
Diagnostic performance of narrow-band imaging international colorectal endoscopic and Japanese narrow-band imaging expert team classification systems for colorectal cancer and precancerous lesions
2021-02-06 08:06:40YunWangWenKunLiYaDanWangKuiLiangLiuJingWu
Yun Wang,Wen-Kun Li,Ya-Dan Wang,Kui-Liang Liu,Jing Wu
Yun Wang,Department of Gastroenterology,Peking University Ninth School of Clinical Medicine,Beijing 100038,China
Wen-Kun Li,Ya-Dan Wang,Department of Gastroenterology,Beijing Shijitan Hospital,Capital Medical University,Beijing 100038,China
Kui-Liang Liu,Jing Wu,Department of Gastroenterology,Beijing Friendship Hospital,Capital Medical University,National Clinical Research Center for Digestive Diseases,Beijing 100050,China
Abstract BACKGROUND In recent years,two new narrow-band imaging (NBI) classifications have been proposed:The NBI international colorectal endoscopic (NICE) classification and Japanese NBI expert team (JNET) classification.Most validation studies of the two new NBI classifications were conducted in classification setting units by experienced endoscopists,and the application of use in different centers among endoscopists with different endoscopy skills remains unknown.AIM To evaluate clinical application and possible problems of NICE and JNET classification for the differential diagnosis of colorectal cancer and precancerous lesions.METHODS Six endoscopists with varying levels of experience participated in this study.Eighty-seven consecutive patients with a total of 125 lesions were photographed during non-magnifying conventional white-light colonoscopy,non-magnifying NBI,and magnifying NBI.The three groups of endoscopic pictures of each lesion were evaluated by the six endoscopists in randomized order using the NICE and JENT classifications separately.Then we calculated the six endoscopists’sensitivity,specificity,accuracy,positive predictive value,and negative predictive value for each category of the two classifications.RESULTS The sensitivity,specificity,and accuracy of JNET classification type 1 and 3 were similar to NICE classification type 1 and 3 in both the highly experienced endoscopist (HEE) and less-experienced endoscopist (LEE) groups.The specificity of JNET classification type 1 and 3 and NICE classification type 3 in both the HEE and LEE groups was >95%,and the overall interobserver agreement was good in both groups.The sensitivity of NICE classification type 3 lesions for diagnosis of SM-d carcinoma in the HEE group was significantly superior to that in the LEE group (91.7% vs 83.3%;P=0.042).The sensitivity of JNET classification type 2B lesions for the diagnosis of high-grade dysplasia or superficial submucosal invasive carcinoma in the HEE and LEE groups was 53.8% and 51.3%,respectively.Compared with other types of JNET classification,the diagnostic ability of type 2B was the weakest.CONCLUSION The treatment strategy of the two classification type 1 and 3 lesions can be based on the results of endoscopic examination.JNET type 2B lesions need further examination.
Key Words:Narrow-band imaging international colorectal endoscopic;Japanese narrowband imaging expert team;Colorectal neoplasms;Precancerous lesions;Colorectal endoscopy;Narrow-band imaging
INTRODUCTION
Colorectal cancer (CRC) was the third most common malignancy and the second leading cause of cancer-related death globally in 2018[1].The morbidity and mortality of CRC are still rising rapidly in many low- and middle-income countries[2].The outcome and prognosis of patients with CRC are closely related to the stage of the disease.Milleret al[3]reported that the 5- and 10-year relative survival rates in CRC patients were 65% and 58%,respectively,but the 5-year relative survival rate was 90%when CRC was detected at a localized stage[3].Therefore,it is important to improve the detection rate of early stage CRC and precancerous lesions.
Colorectal endoscopy can directly observe intestinal lesions,so it is irreplaceable in the examination of intestinal disease,especially CRC.To improve the detection rate of early-stage CRC and precancerous lesions,many new assistive techniques have been used in clinical practice such as chromoendoscopy,magnifying endoscopy,fluorescence endoscopy,confocal laser endoscopy,and electronic staining endoscopy.However,the process of chromoendoscopy is complicated and time-consuming,fluorescence endoscopy and confocal laser endoscopy are expensive,and these disadvantages limit the application of these new techniques.
