
Intracranial Abnormalities of Infantile Hemangiomas in the Head and Neck Regions:A Retrospective MRI Study
2021-01-09 05:45YingGaoandXiaoLiYi
国际皮肤性病学杂志 2020年4期
Ying Gao and Xiao-Li Yi
1Department of Dermatology; 2Department of Radiology, Capital Institute of Pediatrics, Beijing 100020, China.
Abstract
Keywords: infantile hemangiomas, magnetic resonance imaging, intracranial abnormalities
Introduction
A cutaneous hemangioma is the most common benign vascular tumor of infancy.1Approximately 60% of infantile hemangiomas are located in the head and neck.2Most infantile hemangiomas are uncomplicated and do not require treatment.However,early intervention may be necessary for hemangiomas in high-risk anatomic sites(such as intracranial) with a risk of complications.3
Most intracranial abnormalities described in previous studies included symptoms such as an increased head circumference, cranial nerve palsy, decreased rectal tone,and areflexia,mostly in association with PHACE(Posterior fossa malformations,facial Hemangiomas,Arterial anomalies,Cardiac defects,and Eye abnormalities)syndrome.4-6Few studies to date have reported the imaging findings of intracranial abnormalities in infants with hemangiomas.Viswanathan et al6reported the imaging findings of hemangioma involvement of the central nervous system in a retrospective study. In addition, Friedland et al7observed 1 patient with a small asymptomatic hemangioma on brain magnetic resonance imaging(MRI)in infants with multifocal cutaneous hemangiomas. However, the abovementioned study only reported the imaging findings of intracranial hemangioma in infants with hemangioma.There is lack of relatively systematic reports about the imaging findings of intracranial abnormalities including brain structure, cerebrovascular, and other anomaly.Considering that early intervention to prevent potential complications arising from intracranial abnormalities is critical for improvement of the patients’quality of life,it is important to describe the imaging characteristics and associations of these intracranial abnormalities.
Moreover, infantile hemangiomas are classified into three morphological subtypes: focal, segmental, and multifocal lesions, and the subtype is a major factor that predicts complications and/or the need for treatment.8-9In a prospective cohort study of 1,058 children,children with segmental hemangiomas were 11 times more likely to develop complications and eight times more likely to receive treatment than patients with focal hemangiomas.3However, there has been no report on the incidence of intracranial abnormalities in different subtypes of infantile hemangioma by now.
We performed the present retrospective MRI study firstly to describe the intracranial abnormalities of infants with hemangiomas in the head and neck,secondly to assess the relationship between intracranial abnormalities and the subtypes of infantile hemangiomas, and thirdly to discuss the need for MRI performed in different subtypes of infantile hemangiomas,which may be helpful to reduce medical costs of patients.
根据项目技术方案,该项目实施地点为丘北县双龙营镇麻栗树村,该村交通便利、水资源丰富,稻田平整集中,年平均气温为18-20℃,年均降雨量900-1200毫米,主要居住着汉族和彝族。通过土地集中流转到合作社统一实施,项目实施面积为120亩。
Materials and methods
We performed a retrospective review of the hemangioma treatment center database at the Capital Institute of Pediatrics for sick children aged <12 months who had been clinically diagnosed as infantile hemangiomas based on their clinical and imaging characteristics from January 1,2010 to July 1,2018.Children with infantile hemangiomas in the head and neck who underwent their first brain MRI examination before initiating therapy were included in the study.The information of patients’demographics(age,sex,andgestationalage),ageatdiagnosis,clinicalfeatures,brain MRI findings, and subsequent medical follow-up were collected and analyzed.Institutional review board approval was obtained from the Capital Institute of Pediatrics for this retrospective chart review (No.KSSHERLL 2017012).
All patients were scanned using a 1.5-Tesla Signa HDx MRI system(GE Healthcare,Chicago,IL,USA).Standard sequences included pre- and post-contrast T1- and T2-weighted imaging,fluid-attenuated inversion recovery,and diffusion-weighted imaging.All images were independently reviewed by two board-certified pediatric radiologists.The key assessment parameter was whether intracranial abnormalities were present.For intracranial lesions,the T1-and T2-weightedimagingcharacteristics,morphology,extentof contrast enhancement,continuity with extracranial hemangiomas, and important associated brain anomalies were assessed.Data are presented as frequency with percentage,mean± standard deviation,or median(range).
