
Intraoperative thromboelastography as a tool to predict postoperative thrombosis during liver transplantation
2020-12-25 07:27LesleyDePietriRobertoMontaltiGiulianoBolondiValentinaSerraFabrizioDiBenedetto
World Journal of Transplantation 2020年11期
Lesley De Pietri,Roberto Montalti, Giuliano Bolondi, Valentina Serra, Fabrizio Di Benedetto
Lesley De Pietri, Department of General Surgery, Division of Anaesthesiology and Intensive Care Unit, Nuovo Ospedale Civile di Sassuolo, Sassuolo 41049, Modena, Italy
Roberto Montalti, Department of Public Health, Hepato-Pancreato-Biliary Surgery Section, Federico II University of Naples, Napoli 80138, Italy
Giuliano Bolondi, Surgery and Trauma Department, Intensive Care Unit, Ospedale Bufalini Cesena, Cesena 47521, Italy
Valentina Serra, Fabrizio Di Benedetto, Surgery Department, Hepato-Pancreato-Biliary Surgery, Surgical Oncology and Liver Transplantation Unit, Azienda Ospedaliero Universitaria di Modena, University of Modena and Reggio Emilia, Modena 41125, Italy
Abstract
Key Words: Thromboelastography; Hepatic artery thrombosis; Portal vein thrombosis; Liver transplantation; Risk factors; Cirrhosis
INTRODUCTION
In recent years, patient survival after liver transplantation (LT) has increased due to improvements in surgical and anesthetic procedures. However, thromboembolic complications (hepatic artery and portal vein thrombosis, pulmonary embolism, intracardiac thrombosis) still affect the perioperative period of LT, representing relatively frequent causes of increased mortality. The percentage increase in mortality varies between 45% and 68% for pulmonary embolism, 50% for early hepatic artery thrombosis (HAT) and between 32% and 60% for portal vein thrombosis (PVT)[1-3].
Several causes of thrombosis have been recognized in LT: Surgical causes (difficult and prolonged arterial reconstruction, kinking of the artery for HAT, preceding PVT or splenectomy, small size of the portal vein), the donor’s characteristics, and prolonged cold ischemia time (CIT) and warm ischemia time (WIT)[4]. Moreover, intrinsic factors such as the patient’s genetics and underlying disease, hemodynamic modifications and intraoperative transfusions are other important causal effects.
Less attention has been paid to modification of the recipient's coagulation profile during LT[5]. The traditional concept of cirrhosis as a hypocoagulable condition has been replaced by the new idea of rebalanced hemostasis obtained by a parallel decline in pro and antihemostatic drivers[6,7]. This precarious balance can readily tip toward either hemorrhage or a prothrombotic state during LT, both for endogenous and exogenous factors. During this surgical procedure, von Willebrand factor (vWF) levels remain elevated increasing its functional capacity during surgery[8]. At the same time, the plasmatic concentration of ADMTS13 cleaving protease decreases, modifying the normal ratio of vWF/ADMATS13 in favor of vWF, possibly increasing the thrombotic risk. Abnormally increased levels of factor VIII, due to decreased degradation and reduced protein C, have also been observed[9,10].
During the anhepatic phase and after reperfusion of the liver graft, a temporary hyperfibrinolysis, attributed to changes in t-PA, PAI, and TAFI activity, can develop, but it usually corrects spontaneously as the liver graft begins to function[10,11]. However, a huge increment in plasminogen activator inhibitor type 1 (PAI-1) develops at the end of the surgery, causing a hypofibrinolytic condition usually lasting up to 5 d after the surgical procedure[12].
Traditional coagulation tests, such as prothrombin time/international normalized ratio, activated partial thromboplastin time, fibrinogen, and platelet count have several limitations in recognizing significant coagulopathies or prothrombotic conditions. In contrast, viscoelastic tests such as thromboelastography (TEG) and thromboelastometry (ROTEM) have been shown to be ideal tests for rapid diagnosis of coagulation balance, offering physicians better indicators for the clinical management of liver transplant patients[10,12]. They provide visual information on the coagulation process, assessing the viscoelastic properties of whole blood with particular reference to maximal fibrin clot formation, fibrinolysis and the tendency to hypercoagulability. As TEG properties can demonstrate the recipients’ coagulation balance, we hypothesized that intraoperatively performed thromboelastographic tracing could identify those patients at an increased risk of developing vascular early thrombotic (HAT and PVT) complications after LT.
