
Systemic adverse effects and toxicities associated with immunotherapy: A review
2021-04-02 08:03AsimKichlooMichaelAlbostaDushyantDahiyaJeanClaudeGuidiMichaelAljadahJagmeetSinghHafeezShakaFarahWaniAkshayKumarManidharLekkala
Asim Kichloo, Michael Albosta, Dushyant Dahiya, Jean Claude Guidi, Michael Aljadah, Jagmeet Singh, Hafeez Shaka, Farah Wani, Akshay Kumar, Manidhar Lekkala
Asim Kichloo, Michael Albosta, Dushyant Dahiya, Department of Internal Medicine, Central Michigan University, Saginaw, MI 48603, United States
Asim Kichloo, Jean Claude Guidi, Department of Internal Medicine, Samaritan Medical Center,Watertown, NY 13601, United States
Michael Aljadah, Department of Internal Medicine, Medical College of Wisconsin, Milwaukee,WI 53201, United States
Jagmeet Singh, Department of Nephrology, Guthrie Robert Packer Hospital, Sayre, PA 18840,United States
Hafeez Shaka, Department of Internal Medicine, John H Stroger Jr. Hospital of Cook County,Chicago, IL 60612, United States
Farah Wani, Department of Family Medicine, Samaritan Medical Center, Watertown, NY 13601, United States
Akshay Kumar, Department of Surgery, University of Pittsburgh, Pittsburgh, PA 15213, United States
Manidhar Lekkala, Department of Hematology and Oncology, University of Rochester Medical Center, Rochester, NY 14642, United States
Abstract Immunotherapy is rapidly evolving secondary to the advent of newer immunotherapeutic agents and increasing approval of the current agents by the United States Food and Drug Administration to treat a wide spectrum of cancers.Immunotherapeutic agents have gained immense popularity due to their tumorspecific action. Immunotherapy is slowly transforming into a separate therapeutic entity, and the fifth pillar of management for cancers alongside surgery,radiotherapy, chemotherapy, and targeted therapy. However, like any therapeutic entity it has its own adverse effects. With the increasing use of immunotherapeutic agents, it is vital for physicians to acquaint themselves with these adverse effects. The aim of this review is to investigate the common systemic adverse effects and toxicities associated with the use of different classes of immunotherapeutic agents. We provide an overview of potential adverse effects and toxicities associated with different classes of immunotherapeutic agents organized by organ systems, as well as an extensive discussion of the current recommendations for treatment and clinical trial data. As we continue to see increasing usage of these agents in clinical practice, it is vital for physicians to familiarize themselves with these effects.
Key Words: Immunotherapy; Cancer; Malignancy; Adverse effects; Immune checkpoint inhibitor; Monoclonal antibody
INTRODUCTION
Immunotherapy has become an increasingly popular therapeutic option for patients suffering from a variety of malignancies over the past several years. The development of these therapies began nearly two decades ago, when Leachet al[1]discovered that inhibition of cytotoxic T-lymphocyte associated protein 4 (CTLA-4)in vivoled to the rejection of tumor cells. Furthermore, in 2004, Chen described the role of programmed cell death protein 1 (PD-1) and programmed death-ligand 1 (PD-L1) in the suppression of T-cell responses in the tumor microenvironment[2]. These discoveries have sparked extensive research in the field of immunotherapy, ultimately leading to the approval of ipilimumab (CTLA-4 inhibitor) by the United States Food and Drug Administration(FDA) for the treatment of melanoma in 2011[3]. Since then, immunotherapy has attracted immense attention as a therapeutic modality. The idea behind the utilization of these agents is based upon the premise of using the body’s own immune system to attack and destroy cancerous cells[4]. Currently, immunotherapeutic agents have been approved for a wide variety of malignancies, including but not limited to melanoma,non-small cell lung cancer, colorectal cancer, bladder cancer, breast cancer, and head and neck cancers[5]. Although the success of these therapies has been well documented,the literature does report significant side effects closely associated with their use,known as immune related adverse effects (irAE). In this review, we provide a systembased overview of the documented adverse effects associated with the use of immunotherapy. It is essential for care providers to know these systemic adverse effects and toxicities when prescribing these agents for the treatment of cancers.
CLASSES OF IMMUNOTHERAPY AGENTS AND MECHANISMS
Immunotherapy works by stimulating the body’s own immune system to target cancerous cells. With a better understanding of the workings of the immune system and the identification of new molecular targets, the classes of agents continue to grow.Currently, immunotherapeutic agents can be classified into 5 major types including[6,7]:Immune checkpoint inhibitors (ICI); Adoptive cell therapy; Monoclonal antibodies;Treatment vaccines; Immune system modulators.