Statistical analysis
The Kappa test was used to assess the difference between the two radiologists who evaluated the images. Statistical analyses were carried out using SPSS version 22.0 (IBM Corp., Armonk, NY, USA).
Results
Baseline of the patients with hemangiomas in the head and neck regions
A total of 436 patients with infantile hemangiomas were included,consisted of 258 females and 178 males(female:male ratio 1.45:1),with a mean age of 1.9 months(range 1-12) at their first visit to the clinic. Three hundred and fifty-four were born term, and 82 (19%) were born prematurely(<37 weeks).In this cohort,most hemangiomas were classified as focal infantile hemangiomas(342, 79%), whereas 88 (20%) were segmental and 6 (1%) were multifocal.
Clinical features
Abnormal brain MRI findings were reported in 23(5%)of 436 patients; three patients had focal infantile hemangiomas, and 20 had segmental infantile hemangiomas. Most patients presented with cutaneous tumors within the first few months of life (Table 1). The photographs of 20 patients with segmental infantile hemangiomas showed involvement of the frontotemporal region in 14 (70%),frontonasal region in 8 (40%), maxillary region in 4(20%),and mandibular region in 2(10%).The hemangioma involved only one region in 14 (70%) of the 20 patients, and the other six patients had involvement of multiple regions. The lesions developed on the scalp in eight (40%) patients. Eighteen (90%) patients had unilateral hemangiomas. In addition, one patient had a subcutaneous lesion on the left side of the neck(Fig.1A).Four patients had orbital hemangiomas.Two patients had coarctation of the aorta,and one had a sternal cleft.Of the 23 patients with intracranial abnormalities, two patients with a unilateral cerebellopontine angle(CPA)hemangioma exhibited ipsilateral facial paresis,and one patient with bilateral CPA hemangiomas presented with hearing loss at birth; the remaining 20 patients had no abnormal neurological signs or symptoms. In the patient with bilateral CPA hemangiomas, partial hearing was restored 2 months after oral propranolol treatment.
Brain MRI findings
The abnormal brain MRI findings are detailed in Table 1.The most common abnormal brain MRI finding was an intracranial hemangioma, which was identified in 14(61%) of the 23 patients. The evaluation of intracranial hemangiomas showed good agreement between the two radiologists (Kappa=0.822, P<0.001). In all cases, the intracranial hemangiomatous components had the same imaging findings as the extracranial appearance (ie,homogeneous enhancement). Intracranial hemangiomas were located within the ventricle and cisterns or were ipsilateral lesions that involved the extradural space.Eight patients had enhancing hemangiomas in the cisterns,including the CPA and pericerebellar cisterns(Fig.1A and 1B). One patient had enhancing hemangiomas involving the cavernous sinus and adjacent extradural space. Five patients had enhancing hemangiomas within the lateral or fourth ventricle (Fig. 1C).
Eight patients had intracranial structural abnormalities,including six with hypoplasia of the cerebellar hemisphere ipsilateral to the hemangioma and two with Dandy-Walker malformation and hydrocephalus (Fig. 2A). Fivepatients had intracranial arterial anomalies, including two with a hypoplastic and two with an aplastic ipsilateral internal carotid artery,which were seen on brain magnetic resonance angiography (Fig. 2B); the ipsilateral posterior cerebral artery was absent in one patient. In addition, a vein of Galen aneurysm was noted in one patient.Arteriovenous malformations were found in three patients,located in the cavernous sinus, occipital lobe, and cerebellum, respectively. A hypothalamic hamartoma was found in one patient.