MATERIALS AND METHODS
Following institutional review committee approval (No. 139/14 approved on October 29, 2014), 530 patients (≥ 18 years old) who underwent their first LT performed at the Liver University Transplant Center of Policlinico of Modena (Italy) from January 2002 to January 2015 were included in the study. Retransplantations and all combined liver and kidney transplant procedures were excluded. All data of the patients who underwent LT were retrospectively extracted from their medical records.
Early HAT and early PVT were defined as thrombotic complications that occurred within the first 21 d.
The patients with thrombotic complications were compared in a 1:1 match with the same number of nonconsecutive control patients who underwent LT in the same study period without developing these complications. The chosen matching parameters were: Patient graft and donor characteristics (age, sex, BMI), indication for transplantation, procedure details, United Network for Organ Sharing (UNOS) classification, body mass index (BMI), WIT, CIT, the volume of blood products transfused, and conventional laboratory coagulation analysis.
Liver transplants were performed following a standardized anesthetic protocol: The patients were monitored with two invasive radial artery blood pressure gauges. A two-lumen (14 Gauge) central venous catheter was inserted into the left jugular vein under echo-guidance, and a Swan-Ganz catheter was placed in the right jugular vein. General anesthesia induction was obtained with fentanyl (2-3 µg/kg), propofol (2-3 mg/kg) and cisatracurium (0.1-0.2 mg/kg), and maintained with desflurane following Bispectral Index monitoring (BIS, Medtronic®).
Additionally, a standard protocol for TEG (Thromboelastograph coagulation analyzer 5000C; Haemoscope Inc., Skokie, IL, United States) execution was followed: Native and heparinase TEGs were performed after radial artery placement before laparotomy, during the anhepatic phase, and 30, 60, 120 or 180 min postreperfusion. The number of postreperfusion TEG evaluations varied depending on the patient’s clinical condition and the length of the procedure. Additional TEGs were also performed per clinical need. Blood samples were always handled by the same three anesthesiologists. TEG tracings were started within 4 min after sampling. Clot formation was triggered by contact activation, and heparinase was used only after reperfusion in all cases to avoid interference from heparin coming from the liver graft. TEG variables analyzed were reaction time (R-time; nr: 12-26 min), clot formation time (K-time; nr: 3-13 min), α angle (nr: 14°-46°), maximum amplitude (MA; nr: 42-63 mm) and clot lysis 60 min after maximal amplitude (LY; nr: 0.81%-2.99%). The normal ranges for each of these variables, for native whole-blood samples, were obtained from the Haemoscope Corporation®.
Fibrinolysis, considered as the percentage of clot lysis 60 min after maximal amplitude (LY60) on baseline TEG, was differently classified in accordance to its value[13]: Fibrinolysis shutdown (FS) (LY60, 0%-0.80%), physiologic fibrinolysis (LY60, 0.81%-2.99%), and hyperfibrinolysis (LY60, ≥ 3.00%). All TEG MA data were converted to their respective G values before the analysis with a mathematical transformation: G = 5000 × MA (100-MA) where G is a unit of force (nr: 3200-7100 dyne/cm2). G value was considered an indicator of hypercoagulability if it was > than 7100 dyne/cm2. In all patients studied, basal and 120’ postreperfusion TEG values were retrieved from our hospital’s database.
The management of coagulopathy during surgery was led by TEG and based on the same hospital transfusion algorithm in both groups. We transfused erythrocyte concentrates to maintain hemoglobin levels at 8-9 g/dL. This policy was consistent throughout the study period.
The anesthesia team (3 anesthetists) and the surgical team (two main surgeons plus surgical fellows) did not change during the study period. All surgical procedures were performed using the piggy-back technique for graft implantation. Arterial reconstruction and portal vein anastomosis were similarly performed by the surgeons in the team. Additional anastomoses were required in cases of aberrant or complex vascular anatomy. Intraoperative Doppler ultrasound scans were always performed after hepatic artery and portal vein reconstruction.