The National Institute of Health along with the approval of immunotherapeutic agents from the FDA have led to the recommendations for use of these agents in different types of cancers as summarized in Table 1. The mechanism of action of the 4 most frequently used immunotherapeutic agents is described as follows (see Table 2 for an overview of individual immunotherapeutic agents and their proposed mechanisms): (1) ICIs work through therapeutic targeting of the checkpoint molecules CTLA-4, PD-1, and PD-L1, which are normally utilized by healthy cells to promote self-tolerance and inhibit destruction by autoreactive T-cells[8]. However, tumor cells often utilize these proteins to avoid T-cell mediated destruction. By utilization of the ICIs, T-cells may have a greater ability to recognize tumor cells as foreign entities and promote cell lysis; (2) T-Cell transfer therapy is a treatment method in which a patient’s T cells are collected and modified in a laboratory setting in order to improve their ability to bind and kill cancer cells. By collecting activated T-cells from cancer tissue, or genetically engineering T-cells, transfer therapy allows for passive immunization against cancers[9]; (3) Monoclonal antibodies are engineered to be antigen specific, often tumor-specific, and mediate the destruction of tumor cellsviaantibody-dependent cell-mediated cytotoxicity, promotion of phagocytosis or complement activation (referred to as complement-dependent cytotoxicity), or vascular and stromal ablation. A multitude of monoclonal antibodies have been developed to target various endogenous molecules[10]; and (4) Therapeutic cancer vaccines deliver concentrated antigen to both HLA class I and II molecules of antigen presenting cells, promoting both CD4 and CD8 T-cell responses which help to generate an anti-tumor response[11].
SYSTEM BASED CONSEQUENCES OF IMMUNOTHERAPEUTIC AGENTS
The following sections, organized by organ system, will describe and detail the potential adverse effects and toxicities associated with the use of currently approved immunotherapeutic agents. The systems specific adverse effects described are presented in the context of following systems: Cardiovascular, dermatologic,endocrine, gastrointestinal, neurologic, and pulmonary. In addition, we will provide an overview of some of the adverse events unique to chimeric antigen receptor (CAR)T-cell therapy.
CARDIOVASCULAR
The cardiovascular consequences of immunotherapeutic agents are being increasingly documented in medical literature, especially with the use of ICIs. The reported adverse effects can be further classified into two specific subtypes including structural, such as pericarditis and myocarditis, and arrhythmogenic, such as sick sinus syndrome.Cardiotoxicity has been most frequently reported with the use of ICIs and CAR T-cell therapy.
Structural consequences