Compared with these new techniques,electronic staining endoscopy is more convenient and practical,and its sensitivity and specificity in distinguishing colorectal neoplastic lesions from non-neoplastic lesions are about 90% and 85%,respectively[4].Electronic staining endoscopy includes narrow-band imaging (NBI),flexile spectral imaging color enhancement,and i-scan,of which NBI is the most widely used.Since the emergence of NBI in 1999,it has been a reliable tool that has contributed to improving diagnostic accuracy,such as differentiation of neoplastic from nonneoplastic lesions and characterization of colorectal neoplasia[4,5].Through the analysis of capillary vessel structure,surface structure and lesion color under NBI,researchers have proposed a variety of classifications to judge the nature of lesions accurately and select treatment strategy appropriately.In recent years,colorectal NBI magnifying classifications such as Hiroshima,Sano,Showa and Jikei classifications have been widely used in clinical practice and play an important role clinically[6,7].However,magnifying endoscopy has not yet been widely applied outside of Japan.
The Colon Tumor NBI Interest Group put forward a new NBI classification called the NBI international colorectal endoscopic (NICE) classification in 2009[8],and validation studies of this new NBI classification were conducted in 2012[9,10].It is the first NBI classification that can be used for both non-magnifying and magnifying NBI endoscopy[8,11].The NICE classification has a high diagnostic accuracy in detecting nonneoplastic lesions that do not require resection and deep submucosal invasive (SM-d)carcinoma that needs to be treated surgically[12,13].However,it is difficult to differentiate high-grade dysplasia (HGD) or superficial submucosal invasive (SM-s)carcinoma from low-grade dysplasia (LGD)[8,14]using NICE classification.To solve this problem,the Japanese NBI expert team (JNET) composed of Japanese magnifying colonoscopists was organized in 2011,and a new NBI colorectal magnifying classification,the JNET classification was put forward in 2014[15].
To the best of our knowledge,most validation studies of the two new NBI classifications were conducted in originating centers by experienced endoscopists,but application in different centers among endoscopists with varying endoscopic skills remains unknown.To achieve external validity,in our study,we evaluated the clinical application and possible problems of NICE and JNET classifications in our unit,which is a tertiary hospital in China,and six endoscopists with varying levels of experience participated in this study.
MATERIALS AND METHODS
Patients
From September 2014 to December 2019,we enrolled consecutive patients who received white-light colonoscopy,NBI colonoscopy,and magnifying NBI colonoscopy at the same time in Beijing Shijitan Hospital (Beijing,China).Informed consent was obtained from all patients before their examinations.Patients with inflammatory bowel disease,familial adenomatous polyposis,or incomplete clinical data were excluded from this study.
Endoscopic examination
Patients drank 4 L of polyethylene glycol solution for their bowel preparation.A complete colonoscopy was performed by two experienced endoscopists,each of whom had previously performed >1000 colonoscopies annually.All examinations were performed using magnifying colonoscopy (CF-H260AZI;Olympus Optical,Tokyo,Japan) and a standard videoendoscopic system (EVIS LUCERA;Olympus Optical),and magnifying images were taken with moderate-to-high-level power zoom.When a lesion was detected,the mucus and liquid feces on the surface of the lesion were washed away with lukewarm water.Endoscopic images of each lesion were taken in the following order:Non-magnifying conventional white-light colonoscopy,nonmagnifying NBI,and magnifying NBI.The size of each lesion was estimated using the open-biopsy forceps method,with an open diameter of 7 mm (Radial Jaw 3;Boston Scientific Corp.,Natick,MA,United States).The locations of the lesions were divided into three groups (proximal colon,distal colon,and rectum).Lesions were resected by biopsy,endoscopic mucosal resection (EMR) or endoscopic submucosal dissection(ESD),and the biopsy was analyzed histopathologically.The histopathological diagnosis was based on World Health Organization criteria.
NICE and JNET classification
The NICE classification[9,10]and JNET classification[15],and typical examples of the endoscopic images used in our study are shown in Figures 1 and 2.
Interpretation of endoscopic images
Six endoscopists with varying levels of experience participated in the present study.The endoscopists were divided into two groups:A group of less-experienced endoscopists (LEE group) who had carried out colonoscopies for >5 years but not with magnifying NBI,and a group of highly experienced endoscopists (HEE group)who had routinely used magnifying NBI for >5 years[16].The three groups of endoscopic pictures of each lesion (non-magnifying white-light colonoscopy,nonmagnifying NBI,and magnifying NBI) were evaluated by the six endoscopists in a randomized order using the NICE and JENT classifications separately.The nonmagnifying white-light colonoscopy and non-magnifying NBI images demonstrated an overview of each lesion in order to mimic real-time endoscopic examination,whereas the magnifying NBI images showed crucial findings to evaluate the histopathological features.Patients information such as age,sex,clinical diagnosis,and histopathological results was not disclosed to any of the evaluators,and discussions were not permitted among the endoscopists individually or in groups.