In the postoperative period, all patients received thromboprophylaxis therapy with oral aspirin (75 mg/d, starting as soon as their platelet count was above 50 × 109/L), and low molecular weight heparin (0.5 mg/kg daily adjusted for renal function) as soon as any bleeding risk was excluded, usually starting on the second postoperative day.
方案组合数N=n1n2n3n4n5=48个,对方案中不相容的功能单元解进行删选剔除,得到原理方案如下:
We also evaluated other risk factors for HAT and PVT such as recipient characteristics, including age, sex, BMI, etiology of liver disease, UNOS status, and the presence or absence of hepatocellular carcinoma. Donor age, CIT, and WIT were evaluated as well. For surgical characteristics, the presence of a complex arterial reconstruction (placement of an arterial interposition graft or multiple anastomoses), presence of preoperative PVT, and intraoperative blood product transfusions (packed red blood cells, platelets, fresh-frozen plasma) were recorded and evaluated for correlations with thrombotic events.
Missing data for each variable analyzed were less than 95%.
Normally distributed continuous data are reported as the mean ± SD and compared using one-way Analysis of Variance (ANOVA). Non-normally distributed continuous data are reported as the median (interquartile range) and compared using the Mann–Whitney test. Categorical variables were analyzed with Chi-square tests with Yates correction or Fisher’s exact test depending on best applicability. IBM SPSS Statistics version 24 (SPSS Inc., Chicago, IL, United States) was employed for statistical analysis. Statistical significance was set atP< 0.05. The study was reviewed by our expert biostatistician, Montalti Roberto.
RESULTS
Five hundred and thirty adult patients underwent a first LT during the study period. Twenty-seven (5.09%) patients had postoperative early thrombosis. Early HAT was recorded in 16 (3.02%) patients, while early PVT developed in 11 patients (2.07%). The characteristics and preoperative laboratory findings of the patients with thrombotic complications and control cases with their indications for LT are displayed in Table 1.
There were no donor or graft characteristics associated with the diagnosis of HAT or PVT. Among the surgical-related characteristics, a longer duration of surgery was registered in the case group (390 ± 123 minvs324 ± 95 min,P= 0.032) (Table 2).
The number of patients transfused and the volumes of blood and blood products transfused were similar between the two groups (Table 3).
TEG Analysis
The preoperative and 120’ postreperfusion TEG values are shown in Table 4. No statistically significant differences in these values were observed between the two groups except for mean lysis 60 value at 120’ postreperfusion and basal and 120’ postreperfusion G value (Table 4). This value was higher in the case group compared to the control group (P= 0.001 andP< 0.001, respectively), although it did not indicate hypercoagulability at any time (Table 4). Lysis 60 at 120’ postreperfusion was lower in the case group (P= 0.035), showing a FS phenotype in 23 patients (85%) in the case groupvs15 patients (55%) in the control group (P= 0.043).
FS was the dominant fibrinolysis phenotype both at baseline (56%; 15/27 in the thrombosis group and 48%; 13/27 in the control group,P= 0.785) and at 120’ postreperfusion in both groups (85%; 23/27 in the case group and 55%; 15/27 in the control groupP= 0.037) (Table 5). Postoperative early HAT occurred in 15 of 16 (94%) recipients with the FS phenotype at 120’ postreperfusion TEG, while only one patient with early HAT had a physiologic fibrinolysis phenotype. Postoperative early PVT occurred in 8 (72%) recipients with the FS phenotype at 120’ postreperfusion TEG, while physiologic fibrinolysis and hyperfibrinolysis phenotypes were recorded in 2 (18%) and 1 (9%) patients, respectively, who had this portal complication (Table 5).
With regard to the other TEG values analyzed, in the case group, 19 of 27 patients (70%) and 20 of 27 patients (74%) in the control group had normal or faster clot formation (normal or minor R value) at the basal time (P= 1) (Table 5). The mean R value measured at 120’ postreperfusion was not significantly different between the two groups (P= 0.407) and was within the normal or shorter than the normal reference range in 21 patients (78%) in the case group and in 26 (96%) in the control group (P= 0.105). In the case group, 10 (37%) patientsvs14 (52%) patients in the control group had a normal or increased basal MA showing a normal or increased clot strength (P= 0.411). The MA value measured at 120’ postreperfusion was within the normal reference range or larger than the normal reference range in 8 patients (30%) in the case group and in 7 (26%) in the control group (P> 0.999) (Table 5).