The structural consequences may manifest in several ways. Patients may be asymptomatic, but laboratory investigations may report elevated markers of myocardial necrosis[12]. Furthermore, they can present with systolic dysfunction,symptoms of myocarditis, pericarditis, pericardial effusions, cardiac tamponade, or stress induced cardiomyopathies[12]. Structural cardiotoxicity secondary to the use of immunotherapy may be life-threatening and high suspicion for early recognition is imperative to prevent adverse outcomes.
The cause of cardiotoxicity due to immunotherapy is still largely under investigation. For immune checkpoint inhibitors, the presence of similar T-cell receptor sequences in tumor and in cardiac muscle is presumed to be the reason for myocardial and pericardial inflammation[13]. Furthermore, this can be confirmed with histopathological findings of fibrinous exudates with lymphocyte, plasma cell, and macrophage infiltration in patients with pericarditis[14]. Additionally, histopathological findings of endomyocardial CD8+ T-cell cells on post-mortem biopsy of those who had myocarditis secondary to immune checkpoint inhibitors also supports thistheory[15]. With respect to CAR T-Cell therapy, the mechanism of action of cardiotoxicity is presumed to be secondary to a cytokine storm generated by the reprogrammed T-cells leading to cardiovascular collapse[13]. Furthermore, like immune checkpoint inhibitors, common antigens between cardiac tissues and tumor cells,specifically the protein titin, has been hypothesized as a mechanism of action of cardiotoxicity from CAR T-cell therapy[13].

Table 1 Immunotherapy agents approved for treatment by the United States Food and Drug Administration in various types of cancers
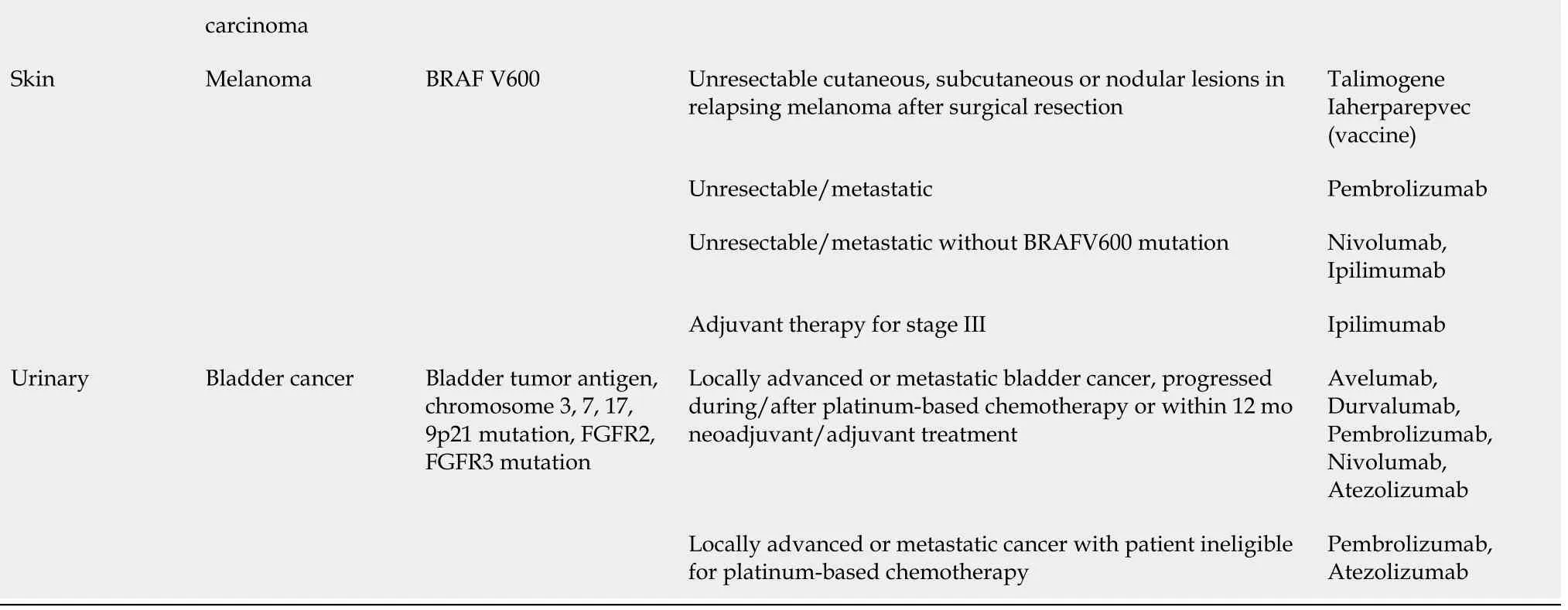
GBM: Glioblastoma multiforme; SCC: Squamous cell carcinoma; SSC-Ag: Squamous cell carcinoma antigen; CLL: Chronic lymphocytic leukemia; ALL:Acute lymphoblastic leukemia; HSCT: Hematopoietic stem cell transfer; NSCLC: Non small-cell lung carcinoma.
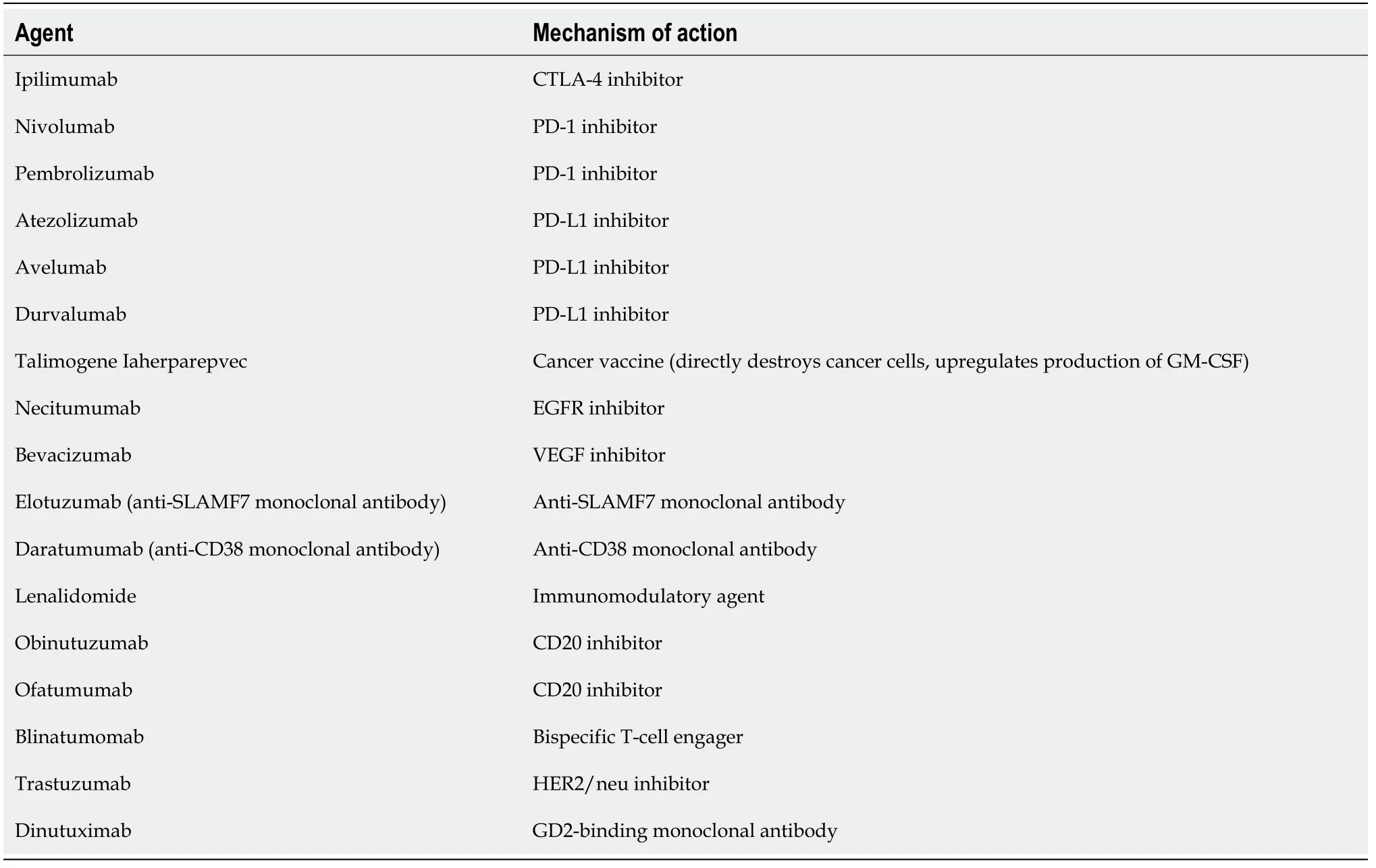
Table 2 Overview of some of the common immunotherapeutic agents and their proposed mechanisms
The literature also reports structural consequences with the use of monoclonal antibody therapy. Patient’s with non-small-cell lung cancer treated with pembrolizumab, a PD-1 inhibitor, were found to have immune-mediated pericarditis[16].Additionally, trastuzumab, a HER2 receptor blocker used in breast cancer treatment, is commonly known to cause cardiotoxicity. While the exact mechanism of cardiotoxicity is unknown, studies have shown that the structural changes are different from those found with anthracyclines[17]. The most current hypotheses focuses on trastuzumab’s interference in the integral HER2 signaling cascade resulting in the accumulation of toxic metabolites leading to cardiotoxicity. However, the exact molecular contributor is still unknown[18].