Statistical analysis
We calculated sensitivity,specificity,accuracy,positive predictive value (PPV),and negative predictive value (NPV) for each category of the two classifications.We received histology of colorectal lesions as the gold standard.Sensitivity,specificity,accuracy,PPV,and NPV of each category of the two classifications were compared between the two groups by using the Mann-WhitneyUtest.P<0.05 was considered statistically significant.In addition,the interobserver agreement in each group was assessed using k values as follows:<0.4,poor agreement;0.41-0.60,fair agreement;0.61-0.80,good agreement;and >0.80,excellent agreement.All statistical analyses were conducted using SPSS Statistics for Windows version 22.0 (IBM Corp.,Armonk,NY,United States).The statistical methods of this study were reviewed by Qing-Kun Song from Beijing Shijitan Hospital,Capital Medical University.
RESULTS
Ninety-six patients received white-light colonoscopy,NBI colonoscopy and magnifying NBI colonoscopy at the same time between September 2014 and December 2019,and 137 lesions were resected.Nine patients with inflammatory bowel disease,familial adenomatous polyposis,or incomplete clinical data were excluded.Finally,87 consecutive patients were enrolled for endoscopic evaluation,and 125 lesions were photographed during non-magnifying conventional white-light colonoscopy,nonmagnifying NBI,and magnifying NBI.Bowel preparation was achieved perfectly and complete colonoscopy was performed to the cecum in every patient.Demographic data and characteristics of the lesions such as size,location and pathology are shown in Table 1.
Diagnostic characteristics of NICE classification
The diagnostic characteristics of each category among the two groups are shown in Table 2.The sensitivity,specificity,accuracy,PPV and NPV of type 1 lesions for the diagnosis of hyperplastic lesions (HPLs) and sessile serrated lesions (SSLs) in the HEE group were 84.6%,94.9%,93.9%,65.9%,and 98.2%,respectively,and 82.1%,93.8%,92.5%,60.4%,and 97.8%,respectively,in the LEE group.The sensitivity,specificity,accuracy,PPV and NPV of type 2 lesions for the diagnosis of adenoma in the HEE group were 91.4%,86.3%,90.7%,97.7%,and 61.2%,respectively,and 89.8%,84.3%,89.1%,97.3%,and 56.6%,respectively,in the LEE group.The sensitivity,specificity,accuracy,PPV and NPV of type 3 lesions for the diagnosis of SM-d carcinoma in the HEE group were 91.7%,97.0%,96.8%,54.0%,and 99.7%,respectively,and 83.3%,96.4%,96.0%,45.8%,and 99.4%,respectively,in the LEE group.Except for sensitivity of type 3 lesions for diagnosis of SM-d carcinoma in the HEE group was significantly superior to that in the LEE group (91.7%vs83.3%;P=0.042),the diagnostic characteristic of each category of the NICE classification was comparable,and there were no significant differences between the two groups.The overall interobserver agreement was good in both groups (κ=0.751 in HEE group,and κ=0.744 in LEE group).