DISCUSSION
In our patient population, the incidence of HAT was 3%. Although its etiology is known to have several causes and to be significantly associated with patient and surgical-related factors (difficulties associated with the arterial reconstruction), it is notable that in this study, 15 (94%) of 16 patients who developed early HAT had TEG evidence of FS on the 120’ postreperfusion TEG trace, a higher G value at basal and 120’ postreperfusion time, and a longer duration of surgery. Similarly, the incidence of PVT was 2%, and 8 (72%) of 11 patients who developed this complication had TEG evidence of FS at 120‘ postreperfusion.
Different to Krzanickiet al[14]and Lerneret al[15], who reported during LT that some TEG signs of hypercoagulability appeared in the patients who developed early HAT, in our series, except for a few patients, in general, the patients showed no signs of enhanced clot formation or clot strength. In particular, the MA value at 120’ postreperfusion TEG was larger than the normal reference range in only 4% of patientsin both groups. Only 18% and 14% of patients, respectively, in the case and control groups showed shorter than normal R time values at the same TEG time.
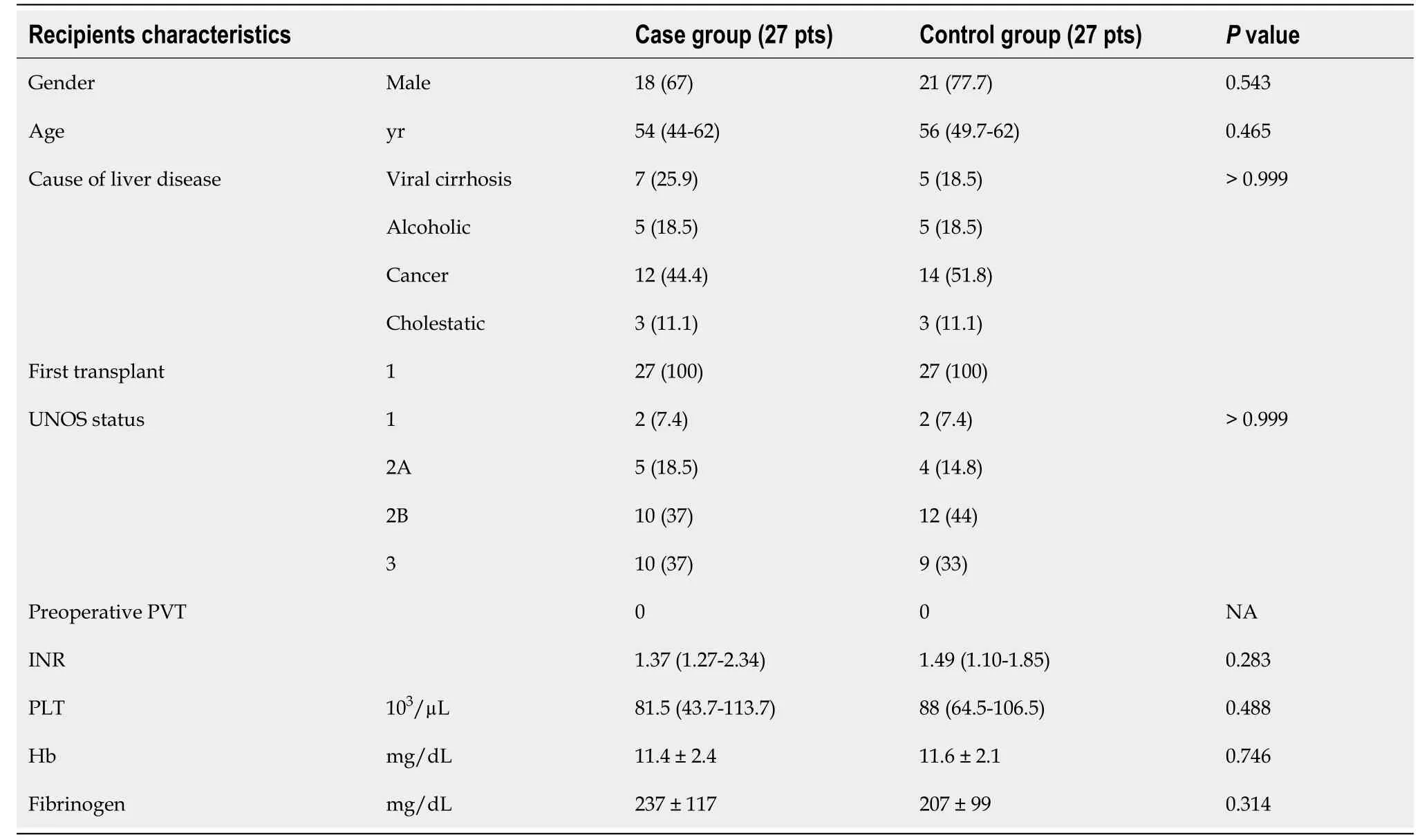
Table 1 Preoperative recipient characteristics, n (%)
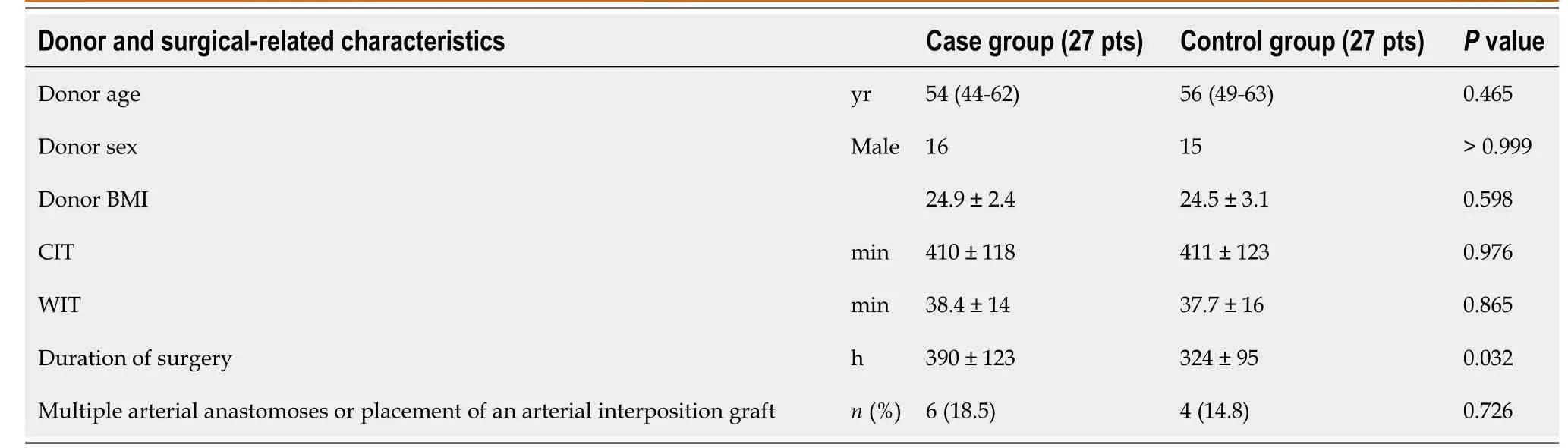
Table 2 Donor characteristics in the thrombosis group and control group