Treatment for the cardiotoxicity is centered around treating the over-active T-cell response with therapies such as high dose intravenous steroids, immunosuppressants,plasmapheresis, and intravenous immunoglobulins[14]. Furthermore, cessation of therapy should be considered with persistent cardiac symptoms longer than three months, if immunosuppressive therapy will need to be ongoing, or if there is evidence of life-threatening side-effects[14].
Rhythm consequences
Arrhythmias that have been well documented in the setting of immunotherapy use include atrial fibrillation, supraventricular arrhythmias, ventricular arrhythmias, and heart blocks[15].
The cause of rhythm consequences secondary to the use of immunotherapy is also still largely under investigation with even less knowledge about the mechanism when compared to structural consequences. If an arrhythmia presents in the setting of immunotherapy use, it is most often a result of persistent myocarditis that disrupts cardiac conduction[15]. However, post-mortem histopathologic analysis has demonstrated lymphocyte infiltration in both the sinoatrial node and the atrioventricular node, which provides strong evidence for a T-cell mediated insult similar to the mechanism of action of structural cardiotoxicity[15].
Patients who develop arrhythmias in the setting of immunotherapy should be treated with antiarrhythmics[15]. If the arrhythmia persists, an evaluation for a permanent pacemaker should be considered[15]. Similarly to structural consequences,cessation of immunotherapy should be considered with persistent cardiotoxic side effects and evidence of life-threatening consequences[14].
DERMATOLOGICAL
Dermatologic toxicities are extremely common with immunotherapy, most commonly resulting in a maculopapular rash and pruritis[19]. However, lichen dermatitis,psoriasis, bullous pemphigoid, as well as life-threatening adverse events like erythema multiforme or Stevens-Johnson syndrome (SJS) have also been reported[19].
The exact mechanism of causation of these lesions is not well understood, but several hypotheses have been put forth. Antibodies directed against melanomaassociated antigens can cross-react with the antigens produced by normal melanocytes. The presence of a Vitiligo-like lesion has been associated with higher objective tumor response rates.
Monoclonal antibodies are also frequently linked to dermatological adverse events.Rituximab, a CD20 antagonist, has been associated with morbilliform skin eruptions or even SJS, with the former requiring steroid therapy, while the latter requires immediate discontinuation of the agent[20]. Anakinra, an IL-1 antagonist, is associated with new-onset psoriasis as well as injection-site reactions. Tocilizumab, an IL-6 receptor antagonist, may rarely present with skin rash[20]. Ipilimumab, a CTLA-4 inhibitor used in the treatment of melanoma, has a diverse range of dermatologic adverse effects associated with its use such as rashes, folliculitis, mucositis, rosacea,SJS and vitiligo[20].
It is highly recommended for patients to undergo a dermatologic exam prior to starting immunotherapy to establish a baseline[19]. Depending on the severity of the condition, topical or systemic corticosteroids can be considered. However, prompt discontinuation is necessary in the event of severe reactions such as SJS[20]. Early detection and prompt management of these reactions is necessary as they profoundly diminish quality of life.
ENDOCRINE
Endocrine irAEs are also well documented, with the most common being acute hypophysitis and thyroid dysfunction[21]. Additionally, adrenal insufficiency,pancreatic dysfunction resulting in worsening glycemic control with subsequent diabetic ketoacidosis (DKA) or hyperosmolar hyperglycemic state, and hypoparathyroidism have also been reported[21]. These adverse events are most commonly associated with ICI therapy. Conversely, oncolytic viruses, adoptive T-cell transfer,and cancer vaccines may rarely cause endocrinological dysfunction[22]. Currently, there are no specific recommendations for the screening of patients on ICI therapy for endocrine dysfunction, thereby making establishing a diagnosis of endocrine irAE quite challenging. Therefore, it is of critical importance that care providers monitor these patients closely to avoid morbidity and mortality secondary to the use of these therapeutic agents. The specific endocrine system related side effects, including proposed mechanism, presentation, and management strategies are discussed in detail in the following sections.
