe is a device that conveys and receives ultrasound waves. It is divided into linear (high frequency) and convex array (low frequency) probes. The linear array probe has high resolution but poor penetration ability, whilst the convex array probe has low resolution but good penetrating ability. If the target structure to be injected is located at the deeper area, the convex array probe should be selected, otherwise, the linear array probe should be used for ultrasound guidance[13].
Scanning techniques[14]
Probe pressurization:The distance between the target and probe should be minimized to improve imaging quality. Sliding the probe along the skin surface should be performed to track certain structures.
Probe rotation:The probe should be rotated to obtain an image of the target structure and switched between its cross-section and vertical sections.
Probe tilt:The incident angle between the probe and the skin should be adjusted to enable the ultrasound beam to be fully reflected by the target structure. This allows the probe to receive the clearest possible images.
Method of needle insertion
Needle insertion methods can be divided into in- and out-of-plane according to the position of the needle puncture within the scanning range of the ultrasound probe[15].The in-plane puncture method results in the needle tip and shaft being observed in the ultrasound images. The out-of-plane puncture method shows a high echo bright spot in the ultrasound image, however, this method cannot distinguish the needle tip and shaft. As a result, the in-plane puncture method should be preferentially used for injection into the spinal nerve root to avoid complications[16].
INDICATIONS AND CONTRAINDICATIONS FOR ULTRASOUND-GUIDED SP INJECTIONS
Indications
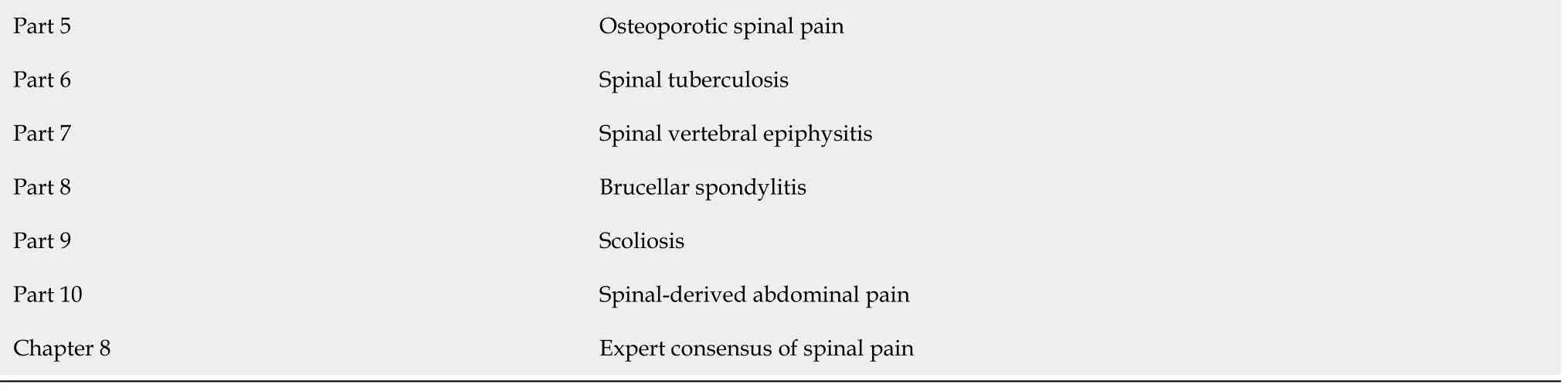
Ultrasound-guided SP injections can be used to treat tumors and multilevel intervertebral disc disorders in which surgical treatment is unsuitable[6]. These include lumbar disc herniation, cervicogenic headaches, occipital neuralgia, articular process disorders, medial branch pain of the posterior spinal nerve, herpes zoster and postherpetic neuralgia, reflective sympathetic dystrophy, thoracic outlet syndrome,intercostal neuralgia, post-operative recurrent radicular pain, and radicular pain.Other indications include scenarios requiring immediate alleviation of radicular pain and in patients with a positive neurological examination, but insignificant vital signs[17-21]. For more detailed indications for spine-related pain or diseases, please refer to Table 1.