In liver recipients, Lerneret al[15]demonstrated a TEG hypercoagulablility in more than 70% of cases, and Zahret al[16]inferred that preoperative TEG might reliably detect groups of recipients with an increased risk of displaying early HAT in the preoperative period. Some enhanced coagulability at some point before or at the end of the LT procedure did not seem to be statistically significantly related to thrombotic events in our series. A total of 16 (60%) patients who developed a thrombotic complication in our study had a normal R time value at 120’ postreperfusion. These findings are in agreement with the more diffuse knowledge of the new hemostatic competence of cirrhotic patients, which has reduced the widespread fear of bleeding during LT in favor of a greater awareness of the thrombotic risk to which the patient is exposed[17-19].
In the postoperative period after LT, almost all of the procoagulant proteins need two to three days to reach normal activity, and the anticoagulant factors have adelayed recovery which is responsible for an imbalance of coagulation towards hypercoagulability lasting a variable period of time after LT. The old concept of the cirrhotic patient as an anticoagulated patient has been replaced[20,21]. Thrombocytopenia, typical of end-stage liver disease, is somehow compensated by a preserved platelet adhesion. Awareness of all these changes is responsible for shifting the focus on the possible thromboembolic complications of LT, justifying the need for more reliable tests capable of identifying patients at greater thrombotic risk[22].