Thyroid
As discussed, thyroid dysfunction is one of the most common irAEs secondary to the use of ICI therapy. The mechanism of the development of thyroid dysfunction is currently being studied; however, there are several theories that have been proposed as the possible cause. First, it is assumed that increased immune system activation secondary to the use of ICIs may lead to an enhanced cytotoxic immune reaction that damages healthy tissue[23]. Second, it has been recognized that patients suffering from autoimmune damage associated with ICIs have an increase in the HLA-DR expression on CD14+CD16+ monocytes[23]. Some investigators have hypothesized that this overexpression may lead to excess monocytic activation, which infiltrate the thyroid gland, recognize self-antigens and induce subsequent cytotoxic damage to the normal cells[23]. However, it is not entirely clear whether the monocytes are directly responsible for the cytotoxic damage, or whether the damage is mediated by monocyte-activated autoreactive CD8+ T-cells. It has been well recognized that the incidence of autoimmune thyroid dysfunction occurs at much higher rate with PD-1/PD-L1 inhibitors as compared to CTLA-4 inhibitors. It is believed that this observation could be because healthy thyroid tissue has an increased expression of PD-L1, or because intra-thyroid lymphocytes have lower CTLA-4 expression[23].
Thyroid dysfunction could lead to features of hypo- or hyperthyroidism in these patients. Symptoms of hypothyroidism include fatigue, cold intolerance, weight gain,constipation, and hair loss, among many others. These patients may present with elevated Thyroid stimulating hormone (TSH) and low levels of T4. According to a retrospective cohort study by Maet al[24], the median time to onset of hypothyroidism in patients receiving pembrolizumab (PD-1 inhibitor) was found to be 84 d (range: 43-544;P= 0.333) . For those receiving nivolumab (PD-1 inhibitor) and ipilimumab(CTLA-4 inhibitor) + nivolumab (PD-1 inhibitor), the median time to onset was 84 d(range: 14-154;P= 0.002) and 62 d (range: 21-141;P= 0.057) respectively[24].
Patients may also present with thyrotoxicosis, often secondary to thyroiditis or Graves’ disease[21]. These patients will have typical features of hyperthyroidism such as weight loss, palpitations, tremors, diarrhea, and heat intolerance. Furthermore, many patients may commonly be asymptomatic, with the hyperthyroid state uncovered on routine laboratory investigations[21]. Maet al[24]found that the median time to onset of thyrotoxicosis in patients treated with pembrolizumab (PD-1 inhibitor) was 44 d(range: 19-447;P= 0.593), while time for those receiving nivolumab (PD-1 inhibitor)was 56 d (range: 13-126;P= 0.004) and ipilimumab (CTLA-4 inhibitor) + nivolumab(PD-1 inhibitor) was 21 d (range: 7-64;P= 0.158). It is abundantly evident from these studies that the use of combination therapy leads to a more rapid symptom onset.
The treatment of thyroid dysfunction in these patients varies and depends on several factors such as whether the patient is suffering from hypo-vshyperthyroidism,the severity of symptoms, and whether additional intervention such as hospitalization or surgery are indicated. The Society for Immunotherapy of Cancer has put forth guidelines for patients with hypothyroidism. These guidelines recommend that patients with severe symptoms with limitations of activities of daily living should discontinue ICI therapy, and should start standard thyroid replacement therapy[21].Additionally, TSH and free T4 should be repeated after 6-8 wk of therapy to allow for titration of the dose. Resolution of symptoms is not needed prior to restarting ICI therapy, and these patients may resume ICI therapy once symptoms are no longer limiting self-care activities of daily living[21]. For patients with hyperthyroidism, the recommendation for discontinuation of ICIs is similar. In patients with severe symptoms that limit self-care activities of daily living, ICI should be discontinued immediately. Additionally, patients may benefit from beta-blockers for symptomatic improvement of hyperthyroid symptoms[21]. Of note, corticosteroids are not required for patients with thyroid irAEs.
Pancreas
Another frequently effected organ is the pancreas, as patients on ICIs have been reported to have diabetes as a consequence of the therapy[25]. These patients frequently present with symptoms consistent with DKA and may be subsequently diagnosed with new onset type 1 diabetes mellitus. However there have also been reports of insidious worsening of type 2 diabetes mellitus presenting as ketoacidosis as well[25,26].The pathophysiology of the development of diabetes in these patients is not well understood, but it is postulated that it may be due to autoreactive CD8+ T cell activation against pancreatic beta cells as a consequence of the blockade of inhibitory pathways, such as the PD-1/PD-L1 pathway[27]. Patients may present with symptoms typical of hyperglycemia or ketoacidosis, including polyuria, polydipsia, weight loss,nausea, and vomiting. In a review of cases reported by Tanet al[25], it was found that the median onset of clinical presentation was 7.5 wk after starting ICI therapy,although cases have been described as early as one week or as late as one year after initiation. While more than two-thirds of the patients presented in DKA, only about 50% had positive auto-antibodies (anti-GAD, anti-insulin, anti-islet cell A, anti-zinc transport 8)[25].
Patients presenting with features of DKA should discontinue ICI therapy immediately and should be managed according to standard guidelines for DKA management[21]. If patients do not have DKA, but fasting glucose is in the 250-500 mg/dL range, ICI should also be held and the patient should be treated with insulin with a goal of fasting glucose level below 160 mg/dL[21]. All patients with new onset diabetes secondary to the use of ICIs should receive an endocrinology consultation.