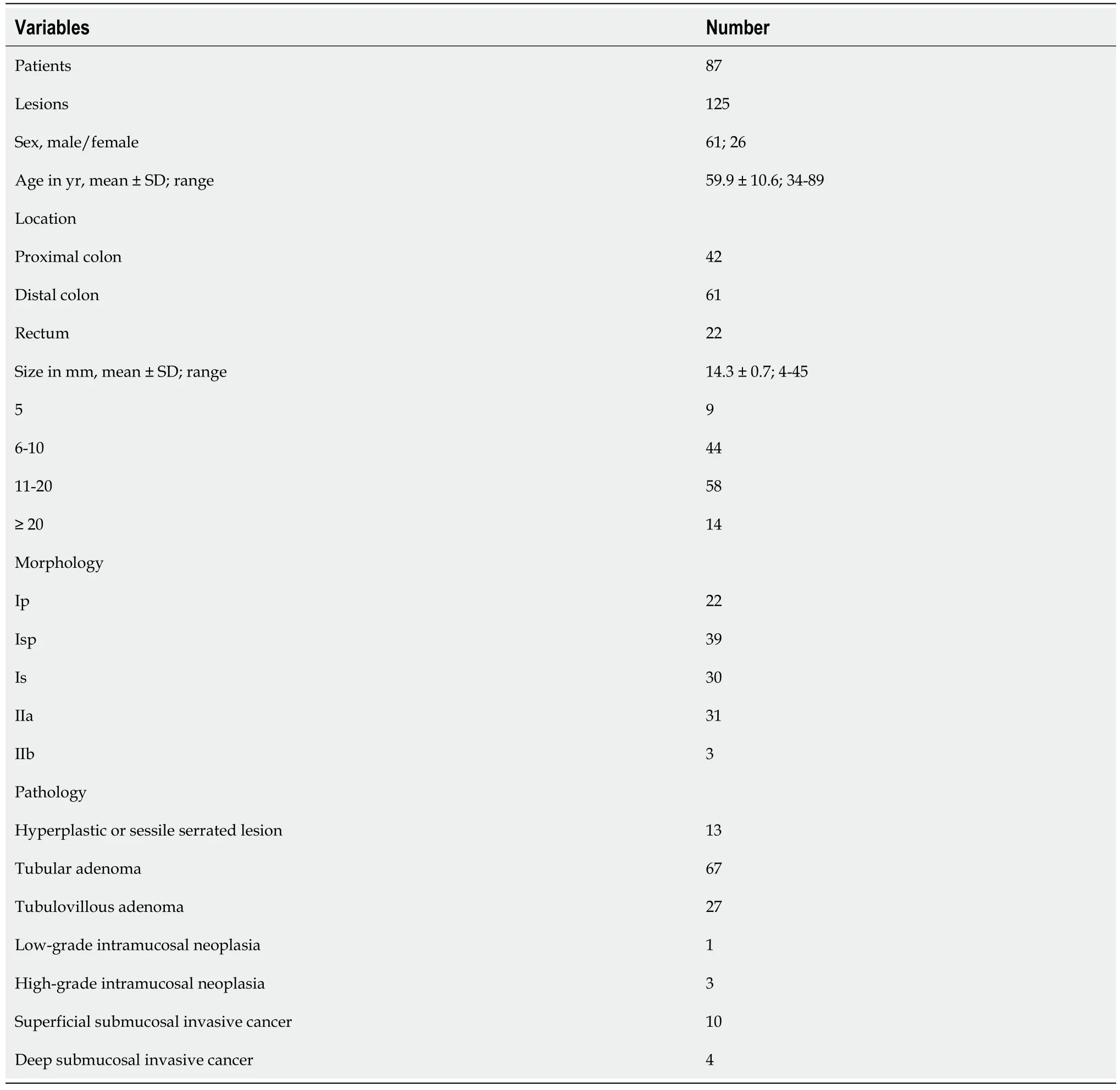
Table 1 Demographic characteristics of 87 patients with 125 colorectal lesions
Diagnostic characteristics of JNET classification
The diagnostic characteristics of each category between the two groups are shown in Table 3.The sensitivity,specificity,accuracy,PPV and NPV of type 1 lesions for the diagnosis of HPLs and SSLs in the HEE group were 87.1%,97.3%,95.5%,74.1%,and 98.5%,respectively,and 84.6%,96.4%,95.2%,73.4%,and 98.2%,respectively,in the LEE group.The sensitivity,specificity,accuracy,PPV and NPV of type 2A lesions for the diagnosis of LGD in the HEE group were 82.5%,90.0%,81.9%,93.3%,and 58.5%,respectively,and 82.5%,91.1%,84.5%,96.7%,and 62.1%,respectively,in the LEE group.The sensitivity,specificity,accuracy,PPV and NPV of type 2B lesions for the diagnosis of HGD-SM-s carcinoma in the HEE group were 53.8%,84.2%,81.4%,31.5%,and 92.2%,respectively,and 51.3%,84.8%,81.3%,28.3%,and 93.8%,respectively,in the LEE group.The sensitivity,specificity,accuracy,PPV and NPV of type 3 lesions for the diagnosis of SM-d carcinoma in the HEE group were 91.7%,98.1%,97.9%,63.2%,and 99.7%,respectively,and 83.3%,98.4%,97.9%,63.3%,and 99.4%,respectively,in the LEE group.The overall interobserver agreement was good in both groups (κ=0.747 in HEE group,κ=0.759 in LEE group).