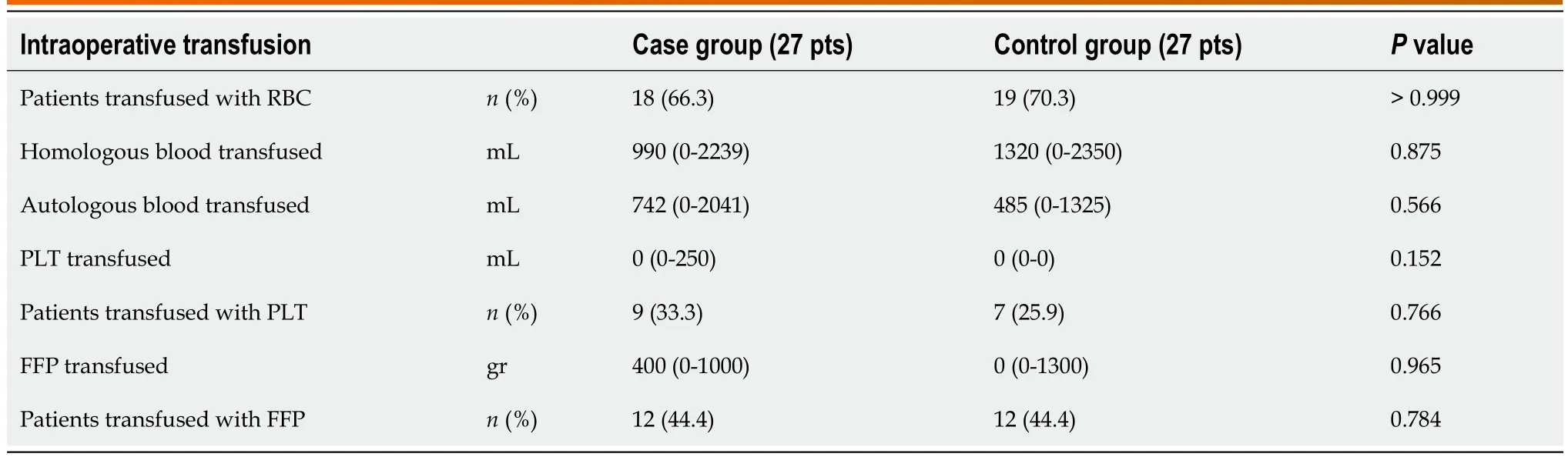
Table 3 Intraoperative transfusion and number of patients transfused in the case group and control group
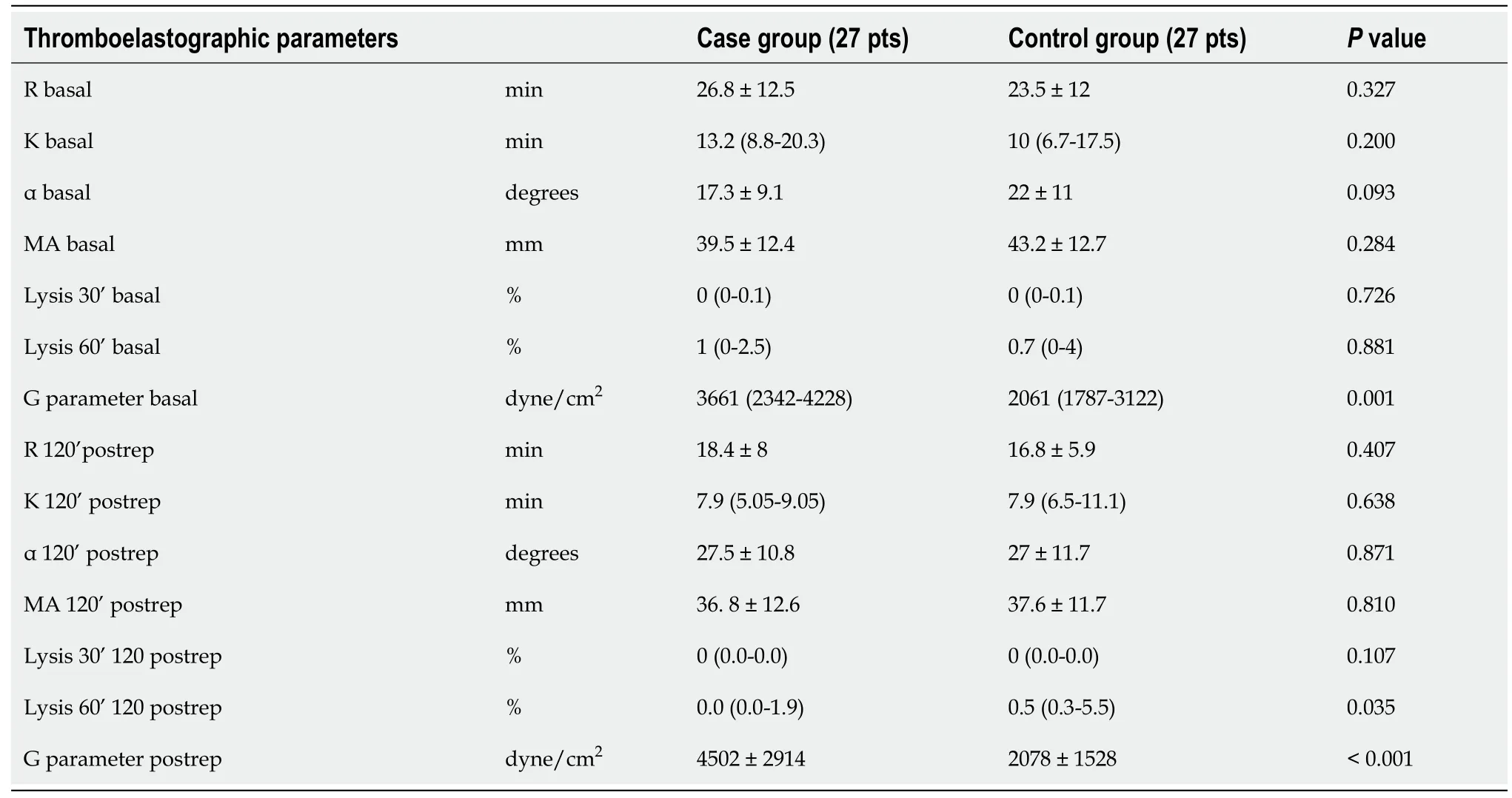
Table 4 Thromboelastographic variables were statistically different during liver transplantation and between the two study groups
Novel studies have begun to stress that a condition of perioperative hypercoagulability may be responsible for complications such as HAT, PVT and other systemic thrombotic events. MA is an expression of clot strength, reflecting platelet count and function, fibrinogen levels, and the interaction between platelets and fibrinogen. Specifically, in LT surgery, the MA value at preoperative TEG is an independent factor correlated with an increased incidence of early HAT[16]. A cut-off value of 65 mm was found by Area Under the Curve analysis, with a decent sensitivity of 70%: Above that value, the hazard ratio for early HAT was 5.28, suggesting it is a powerful screening tool that could be used to identify patients at risk of experiencing early HAT. Similarly, a greater than normal postoperative MA value, in a large series of patients undergoing various types of surgical procedures, has been shown to be a risk factor for postoperative thrombosis[23]. Maximum Clot Firmness, which is the equivalent of MA in ROTEM®, is abnormally increased and is correlated with a higher PVT risk in noncirrhotic patients and hepatocellular carcinoma and cholangio-carcinoma patients[24-26].

Table 5 Distributions of normal and abnormal thromboelastography parameters at different times during the observation period, n (%)
Different to these authors, in our case group, both basal MA and 120’ postreperfusion MA did not show any statistical correlation with thrombosis and was larger than normal in only 4% of patients. The majority of patients who had thrombotic complications in our series showed reduced cloth strength at the chosen time of observation, rejecting the role of increased clot strength as a risk factor for HAT or PVT. The absence of hypercoagulability findings among our patients was also confirmed by the G value, which similar to Krzanickiet al[14], was significantly related to HAT and PVT, but at no time during observation pointed to hypercoagulability. In particular, in the case group, the G value measured at basal and postreperfusion time was within the normal reference range compared to the control group where the G value pointed to mild hypocoagulability.
