
A red herring: An unusual case of pneumothorax
2021-03-16 05:59:16JosephWallineKoonhoCheungPriscillaSongColinGraham
Joseph H. Walline, Koon-ho Cheung, Priscilla P. Song, Colin A. Graham
1 Accident and Emergency Medicine Academic Unit, Prince of Wales Hospital, the Chinese University of Hong Kong, HongKong, China
2 Department of Accident and Emergency Medicine, Prince of Wales Hospital, Hong Kong Hospital Authority, Hong Kong,China
3 Centre for the Humanities and Medicine, the University of Hong Kong, Hong Kong, China
Dear editor,
A 67-year-old Chinese man presented to our emergency department (ED) complaining of right-sided chest wall pain.He noticed these symptoms three hours prior to arrival. He denied any shortness of breath or recent injury. Past medical history was signif icant only for hypertension. Social history was signif icant for a history of smoking (40 packs per year).On examination, the patient appeared calm and in no acute distress. No central or peripheral cyanosis was seen, nor any peripheral edema. Vital signs at triage were blood pressure 148/79 mmHg (1 mmHg=0.133 kPa), heart rate 95 beats per minute, respiratory rate 16 breaths per minute, temperature 37.4 °C, and oxygen saturation (SpO2) 95% on room air. Electrocardiogram (ECG), blood count, electrolytes,troponin, and D-dimer tests were unremarkable.
Initial chest X-ray (Figure 1) showed right-sided pleural effusion, and the patient was admitted for observation. Right-sided pneumothorax (1.4 cm) was also found on the chest X-ray the next day. On further questioning, the patient mentioned that he had “choked on a f ishbone” during dinner 24 hours prior to ED arrival.A chest enhanced computed tomography (CT) with oral contrast was then performed, demonstrating a foreign body at the gastroesophageal junction (Figure 2).
The patient was treated with a therapeutic esophagogastroduodenoscopy (EGD) with successful removal of a T-shaped f ishbone from the distal esophagus and endoscopic clip repair of an 8-mm esophageal perforation.A feeding tube, a chest tube, and IV antibiotics were also provided. The patient made an uneventful recovery.
Diagnosis: right-sided hydropneumothorax secondary to foreign-body perforation of the distal esophagus.
DISCUSSION
Fish and other seafood are a major source of dietary protein in East Asia, and complaints of fish bone ingestion are quite common in EDs in this region. Fishbone ingestions generally do not result in serious injuries, although sporadic cases have appeared in the literature.[1-3]The case presented here shows how a common chief complaint of chest pain could easily be attributed to a pleural effusion or pneumothorax, but was actually secondary to ingesting a fishbone. Additionally, this case illustrates how an initial radiograph may fail to detect needle-like foreign bodies such as an ingested fishbone.[4,5]This case also demonstrates the importance of medical history taking to obtain the proper diagnosis and treatment.
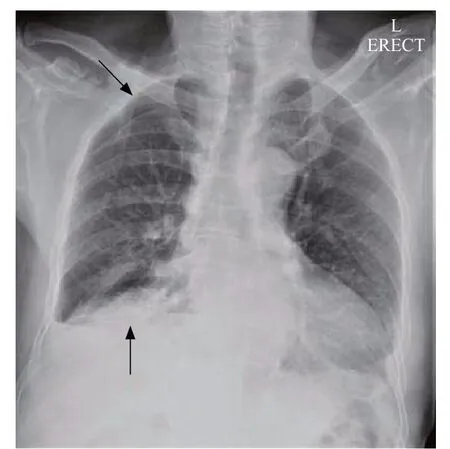
Figure 1. Initial chest radiograph demonstrating right-sided pleural effusion (lower arrow) and pneumothorax (upper arrow).

Figure 2. Images of computed tomography (CT). A: oral-contrast enhanced CT image demonstrating a foreign-body(arrow) at the gastroesophageal junction; B: non-contrast enhanced CT image demonstrating a foreign-body (arrow) at the gastroesophageal junction.
Funding:None.
Ethical approval:Not needed.
Conf licts of interests:No benef its in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Contributions:KHC and JHW collected the clinical information.PPS, CAG and JHW drafted the manuscript. All authors were involved in the final editing of the manuscript and preparation of materials for submission. The manuscript had been read and approved by all the authors, requirements for authorship had been met by each one, and each author believed that the manuscript represented honest work.
 World journal of emergency medicine2021年2期
World journal of emergency medicine2021年2期
- World journal of emergency medicine的其它文章
- World Journal of Emergency Medicine
- Overlapping public health crises during the coronavirus disease pandemic
- Comparison of intraosseous access and central venous catheterization in Chinese adult emergency patients: A prospective, multicenter, and randomized study
- Empyema associated with vegetable foreign body aspiration
- A case of a successful post-transcatheter aortic valve replacement His bundle pacing
- Detection of adrenal mass during an educational point-of-care ultrasound in the emergency department