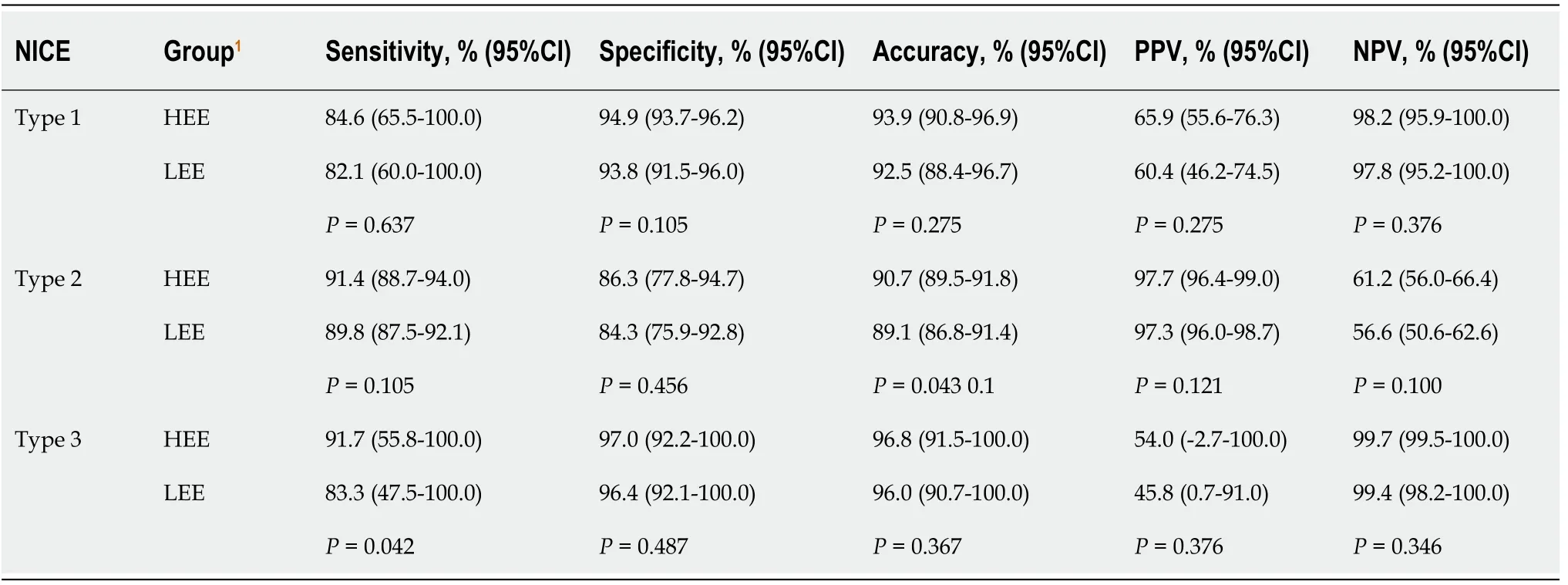
Table 2 Performance characteristics of each type of the narrow-band imaging international colorectal endoscopic classification
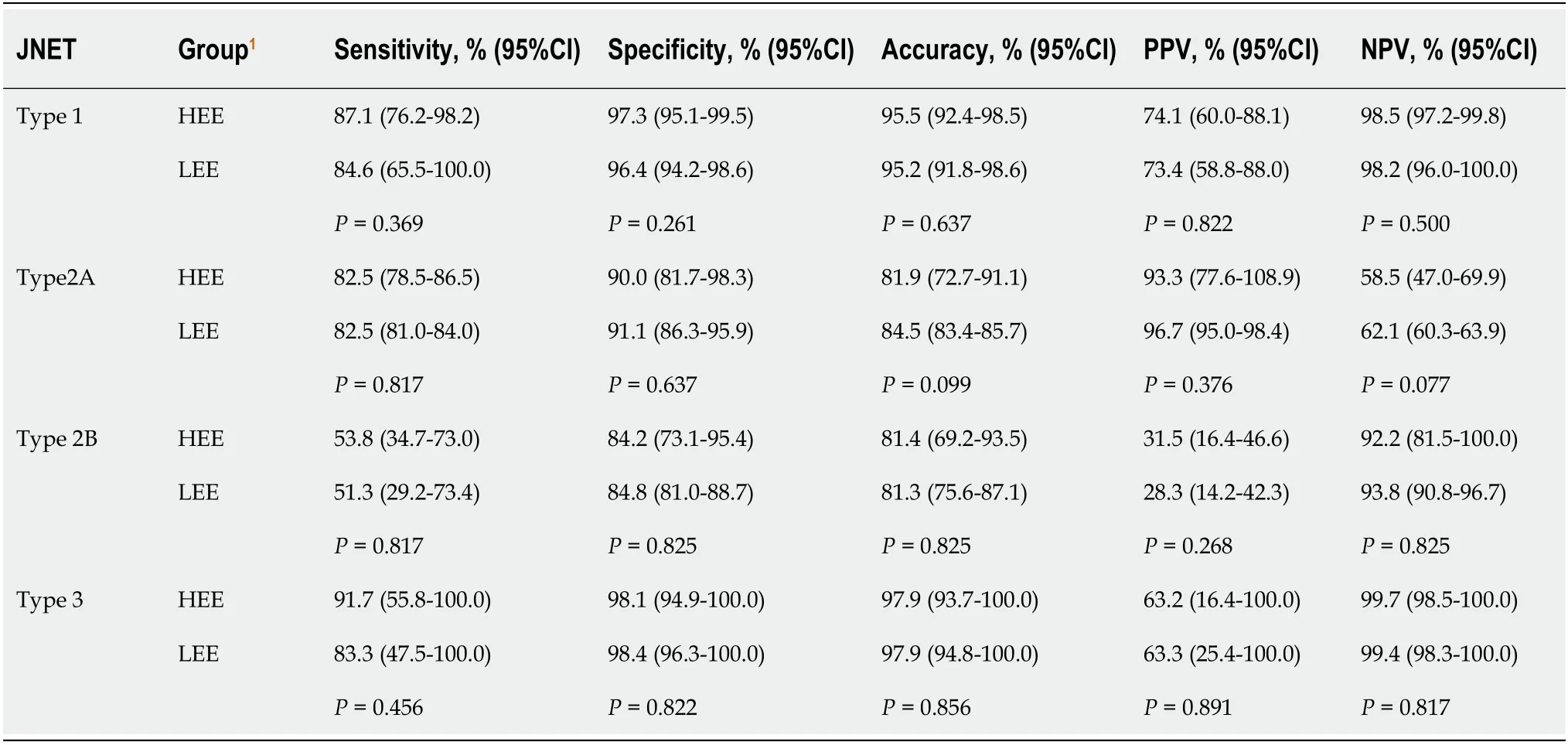
Table 3 Performance characteristics of each type of the Japanese narrow-band imaging expert team classification
DISCUSSION
Colorectal adenoma is a precancerous lesion of CRC,and its resection can reduce the incidence and mortality of CRC;therefore,in western countries,removal of all adenomatous polyps has been standardized[17,18].In clinical practice,the pathological diagnosis of all resected polyps is routinely performed,and the final pathological result determines the intervention of endoscopic follow-up[19].However,the removal of all polyps and routine pathological diagnosis not only increase the risks associated with the resection process,but also the cost of both the operation and the pathological diagnosis.Therefore,the resect and discard policy has been proposed[20-22].The policy states that the HPL do not need treatment,and the treatment of these lesions may increase the adverse events of polypectomy and cost of medical care[19,23-25].As reported previously,the NICE classification is simple and practical in identifying HLP that should be left[8,26].In our study,the sensitivity,specificity and accuracy of NICE classification type 1 lesions for the diagnosis of HPLs and SSLs in both the HEE and LEE groups were >80%,with specificity and accuracy >90%,with no significant difference between the two groups.This result shows that endoscopists can choose the treatment plan based on the NICE classification,which may improve the resect and discard strategy better promote.