Contraindications
Absolute contraindications for ultrasound-guided SP injections include uncooperative patients (including mental patients), patients with whole-body infection or infection in the puncture area, patients with bleeding tendencies, patients allergic to local anesthetics, patients with severe hypovolemia, patients with unclear diagnosis, and patients adversely affected by illness due to injections[22,23].
Relative contraindications include patients with severe heart disease, patients with severe systemic conditions, patients with other diseases that can be adversely affected due to injections, and patients with severe hypertension, diabetes, or active ulcers.
COMMON TECHNIQUES OF ULTRASOUND-GUIDED SP INJECTIONS
Cervical spine
The cervicogenic pain refers to pain caused by disorders of the cervical structures.Specifically, these include: The cervical sympathetic nerve, the cervical dorsal root ganglion, the cervical nerve root, the cervical dorsal rami nerve, the medial branch of the cervical dorsal rami nerve, the cervical zygapophyseal joints, the cervical atlantoaxial joints, and the cervical intervertebral disc. Ultrasound-guided injection techniques for cervical SP include stellate ganglion block, selective cervical nerve root block, medial branch block of the posterior cervical nerve, cervical zygapophyseal joint block, block of the atlantoaxial joint block, C2 dorsal root ganglion block, block of the nerve root and posterior nerve branch, the greater occipital nerve block, and the third occipital nerve block[24-27]. All of the techniques mentioned above can be performed under real-time ultrasound guidance.
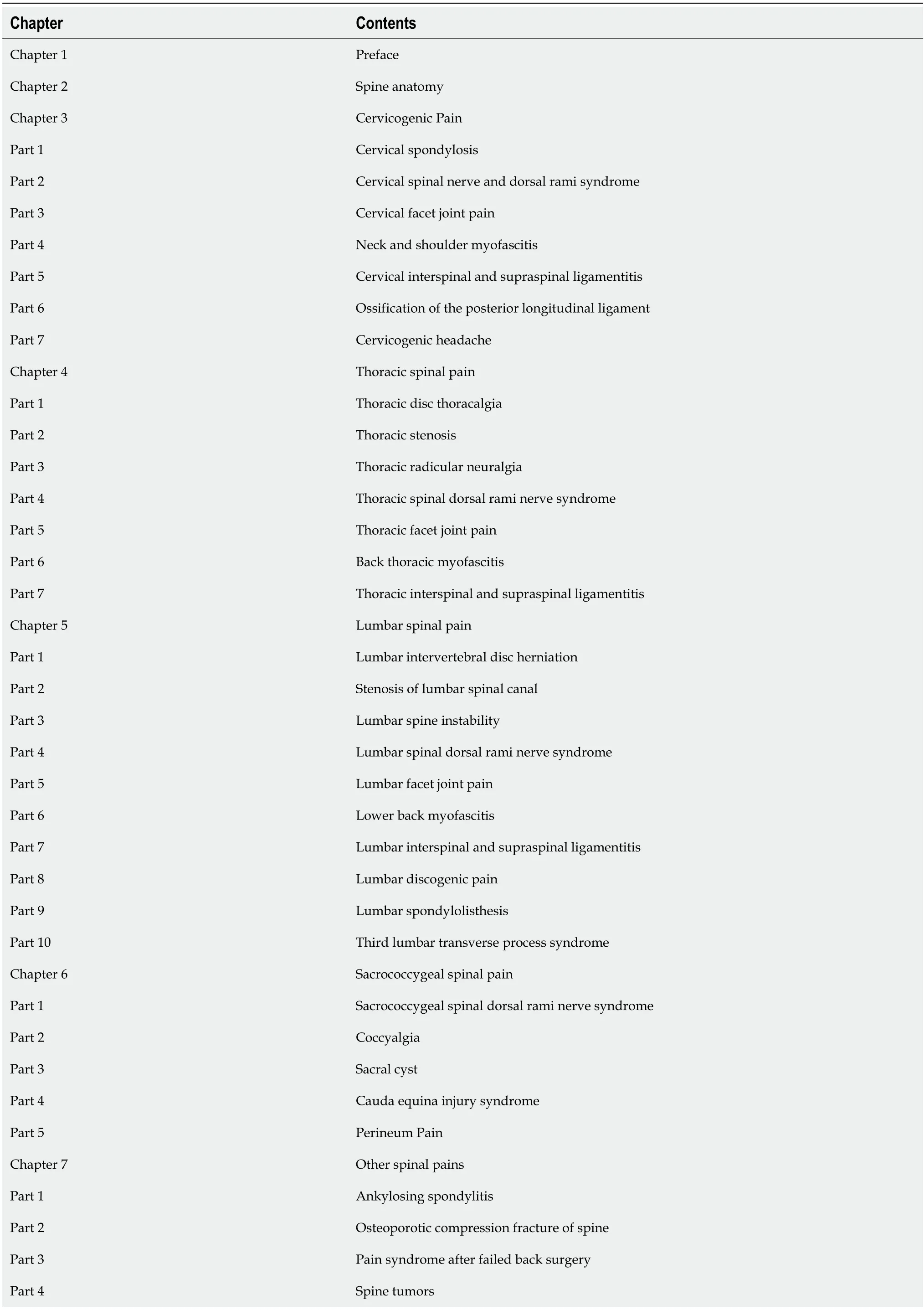
Table 1 Contents of Spinal Pain[52] can be used as a reference for the selection of clinical indications for clinical ultrasound-guided injections
?