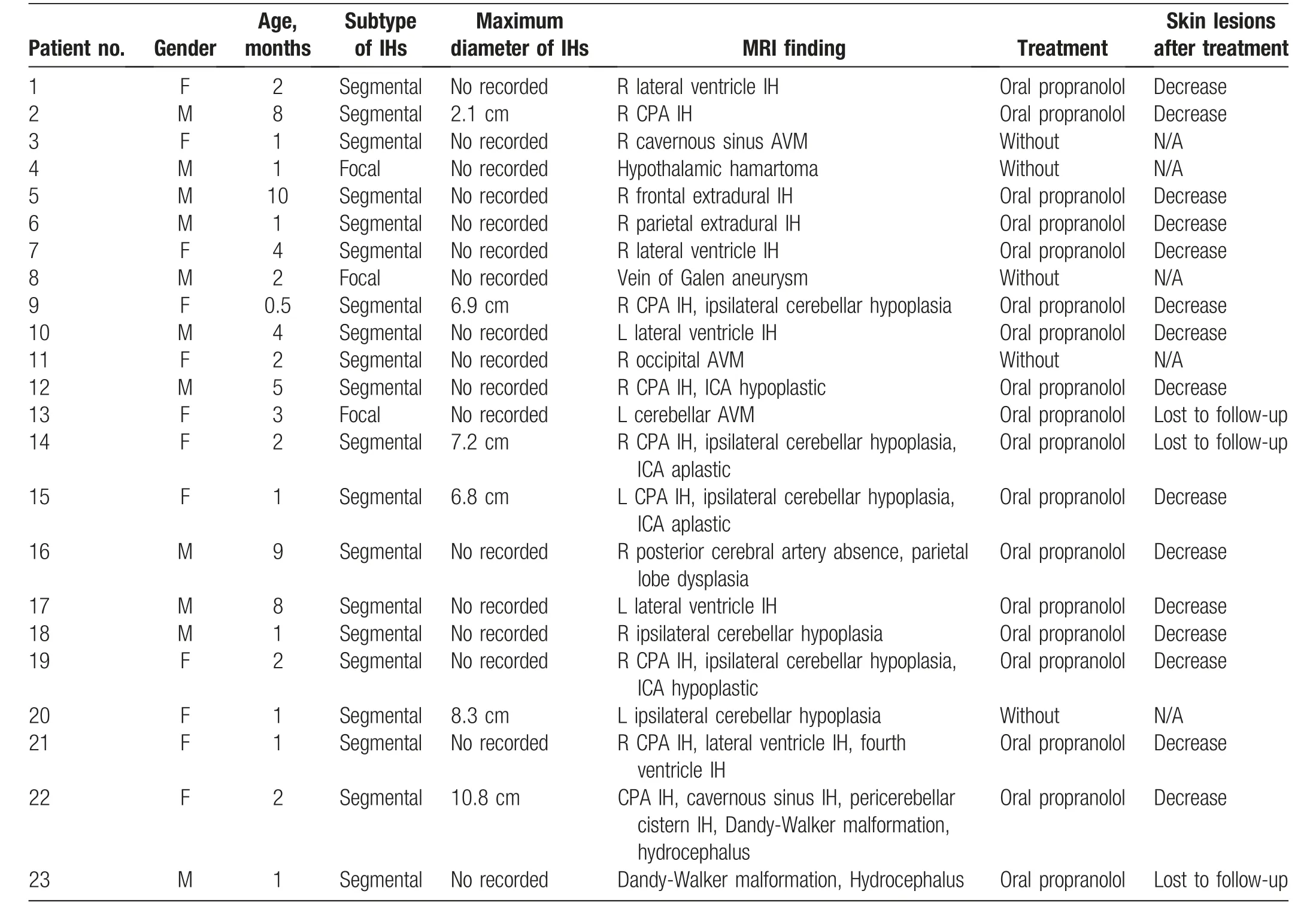
Table 1 Brain MRI findings and management of patients with intracranial abnormalities.