The HEE group still had high specificity and accuracy >95% when using NICE type 3 to diagnose SM-d carcinoma,and the sensitivity was 91.7%,but in the LEE group the sensitivity was only 83.3%.ThePvalue of the sensitivity between the two groups was 0.042 by the Mann-WhitneyUtest,and the difference between the two groups for diagnosis of SM-d carcinoma was significant.Hayashiet al[10]found that the sensitivity of NICE type 3 for the diagnosis of SM-d carcinoma was 94.9%[10].Compared with the study above,the sensitivity of the LEE group in the diagnosis of SM-d carcinoma was still low.This result may be related to the lack of experience in the diagnosis of SM-d carcinoma in the LEE group.Therefore,endoscopists in the LEE group should receive more training to avoid missed diagnosis of SM-d carcinoma.
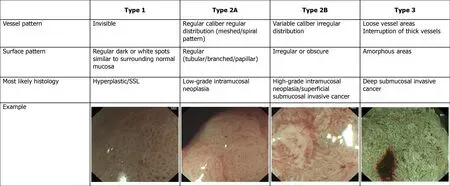
Figure 2 Japanese Narrow-band Imaging Expert Team classification.
To obtain a precise histological diagnosis,HGD or SM-s carcinoma should be resected byen blocEMR/ESD or surgery rather than piecemeal EMR (pEMR).However,in clinical practice,we cannot determine the strategy of endoscopic treatment,such as pEMR,en blocEMR/ESD or surgery,because NICE type 2 is difficult to differentiate HGD or SM-s carcinoma from LGD[8,14].To solve this problem and unify the current NBI classifications,the JNET classification with magnification was proposed[15].The principles and characteristics of the JNET classification are as follows:Mmagnification is essential and the basis is the NICE classification;NICE type 2 is divided into 2A and 2B subtypes using magnifying findings;Because magnification does not need estimation of color,the classification does not include the finding of color;and basic findings are composed of both vessel and surface patterns[27].
Our results suggested that the sensitivity,specificity and accuracy of JNET classification types 1 and 3 were similar to NICE classification types 1 and 3 in both the HEE and LEE groups,and the specificity of JNET classification types 1 and 3 and NICE classification type 3 in both the HEE and LEE groups was >95%.The sensitivity,specificity,accuracy,PPV and NPV of JNET classification type 2A lesions for the diagnosis of LGD in the HEE group were 82.5%,90.0%,81.9%,93.3%,and 58.5%,respectively,and 82.5%,91.1%,84.5%,96.7%,and 62.1%,respectively,in the LEE group.The results are similar to those of Sumimotoet al[27].In order to avoid missed diagnosis of lesions,the sensitivity of the classification is important.However,before treatment of the lesion,the specificity of the classification is more important,because only by accurately determining the nature of the lesion can the appropriate treatment strategy be selected.In our study,the specificity of NICE types 1 and 3 and JNET types 1,2A and 3 in both the HEE and LEE groups was >90%.So,when the endoscopist’s diagnostic confidence level is high (>95%)[27],the treatment strategy for NICE types 1 and 3 and JNET types 1,2A and 3 lesions can be determined based on the results of endoscopic examination.Of course,if the confidence level is low,an additional examination should be performed.
The JNET type 2B lesions are the most important for curation and the most difficult to be diagnosed endoscopically.In our study,the sensitivity of JNET classification type 2B lesions for the diagnosis of HGD-SM-s carcinoma in the HEE group was 53.8% and 51.3% in the LEE group.As our result,even in the HEE group the sensitivity was not more than 60%.Previous studies showed that the sensitivity of JNET classification Type 2B lesions for diagnosis of HGD-SM-s carcinoma was 44.9%-61.9%[27,28].Compared with other types of JNET classification,the diagnostic ability of type 2B is the weakest.Although Sumimotoet al[29]further divided JNET type 2B into 2B-low and 2B-high[29],the ability to diagnose HGD-SM-s carcinoma has not been significantly improved.The original intention of the JNET classification introduce the type 2A and 2B lesion was to distinguish LGD and SM-d carcinoma from HGD-SM-s carcinoma,and then to choose an appropriate treatment strategy,such as pEMR,en blocEMR/ESD or surgery.However,due to poor diagnostic capabilities of type 2B,this goal cannot be achieved,and the type 2B lesions is still the biggest challenge for the endoscopists.So,lesions of type 2B need a further pit pattern diagnosis using magnifying chromoendoscopy or endoscopic ultrasound[29-31].