Patients are required to lie on their lateral sides with the upper limbs placed parallel to the body. After skin disinfection and covering with surgical drapes, the ultrasound scanning is performed from the junction of the posterior part of the neck and the occipital bone. The probe is placed perpendicular to the long axis of the cervical vertebrae and slowly moved from the head side to the tail side. When an “arc”acoustic shadow is detected, this indicates the location of the C1 vertebral laminae. The probe is then gradually moved to the tail side. It indicates the C2 spinous process when an acoustic shadow with a bifurcation is seen. Other spinous processes can be located in this way. The probe can also be placed at the level of the inferior margin of the lateral cricoid cartilage to observe the anterior and posterior tubercle of cervical transverse process. The arm-shaped acoustic shadow can be seen at the level of C7 transverse process since the anterior tubercle is absent in C7 transverse process.Following identification, the probe should be moved to the head side to locate the relevant transverse process of the cervical vertebrae. These two methods should be carried out to confirm the relevant spine segments before injection.
Stellate ganglion block, see Table 2 for more details.
Recommendations: The stellate ganglion may be located in the front of C6, C7, and T1 vertebrae due to anatomic variations[28]. In these cases, injection into the surface of thelongus collishould be used to achieve a blocking effect with local anesthetics diffusing through the prevertebral fascia[29]. At the C6 section, attention should be paid to the obstacle from the anterior tubercle of the C6 transverse process during the stellate ganglion block. The vagus nerve can be easily blocked if the direction of puncture is to the inner side (flat angle). The needle tip may be located in the muscle oflongus colliif the puncture is too deep. Puncture at the C7 section should avoid accidental injuries to the vertebral artery, vertebral vein, cupula pleurae, and phrenic nerve[30-32].
Cervical nerve root block, see Table 2 for more details.
Recommendations: Avoidance of injuries in the vertebral vessel, the radicular artery, the ascending cervical artery, and the deep cervical artery[33]. The drug dosage should be controlled to prevent diffusion into the spinal canal, which results in neuraxial anesthesia or total spinal anesthesia[34].
The cervical zygapophysial joint block, see Table 2 for more details.
Recommendations: The drug dose should be controlled to prevent diffusion into the spinal canal, which would result in neuraxial anesthesia[35-37]. In clinical practice,treatments should not be limited to particular injured zygapophyseal joints. Improved efficacy can be achieved by blocking in the injured zygapophyseal joint, the posterior branch of the inferior nerve root, and the posterior branch superior to the nerve root[38].
The medial branch block of the posterior rami of cervical spinal nerve, see Table 2 for more details.
Recommendations: The puncture plane should be correctly selected. It is important to avoid the injuries to the vertebral artery during the puncture procedure.
Block of the atlantoaxial joint, the medial branch of C2 nerve root and dorsal root ganglion, and the third occipital nerve, see Table 2 for more details.