Pituitary/adrenal insufficiency
Pituitary dysfunction and adrenal insufficiency have also been well documented irAEs of ICI therapy. In a meta-analysis conducted by Luet al[28], the incidence of adrenal insufficiency was found to be 2.43% (95%CI: 1.73%-3.22%), while the rate of hypophysitis was reported to be 3.25% (95%CI: 2.15%-4.51%). Hypophysitis most frequently occurs secondary to CTLA-4 inhibitor therapy[28]. The specific mechanism is not well understood; however, multiple theories are currently being investigated. First,similar to all irAEs, it is believed that inhibition of self-tolerance leads to an autoimmune response against pituitary endocrine cells[29]. It has also been shown that CTLA-4 expression is greater on endocrine cells of the pituitary gland, especially prolactin and TSH secreting cells, which could possibly explain as to why both pituitary and thyroid dysfunction are the most common irAEs, and why symptoms occur more frequently in patients receiving CTLA-4 inhibitor therapy[29]. Patients may present with symptoms of headache, vision changes, and fatigue[21]. If patients subsequently develop adrenal insufficiency secondary to pituitary dysfunction,symptoms may include abdominal pain, vomiting, weakness, fatigue, hypotension,weight loss, and features of adrenal crisis. Additionally, the loss of function of other anterior pituitary hormones (FSH, LH, ACTH, TSH, Prolactin, GH) may lead to presenting symptoms consistent with the effects of the deficient hormone. Literature reports the median onset of clinical presentation to be 12 wk (range 3-76 wk) from initiation of ICI therapy.
Management of the pituitary dysfunction is focused on the replacement of the deficient hormone. In patients with adrenal insufficiency, steroids should be started to replace the corticosteroid deficit[21]. ICI therapy should be held in patients with moderate symptoms requiring local or non-invasive intervention, who have some limitation of instrumental activities of daily living[21]. ICI may be resumed when an initial work up is completed and the hormone replacement has begun[21].
GASTROINTESTINAL
The literature reports abundant gastrointestinal (GI) adverse effects associated with the use of immunotherapeutic agents. These have been reported across every class of immunotherapeutic agent, except for therapeutic cancer vaccines. In contrast to other cytotoxic therapies, cancer vaccines have reported minimal toxicities in a majority of clinical trials[30]. However these therapies are largely still in the development phase and adverse events will most likely be elucidated in the future.
The side effects associated with ICIs tend to be mild and transient with watery, nonbloody diarrhea being the most commonly reported[31]. Colitis, presenting with bloody diarrhea and fever, has also been reported. Typically, these adverse effects are more frequent with anti-CTLA-4 and anti-PD-1 agents[32]. Mouth ulcers, anal lesions like fistulas, abscesses or fissures, and other extra-intestinal manifestations may also occur[33]. Some patients may also have asymptomatic elevation in the liver function tests[34]. Although the upper GI tract is rarely involved, some reported adverse effects include gastritis, esophagitis and aphthous ulcers[32].
The management of GI adverse effects as a result of ICI therapy is stratified based on the severity of the diarrhea or colitis. They are graded from 1-5 based on the severity, number of stools per day, and the need for hospitalization or additional intervention[35,36]. Treatment typically ranges from supportive (antidiarrheals,fluids/electrolytes) to hospitalization (IV corticosteroids and discontinuation of immunotherapy). Life threatening enterocolitis with perforation requires immediate surgical intervention.
T-cell therapy is associated with on-target adverse effects which are usually not lifethreatening but may be treatment limiting. These on-target adverse effects are expected as the engineered T-cells may share specific target antigens with different organ systems with the most common T-cell adverse event being colitis[37]. The decision to discontinue T-cell therapy should be individualized to the patient and based on the severity of illness.
Monoclonal antibody agents have also been associated with diverse GI toxicities.Anti-angiogenic agents such as bevacizumab (VEGF inhibitor) and aflibercept (VEGF inhibitor) have been associated with dose-dependent GI perforations[38]. It is hypothesized that this may be due to ischemia secondary to limitation of blood flow to the GI tract[39]. The management of GI perforation includes prompt surgical intervention, bowel rest, and initiation of intravenous antibiotics. It has been reported that EGFR inhibitors such as cetuximab and panitumumab have a 66% increased risk of diarrhea compared to chemotherapy alone[40]. Hypomagnesemia is another common adverse effect of EGFR inhibitor therapy. It is dependent on the duration of the therapy and could possibly be the result of chronic diarrhea[41]. The management of diarrhea consists of bowel rest, hydration, electrolyte repletion, and the use of antimotility agents. Hospitalization may be necessary in patients with severe dehydration.Finally, Trastuzumab (HER2/neu inhibitor) has been found to be associated with a higher prevalence of diarrhea compared to chemotherapy alone[42].
NEUROLOGICAL
Although rare, neurological irAEs are well reported side effects of ICI therapy,occurring in 1% of patients receiving monotherapy and 2%-3% of patients receiving a combination of ICIs[43]. Median onset of symptom occurrence is 6 wk; however,symptoms have been shown to occur as early as after the first dose and as late as at the 68thweek after initiation of therapy[43]. Neurologic events are more commonly reported with CTLA-4 inhibitor therapy[44].