Our study had some limitations.First,although six endoscopists with varying levels of experience participated in the study,they all belonged to the same institution and would be following similar guidelines,which may produce high interobserver agreement and threaten the external validity of the results.These results might be different when endoscopists belong to different units.Second,we initially presented non-magnifying conventional white-light overview images of entire lesion in order to mimic real-time endoscopic examination.For some endoscopists,the first observation of an entire lesion may affect their diagnosis of the lesion,especially when evaluating the lesion using the JNET classification.It is necessary for us to conduct a further study where we evaluate JNET classification using only magnifying NBI images of the lesions.Third,as a retrospective study,we enrolled as many cases as possible.However,in clinical practice,most SM-d carcinoma can be correctly diagnosed under white-light colonoscopy without further magnifying examination,so there were only four cases of deep-submucosal invasive cancer.The diagnostic accuracy and reliability of NICE and JNET classifications should be validated in a multicenter prospective study.
CONCLUSION
In conclusion,NICE types 1 and 3 and JNET types 1,2A and 3 lesions showed excellent diagnostic ability in both the HEE and LEE groups.When the confidence level is high,the treatment strategy of the NICE types 1 and 3 and JNET types 1,2A and 3 lesions can be determined based on the results of endoscopic examination.JNET type 2B lesions require extra examination,such as magnifying chromoendoscopy or endoscopic ultrasound,to make an accurate assessment of the invasion depth for selecting an appropriate treatment strategy.
ARTICLE HIGHLIGHTS
Research background
Detecting and treating early stage colorectal cancer (CRC) and precancerous lesions is the most effective method to reduce the morbidity and mortality of CRC.Narrowband imaging (NBI) endoscopy has been a very useful technique that has contributed to improving the detection rate of early stage CRC and precancerous lesions.Researchers have proposed a variety of NBI classifications to judge the nature of lesions accurately and select treatment strategy appropriately.
Research motivation
For the past few years,two new NBI classifications have been proposed:The NBI international colorectal endoscopic (NICE) classification and Japanese NBI expert team(JNET) classification.Most validation studies of the two new NBI classifications were conducted in originating centers by experienced endoscopists,but application in different centers among endoscopists with varying endoscopic skills remains unknown.
Research objectives
To achieve external validity,we evaluated the clinical application and possible problems of the NICE and JNET classifications for differential diagnosis of colorectal cancer and precancerous lesions.
Research methods
Six endoscopists with varying levels of experience were divided into two groups:Highly experienced endoscopists (HEEs) and less-experienced endoscopists (LEE).Eighty-seven consecutive patients with a total of 125 lesions were photographed during non-magnifying conventional white-light colonoscopy,non-magnifying NBI,and magnifying NBI.The three groups of endoscopic pictures of each lesion were evaluated by the six endoscopists in a randomized order using the NICE and JENT classifications separately.We calculated sensitivity,specificity,accuracy,positive and negative predictive value for each category of the two classifications.
Research results
In both the HEE and LEE groups,the specificity of JNET classification type 1 and 3 and NICE classification type 3 was >95%,and the overall interobserver agreement was good in both groups.However,the sensitivity of JNET classification type 2B lesions for the diagnosis of high-grade dysplasia or superficial submucosal invasive carcinoma in both the HEE and LEE groups was <55%.Compared with other types of NICE and JNET classification,the diagnostic ability of JNET type 2B was the weakest.
Research conclusions
Due to the poor diagnostic capabilities of JNET type 2B,the type 2B lesions is still the biggest challenge for the endoscopists.So,lesions of type 2B need an additional examination to choose an appropriate treatment strategy.
Research perspectives
The JNET type 2B lesions are the most important for curation and the most difficult to be diagnosed endoscopically,and accurate diagnosis of JNET 2B lesions still requires further efforts.
 World Journal of Gastrointestinal Oncology2021年1期
World Journal of Gastrointestinal Oncology2021年1期
- World Journal of Gastrointestinal Oncology的其它文章
- Internal hemorrhoid harboring adenocarcinoma:A case report
- Efficacy and safety of intraoperative radiotherapy in rectal cancer:A systematic review and meta-analysis
- Mining The Cancer Genome Atlas database for tumor mutation burden and its clinical implications in gastric cancer
- Survival outcomes and prognostic indicators for gastric cancer patients with positive peritoneal wash cytology but no peritoneal metastasis after radical gastrectomy
- Laparoscopy-assisted transanal total mesorectal excision for lower rectal cancer:A feasible and innovative technique
- Myeloid-derived suppressor cells in gastrointestinal cancers:A systemic review