Recommendations: This procedure should be performed using ultrasound-guided in-plane technique. The probe should be shifted, tilted, and rotated to ensure the puncture needle and target are in the same plane and to ensure the tip and shaft of the puncture needle is completely visible in ultrasound image.
Thoracic spine
The thoracic SP refers to pain that may be caused by many disorders. Specifically,these include disorders of the following: The thoracic nerve root, the thoracic dorsal rami nerve, the intercostal nerve, the lateral branch of the intercostal anterior rami nerve, the anterior cutaneous branch of the intercostal anterior rami nerve, the facetjoint of the thoracic spine, and the costotransverse joint. Morbidity associated with pain in the thoracic vertebra is lower (around 15%) than pain associated with the cervical and lumbar vertebra. Several techniques may be used for ultrasound-guided injection of thoracic SP including nerve root block and neurolysis, paravertebral nerve root block, block of the posterior branch of thoracic nerve and neurolysis, intercostal nerve block and neurolysis, block of the lateral branch of the intercostal anterior rami nerve, intercostal anterior rami nerve block, and neurolysis[39,40]. In addition, thoracic facet joint injection and costotransverse joint injection can also be included[41,42]. All of the techniques listed above can be performed using real-time ultrasound guidance.

Table 2 Contents of the Ultrasound-guided Injection for Spinal Pain Technical Guide
Thoracic nerve root block, see Table 2 for more details.
Recommendations: Withdrawal the syringe before injection to avoid intravascular injection.
Paravertebral nerve root block, see Table 2 for more details.
Recommendations: The drug dose should be controlled to avoid excess drug entering the epidural space that may block or damage the adjacent nerves[43].
Thoracic erector spinae plane block, see Table 2 for more details.
Recommendations: Needle insertion should be performed in- or out-of-plane, and 20 mL of the drug should be injected when the needle tip reaches the target[44].
Intercostal nerve block, see Table 2 for more details.
Recommendations: The intercostal nerve runs along the inferior margin of the target costal. The position of intercostal vessels should be observed using the Doppler effect before puncture. Injury to the pleura needs to be avoided during the needle insertion.In-plane needle insertion should be adopted, with the puncture needle being advanced from the caudal side of the probe. The needle tip may puncture the muscles of the back and the internal and external intercostal muscles located to the inferior margin of the target costal and the shallow surface of the innermost intercostal muscle. No blood present during the syringe withdrawal should be confirmed before injection.
Serratus anterior muscle plane block (lateral branch of intercostal anterior rami nerve), see Table 2 for more details.
Recommendations: The blocking effect is determined by the diffusion of the local anesthetic into the correct layers. The serratus anterior muscle should be identified and the injection should be performed by inserting the puncture needle into the shallow or deep surface of the serratus anterior muscle[45].
Thoracic transverse muscle plane block (anterior cutaneous branch of intercostal anterior rami nerve), see Table 2 for more details.
Recommendations: A striped, high-echo acoustic shadow can be seen in the shallow surface of the internal thoracic artery that is the transverse muscle and the intercostal muscle. The local anesthetic should be injected between these two muscles in order to block the anterior cutaneous branch of the intercostal nerve.
Thoracic zygapophyseal joint block, see Table 2 for more details.
Recommendations: No wide or deep acoustic windows are present between the thoracic zygapophyseal joints. The needle should be inserted in-plane from the caudal side to the cranial side. The drug should be injected after penetrating the articular capsule.
Thoracic retrolaminar block (medial branch of spinal posterior rami nerve), see Table 2 for more details.
Recommendations: The accident injection into the spinal canal through the interlaminar space should be avoided to prevent the neuraxial anesthesia[46].
Costotransverse joint injection, see Table 2 for more details
Recommendations: The in-plane technique is recommended to avoid pneumothorax[42].
Lumbar and sacral spine
The lumbosacral SP refers to pain caused by disorders of relevant structures around the lumbosacral spine. The ultrasound-guided interventional treatments for lumbosacral SP include lumbar and sacral epidural space injection, selective lumbar nerve root block, lumbar zygapophysial joint injection, block of the medial branch of the posterior lumbar nerve, and lumbar sympathetic ganglion block[47-50].