Numerous neurologic irAE have been reported. These include inflammatory myopathies, myasthenia gravis, vasculitis, small fiber sensory type neuropathies,immune-mediated neuropathies, cranial mononeuropathies, aseptic meningitis,autoimmune encephalitis, and multiple sclerosis (both exacerbation and new onset CNS demyelinating disease)[44]. The presentation is largely dependent on the type of irAE. The mechanism for neurological symptoms is most likely due to the increased Tcell and macrophage activation secondary to immune checkpoint inhibition, leading to autoimmune damage to parts of the nervous system[45]. Furthermore, it has been suggested that the aberrant T-cell activation and release of inflammatory cytokines may lead to sub-perineural edema and inflammation of the endoneurial microvessels,which is in part responsible for the nervous system dysfunction[46]. The treatment of the neurological adverse effects depends on the severity of the symptoms.
For any neurologic irAE, ICI therapy should be paused immediately, with considerations for possible permanent discontinuation of therapy if symptoms are severe (limiting ability to perform self-care activities of daily living) or progressive[21].Moreover, patients with moderate symptoms or greater, based on limitation of daily activities, should be started on methylprednisolone (0.5 to 1.0 mg/kg/d for moderate;1-2 mg/kg/d for severe) after a central nervous system infection has been ruled out as a cause of the neurologic dysfunction[21]. Additionally, in patients with involvement of the respiratory muscles, admission to the intensive care unit for close observation and ventilator therapy may be warranted[46]. The decision to restart the patient on immunotherapy should be a joint decision between the patient, oncologist and the neurology consultant.
Monoclonal antibodies and cancer vaccines have not demonstrated consistent evidence of causing adverse neurological consequences. However, additional research is required to elucidate whether this is due to a lack of evidence or the true absence of adverse effects.
PULMONARY
The most frequently cited pulmonary adverse effects of immunotherapy are interstitial lung disease and concomitant pneumonitis. Ipilimumab, a CTLA-4 inhibitor, has been shown to be a common agent responsible for pulmonary adverse effects[47]. Most clinical trials reported a 3%-5% incidence of pneumonitis following treatment with immunotherapy. Studies by Delaunayet al[47]and Naidooet al[48]reported that the incidence was higher in current or ex-smokers. A recent metanalysis by Jianget al[49]investigated fatal immune-related adverse events by checkpoint inhibitors, with ten out of twelve trials evaluating CTLA-4 inhibitors. Based on the analysis, CTLA-4 inhibitors had a higher risk of fatal adverse events of pulmonary toxicity, with an overall risk of 20.5% (OR = 3.48,P= 0.10). A subgroup analysis was also performed according to the different dosing regimens and it was reported that the occurrence of toxicity with a 10 mg/kg dose was greater when compared to a 3 mg/kg dose (dosedependent toxicity)[49]. The study by Nishinoet al[50]reviewed ten different nivolumab(PD-1 inhibitor) trials alone or in combination with other immune checkpoint inhibitors for advanced cancers such as melanoma, lung cancer, and lymphoma, and identified pneumonitis in 11.8% patients. Radiological findings of sarcoid-like granulomatosis has also been reported in a patient receiving both anti-CTLA4 and anti-PD-1 agents. Dose-related adverse effects are less frequently encountered with the use of PD-1 inhibitors, and most toxicities are similar at doses ranging from 0.3 to 10 mg/kg.
The preferred initial modality for identifying features of pneumonitis is computed tomography scan. Pneumonitis can be classified as grade 1 with subclinical radiographic changes, grade 2 with mild dyspnea and cough, grade 3 and 4 with severe and life-threatening symptoms, and radiographic findings suggestive of acute interstitial pneumonia, acute respiratory distress syndrome, and/or cryptogenic organizing pneumonia[51]. The base of the lungs are most frequently involved, followed by the middle and upper regions; however, most often it may be mixed and multifocal.Bronchoalveolar lavage may be helpful in patients with cellular interstitial pneumonitis in that the fluid may show lymphocytosis, however there have been relatively few reports describing this finding and further research is needed[53].
The first step in management of all cases is the discontinuation of the immunotherapy, and initiation of corticosteroids[51]. The average duration of corticosteroid therapy also varies, but in most cases the median time is about 6.1 wk. Grade 1 Pneumonitis can be treated by interrupting immunotherapy, whereas grade 2 responds to oral corticosteroids. Grade 3 and 4 may need IV steroids, with some cases requiring infliximab, mycophenolate, tocilizumab, and IL-1 targeted agents[51].
Restarting immunotherapy in these patients is a challenge as pneumonitis can reoccur at any time; hence, close follow-up is recommended. Reinitiating ICIs can lead to recurrence of Pneumonitis in up to 33% of cases[52]. A flare of Pneumonitis can also occur during the steroid taper phase, and manifest similar to the initial episode. Data shows that steroids are responsive in subsequent flares as well as recurrence.Additionally, another challenging scenario is the relationship between radiotherapy and chemotherapy in aiding the development of side effects when used both prior to the initiation of immunotherapy as well as in combination with it[52].