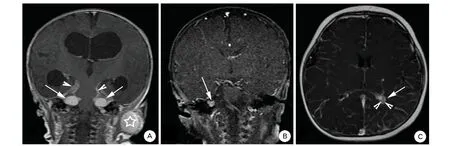
Figure 1. Skin hemangioma together with typical magnetic resonance imaging findings of intracranial hemangiomas. A: Coronal T1 postcontrast image from a two-month-old girl with bilateral cerebellopontine angle (CPA) hemangiomas shows two well-circumscribed, intensely enhancing masses in the bilateral CPA cistern(arrow)invading the adjacent dura(arrowhead).A subcutaneous hemangioma is noted on the left side of the neck(asterisks).The ventricles are markedly enlarged.B:Coronal T1 post-contrast image from a five-month-old boy with a right CPA hemangioma shows the enhancing right CPA mass (arrow). C: Axial T1 post-contrast image from a four-month-old boy with a left facial segmental hemangioma shows an intensely enhancing mass in the trigone of the left lateral ventricle(arrow)with a small number of flow voids(arrowhead), consistent with a hemangioma.
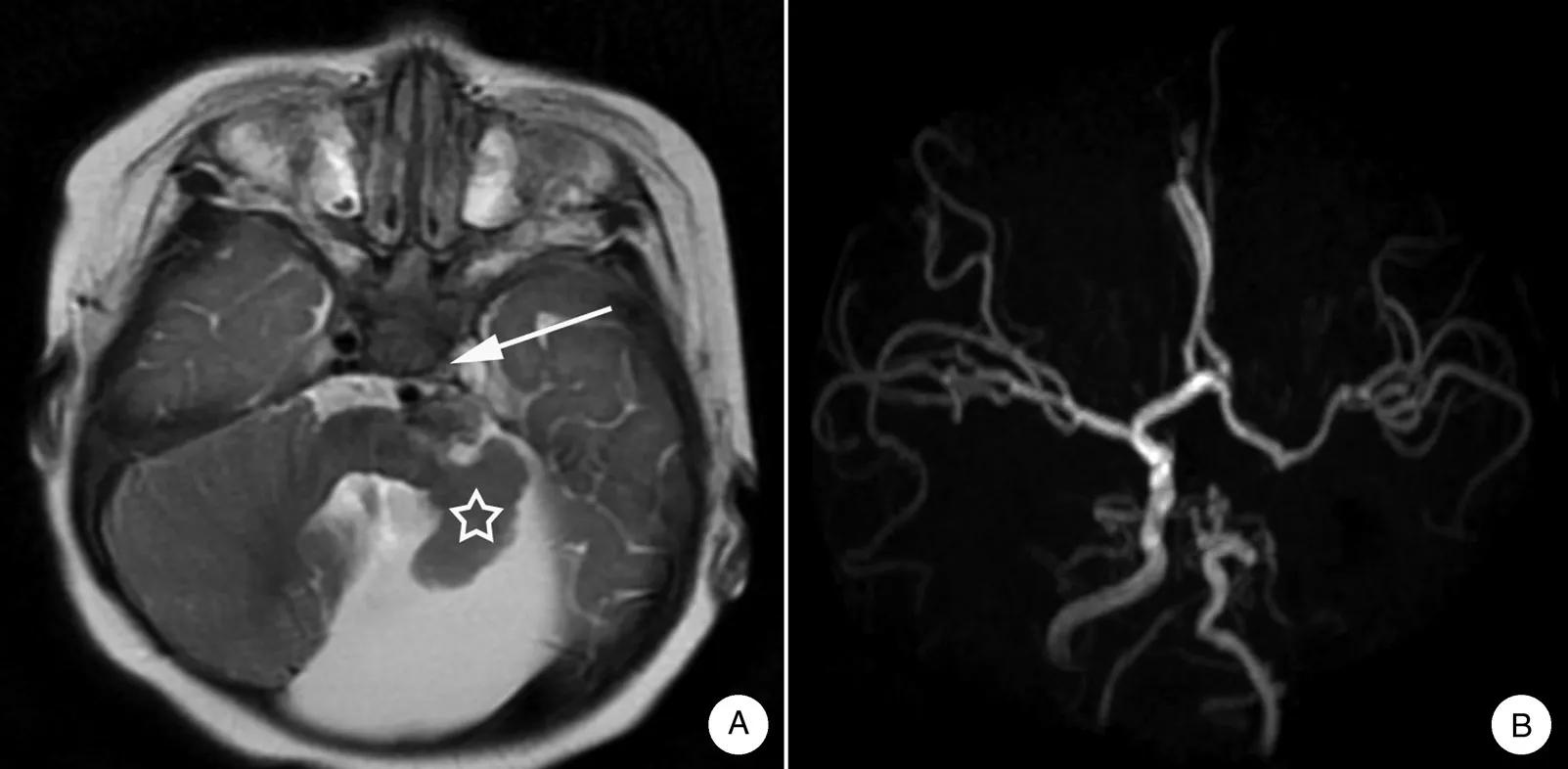
Figure 2. Magnetic resonance imaging and angiography results of abnormal intracranial structures from infants with intracranial hemangiomas.A:Axial T2 image shows no sign of flow void in the left internal carotid artery(arrow).Note the left cerebellar dysplasia(asterisks).B:Magnetic resonance angiography confirmed left internal carotid artery aplasia.