Ultrasound-guided lumbar epidural block, see Table 2 for more details.
Recommendations: Lumbar epidural space injection is a common technique used in clinical pain management. The success rate of difficult epidural access can be improved under ultrasound guidance. The paramedian sagittal oblique scanning and paramedian transverse scanning are often used for the ultrasound-guided epidural access. The ultrasound probe in the paramedian sagittal scanning technique is located 1-2 cm adjacent to the spine, with the scanning direction in line with the sagittal axis of the spine, and tilted towards the central line of the spine. The inferior margin of the ultrasound probe in the paramedian transverse scanning technique is located 3-4 cm adjacent to the spine midline, with the scanning direction vertical to the sagittal axis of the spine, and tilted towards the central line of the spine. The in-plane technique is suggested to avoid puncturing the dura mater[47,51].
Ultrasound-guided sacral epidural block, see Table 2 for more details
Recommendations: The sacral epidural block is widely used in sacral SP treatments.Since there are many variations of the sacral hiatus in adults that have associated difficulties during puncture, ultrasound guidance can improve the success rate of the sacral epidural block. The block can be performed with the short-axis out-of-plane technique or with the long-axis in-plane technique. The location of ultrasound probe in the short axis technique is perpendicular to the long axis of the spine; whilst in the long-axis technique, it is in the same direction of the long axis of the spine.
Ultrasound-guided selective lumbar nerve block, see Table 2 for more details.
Recommendations: Selective lumbar nerve block can be used for both diagnosis and treatment purposes. Compared to X-ray and computed tomography guided techniques, ultrasound-guided selective lumbar nerve block has a success rate of more than 90% and the advantage of reducing radiation exposure. Paramedian transverse scanning should be adopted in the selective L1-L4 nerve root block. The ultrasound probe should be placed perpendicular to the sagittal axis of the spine, 3-4 cm from the midline of the spine. Selective L5 nerve root block adopts paramedian transverse scanning in the triangle area of the lumbar, sacrum, ilium triangle.
Ultrasound-guided block of the lumbar zygapophysial joint and medial branch of the posterior lumbar nerve, see Table 2 for more details.
Recommendations: Lower back pain caused by degeneration of the lumbar facet joint and inflammatory stimulation of the facet joint capsule is termed lumbar facet joint syndrome. Treatments of this syndrome include lumbar facet joint injection,medial branch block of the posterior lumbar nerve, and radiofrequency ablation of the medial branch of the posterior lumbar nerve. Medial branch block of the posterior lumbar nerve can be used for both diagnosis and treatment, which can relieve lower back pain in the long term through multiple blocks. Disorders of one lumbar facet joint should be treated with a block or radiofrequency ablation in the same segment, as well as the superior segment of the medial branch of the posterior lumbar nerve[50].
Ultrasound-guided lumbar sympathetic ganglion block, see Table 2 for more details.
Recommendations: Lumbar sympathetic ganglion block is used to treat sympathetic nerve pain of the lower limbs and vasospastic disease. The block is usually performed under X-ray or computed tomography image guidance. Ultrasound-guided lumbar sympathetic ganglion block can be applied to slim patients, with puncture making full use of the Doppler effect. This avoids injury of the vessels around the vertebrae. Dual guidance of X-ray and ultrasound are often applied in clinical practice.
CONCLUSION
This expert consensus was proposed by domestic experts working on ultrasoundguided pain treatments to guide clinicians and medical experts on the correct use of ultrasound-guided injections for SP.
 World Journal of Clinical Cases2021年9期
World Journal of Clinical Cases2021年9期
- World Journal of Clinical Cases的其它文章
- Expert panel’s guideline on cervicogenic headache: The Chinese Association for the Study of Pain recommendation
- Expert consensus of Chinese Association for the Study of Pain on the application of ozone therapy in pain medicine
- Chinese Association for the Study of Pain: Expert consensus on diagnosis and treatment for lumbar disc herniation
- Expert consensus on the diagnosis and treatment of myofascial pain syndrome
- Chinese Association for the Study of Pain: Expert consensus on chronic postsurgical pain
- Expert consensus of the Chinese Association for the Study of Pain on ion channel drugs for neuropathic pain