TOXICITY RELATED TO CAR T-CELL THERAPY
CAR T-cell therapy is a type of T-cell transfer therapy currently approved for the treatment of several hematologic malignancies, including acute lymphoblastic leukemia and diffuse large B-cell lymphoma[53]. The mechanism of action involves the creation of CAR T-cells directed against the CD19 protein, which is present on Bcells[53]. While this treatment modality has proven effective in destroying chemotherapy-resistant tumor cells, it does not come without its own adverse events. It is thought that the irAEs resulting from CD19-directed CAR T cells are due to the fact that these modified T cells maintain their native receptors, and have the potential to expand rapidly once activatedviainteraction with the CD19 antigen[54]. These cells then have the potential to damage normal tissues expressing non CD19 antigens[54].Several irAEs have been reported, including cytokine release syndrome (CRS),neurotoxicity, and hematologic abnormalities such as B cell aplasia, hypogammaglobulinemia, anemia, or thrombocytopenia[55].
CRS is an overwhelming release of cytokines, especially IL-1 and IL-6, that occurs as a result of CAR T-cell therapy. According to a review by Longet al[55], it may occur in up to 90% of patients. The symptoms of CRS vary greatly, and can involve a number of different organ systems. One of the most common symptoms is fever, and initial symptoms may mimic an acute infectious process[56]. In addition, there are several lifethreatening complications that have been reported, including cardiac dysfunction,acute respiratory distress syndrome, neurologic toxicities, renal failure, hepatic failure,and hypercoagulability[55,56].
Laboratory findings in CRS are variable. Inflammatory markers such as C-reactive protein are often elevated[57]. In addition, patients may present with leukocytosis or leukopenia, anemia or thrombocytopenia, and elevated levels of D-dimer or ferritin[57].Elevated levels of inflammatory cytokines, such as interferon gamma, IL-6, IL-10, or IL-2 may be present[57]. It should be noted that elevated levels of IL-6 are often found in CAR T-cell therapy induced CRS[57].
The National Cancer Institute Common Terminology Criteria for Adverse Events(CTCAE v5.0) has established a grading system to assess the severity of CRS[58]. The grading criteria for CRS according to the CTCAE v5.0 can be classified as follows[58]:Grade 1: Fever with or without constitutional symptoms; Grade 2: Hypotension responding to fluids; hypoxia responding to < 40% O2; Grade 3: Hypotension managed with one pressor; hypoxia requiring ≥ 40% O2; Grade 4: Life-threatening consequences;urgent intervention indicated; Grade 5: Death.
The management of CRS is centered around preventing life-threatening effects of the syndrome while allowing for the CAR T-cells to continue their anti-tumor activity[56]. For patients with grade 1 CRS, supportive care may be most appropriate treatment option[56]. Patients with grade 2 CRS may be treated conservatively, however for patients with extensive comorbidities and those of advanced age, treatment with Tocilizumab (IL-6 receptor inhibitor) and corticosteroids should be considered[56].Finally, patients with grade 3 or 4 CRS should be admitted to the intensive care unit and treated with Tocilizumab (IL-6 receptor inhibitor) and corticosteroids.Tocilizumab has been evaluated and has been found to have considerable efficacy as a treatment option for CAR T-cell induced CRS[56,57]. Leeet al[56]recommend giving tocilizumab at a dose of 4 mg/kg over the course of one hour in adults. They also recommend repeating the dose if there are no signs of clinical improvement over 24 h to 48 h[56].
Neurotoxicity is another common adverse effect secondary to CAR T-cell therapy.According to a review by Gustet al[59], the incidence of neurotoxicity in patients undergoing CAR T-cell therapy varies between 2% to 70% of patients. The clinical syndrome of CAR T-cell induced neurotoxicity is often referred to as immune effector cell-associated neurotoxicity syndrome (ICANS)[59]. The most well known risk factors for developing ICANS are systemic cytokine release in addition to the severity of CRS[59]. Symptoms normally begin within the first 7 d following CAR T-cell infusion[59].Symptoms include cognitive impairment, tremor, headache, altered levels of consciousness, seizures, and even coma[59]. The feared complication is cerebral edema,which is often fatal[59]. Currently, there is no evidence that blockade of a single inflammatory mediator is beneficial in ICANS. Therefore, it is recommended that corticosteroids be used as first line treatment due to their ability to reduce cerebral edema as well as to induce an immunosuppressive effect that decreases the secretion of pro-inflammatory cytokines[59].
CONCLUSION
Immunotherapy, a rapidly evolving therapeutic entity, has proven to be a worthwhile addition to the arsenal of therapeutic modalities care providers have against cancers.Advancement in the field is highly dependent on a better understanding of the immune system and the advent of newer agents. However, like any other therapeutic modality, it has its own set of adverse effects and toxicities. It is essential that physicians familiarize themselves with the adverse effects and toxicities associated with these agents as their role in management of cancers continues to rise.Additionally, proper patient education on the adverse effects of these agents along with the process of joint decision making between the provider and physician will hopefully result in a decrease in unfavorable outcomes. It is also worth noting that immunotherapy is still in its infancy phase, and as newer, more specific therapies emerge secondary to a better understanding of the workings of the immune system,the ratio of benefits to risks may increase significantly.
 World Journal of Clinical Oncology2021年3期
World Journal of Clinical Oncology2021年3期
- World Journal of Clinical Oncology的其它文章
- GOECP/SEOR radiotherapy guidelines for small-cell lung cancer
- Cardiovascular risk management in cancer survivors: Are we doing it right?
- Overview of recent advances in metastatic triple negative breast cancer
- Thromboembolic events in metastatic testicular cancer treated with cisplatin-based chemotherapy