Discussion
To the best of our knowledge,the present study reviewed the largest number of cases with intracranial hemangiomas to date. Considering the racial differences in the clinical characteristics of infantile hemangiomas,10our data are the first to demonstrate the prevalence of intracranial abnormalities with imaging findings in Chinese infants.
The incidence of intracranial hemangiomas and associated anomalies was 61% among the infants with hemangiomas in the present study, which is in disagreement with the previous study showing a extremely low incidence of intracranial abnormalities at <1%.6An important reason for the higher incidence is due at least in part to the referral nature of our practice; therefore, our findings are not necessarily representative of all infantile hemangiomas.
This report provides the first description of the incidence of intracranial involvement and associated anomalies in different morphological subtypes of infantile hemangiomas.The incidence of intracranial abnormalities in infants with segmental infantile hemangiomas was relatively high.Intracranial hemangiomas are believed to be more commonly associated with segmental hemangiomas.However, whether this is a bias remains unclear because patients with large segmental hemangiomas undergo brain imaging, whereas patients with focal facial hemangiomas or multiple hemangiomas generally do not. Our study provides support for the hypothesis that intracranial hemangiomas are indeed much more commonly associated with segmental hemangiomas. Moreover, our patients showed that hemangiomas in the frontotemporal and frontonasal regions are associated with a higher risk of central nervous system involvement. Extracutaneous manifestations may reportedly arise in association with segmental infantile hemangiomas involving other anatomic sites and in conjunction with structural heart disease and central nervous system or eye anomalies.11A previous study showed that segmental hemangiomas occurred in infants born at a later gestational age with higher birth weight than other types of hemangiomas.This finding is in conflict with the known association between hemangiomas and prematurity, again raising the possibility that developmental differences may exist between segmental and other types of hemangiomas.10In the three patients with focal hemangiomas, the brain MRI findings of the intracranial lesions may not have been related to the infantile hemangiomas. Further research is warranted to confirm these results.
In the present case series,the most common intracranial abnormality was hemangiomas.These are extremely rare,and only 36 cases have been reported to date.12Most documented intracranial hemangiomas were located in the CPA or internal auditory canal.6,13-16Other sites of predilection include the ventricle, pineal region, hippocampus, and along the cerebellar convexity.13-14The intracranial hemangiomas in our patients were located in the CPA,pericerebellar cistern,lateral or fourth ventricle,and extradural space, which is consistent with the aforementioned reports. We documented head and neck cutaneous hemangiomas in 14 patients with intracranial hemangiomas, representing approximately 3% of all patients. In our center, brain MRI is routinely performed for patients with head and neck hemangiomas;therefore,it is not surprising that we found a higher rate of intracranial hemangiomas than in other studies.6Intracranial hemangiomas often occur in association with PHACES syndrome.5-6,13Six(43%)of the 14 patients with intracranial hemangiomas met the diagnostic criteria for PHACES syndrome in this study,17which is lower than previously reported.5-6,13Because magnetic resonance angiography and cardiac screening were not routinely performed in this study, it is highly likely that patients with cardiovascular and cerebrovascular anomalies were missed.
The second most common brain MRI manifestation is brain anomalies,especially posterior fossa anomalies.In our cohort,eight of the 88 patients with segmental lesions had ipsilateral cerebellar hypoplasia and Dandy-Walker malformation, whereas none of the 348 patients with non-segmental lesions had brain anomalies. Four patients also had ipsilateral internal carotid artery dysplasia. These eight patients were considered to have fulfilled the diagnostic criteria for PHACES syndrome.17One study suggested that 2% of children with facial hemangiomas and 20%of children with segmental facial hemangiomas may have PHACES syndrome.5In the present study,PHACES syndrome was identified in eight patients,all of whom had segmental hemangiomas.This high incidence of brain anomalies in patients with segmental infantile hemangiomas differs from the findings reported by Li et al.,18suggesting that the morphological subtype is not the major predictor of complications in Chinese patients with hemangiomas.It is possible that brain MRI was not routinely performed in their institution,making it highly likely that patients with brain anomalies were missed.
Three infants in this study presumably had intracranial arteriovenous malformations. To our knowledge, eight cases of segmental hemangiomas occurring in association with arteriovenous malformations have been reported to date,19and six of these eight patients met the diagnostic criteria for PHACES syndrome.18However, none of the three patients met the diagnostic criteria for the PHACES syndrome in the present study. A hypothalamic hamartoma and vein of Galen aneurysm, not previously described in reports of infantile hemangioma, were seen in one patient each. Whether these are rare features of patients with hemangiomas or if their occurrence was merely a coincidence remains unclear.
Our retrospective study had several limitations. First,tertiary hospital-based cases may not represent the incidence of intracranial abnormalities occurring in all infants with head and neck hemangiomas. These results should; therefore, be interpreted with caution. Second,although the size of cutaneous infantile hemangiomas is clinically important information,this was not recorded in all patients. However, the photographs in the medical records showed that the lesion covered the around onefifth of the facial area in patients with intracranial abnormalities. Third, the small sample size was a limitation in performing the statistical analysis. In future studies, the sensitivity and specificity of brain MRI as a screening test for intracranial abnormalities should be clarified because it might affect the clinician’s decision to recommend screening for infants with head and neck hemangiomas or to institute treatment.
In conclusion,this study confirmed that the morphological subtype of an infantile hemangioma is a factor that influences the occurrence of intracranial abnormalities.This study supports the hypothesis that intracranial hemangiomas are indeed much more commonly associated with segmental hemangiomas. The incidence of intracranial abnormalities,including hemangiomas and structural brain and/or arterial anomalies,is not low in infants with segmental head and neck hemangiomas.
Source of funding
The present study was supported by the Research Foundation of Capital Institute of Pediatrics (No. PY-2018-10)and the National Natural Science Foundation of China (No. 81703106).
猜你喜欢
烟台果树(2022年3期)2022-11-26
现代装饰(2021年6期)2021-12-31
中国土壤与肥料(2020年6期)2021-01-18
新农民(2019年2期)2019-08-16
农家科技下旬刊(2017年12期)2018-04-16
现代农业科技(2018年22期)2018-01-15
农家科技下旬刊(2017年9期)2017-11-12
中国核电(2017年2期)2017-08-11
大自然探索(2015年9期)2015-03-16
诗潮(2014年10期)2014-11-17

- 国际皮肤性病学杂志的其它文章
- Kidney Stones Are Prevalent in Individuals with Pseudoxanthoma Elasticum, a Genetic Ectopic Mineralization Disorder
- Adverse Skin Reactions to Personal Protective Equipment Among Health-Care Workers During COVID-19 Pandemic: A Multicenter Crosssectional Study in Indonesia
- Complete Draft Genome Sequence of Cutibacterium (Propionibacterium) acnes Type Strain ATCC6919
- The Immune Function of Keratinocytes in Anti-Pathogen Infection in the Skin
- A Case Report of Pemphigoid Nodularis as Masquerader of Neurotic Excoriations
- Co-occurrence of Vitiligo and Psoriasis in an 11-Year-Old Girl: A Case Report