Different to other studies, we hypothesized that TEG performed 120’ postreperfusion is more comprehensive and clinically reliable than at basal for evaluating the coagulative status of the patients. It is extremely unlikely that the TEG performed at the beginning of the intervention is representative of the coagulation balance at the end of surgery. The surgical procedure itself, transfusions, volume shifts, the hemodynamic instability, and above all, the new graft, will not fail to influence the coagulation balance reached at the end of the intervention. It is reasonable that TEG at 120’ postreperfusion, more so than the basal value, is representative of the coagulation conditions responsible for an increased thrombotic risk. Similar to Nicolau-Raducuet al[13], in our study, FS was the dominant fibrinolysis phenotype in LT recipients at the basal time (48% in the control groupvs56% in the case group) and at 120’ postreperfusion (67% in the control groupvs85% in the case group).
Different to Nicolau-Raducuet al[13], in our study, the FS phenotype was significantly associated with thrombotic complications only for the 120’ postreperfusion TEG and not at the basal time. As explained, it is more probable that a thromboelastographic trace evaluated at the end of surgery is more representative of the risk of a thrombotic complication than a TEG performed at the beginning of the operation.
In LT, as in other settings the prothrombotic predisposition of an FS phenotype has been recognized to be associated with thrombotic complications as we have underlined in this study for early HAT and PVT[27,28]. Fibrinolysis represents a physiologic mechanism capable of maintaining microvascular patency by lysing excessive fibrin clots. It is conceivable that an FS phenotype found at the end of LT is responsible for the failure of this mechanism, causing HAT and PVT complications. The coagulation balance in the cirrhotic patient is extremely unstable and often unpredictable, and it is possible that the FS condition is an expression of an unstable coagulation status which can rapidly tend toward thrombosis. The use of viscoelastic tests in detecting a reduction of physiologic fibrinolysis during LT seems helpful in better hypothetically managing antifibrinolytic therapy or thromboprophylaxis. It remains unclear whether these tests during surgery could offer additional benefits, and considerable uncertainties persist regarding the accuracy of their measures[29]. However, our findings suggest that a reduction in fibrinolytic activity detected by viscoelastic testing identifies certain patients at risk for both PVT and HAT such that a causal relationship needs further research to demonstrate a conclusive link.
This study’s limitations are its retrospective nature, the limited sample size and the fact that the study did not prolong TEG evaluation into the postoperative period, making it difficult to draw conclusions on the persistence of the FS phenotype.
CONCLUSION
To our knowledge, this study is the first to analyze the possible correlation between TEG parameters measured at the end of surgery and thrombotic complications, and to associate fibrinolysis reduction (FS phenotypes) and a normal clot strength (G value) with vascular thrombotic complications. Despite no signs of hypercoagulability detected by viscoelastic testing, an FS phenotype with a normal clot strength seems to put certain patients in an at-risk group for thrombotic events.
ARTICLE HIGHLIGHTS
Research background
End-stage liver disease has been generally perceived as a hypocoagulable condition,related to an increase in bleeding risk in the case of invasive procedures. In cirrhotic patients, coagulopathy is a composite condition in which rebalanced hemostasis is realized by the simultaneous reduction in pro- and antihemostatic factors, responsible for a new hemostatic balance which can tip toward thrombosis or bleeding. In cirrhotic patients, the rebalanced coagulation, together with the reduction in hemorrhagic complications during liver transplantation have made surgeons and anesthetists more conscious and frightened of possible venous or arterial thrombotic events.
Research motivation
Thrombotic events associated with liver transplantation (LT) may be more frequent than believed in the past, sometimes representing a potential risk to patients' lives and organ survival. Changes in the hemostatic system, intra- and postoperative blood products transfusion and surgical causes may contribute to the development of vessel thrombosis. Independent of the real cause of the prothrombotic status, more efforts on the rapid detection and prevention of such complications are necessary.
Due to the limits of conventional coagulation tests in recognizing alterations in the hemostatic balance, in recent years viscoelastic tests, such as thromboelastography(TEG), have gained increasing importance. The use of TEG in identifying hypercoagulation status during LT has been shown to be useful in better guiding blood product transfusion or, theoretically, prophylactic therapy. If its usefulness in identifying coagulopathy has already been shown in LT, its ability to recognize hypercoagulation has yet to be demonstrated.
Research objectives
Encouraging results suggest that hypercoagulability detected by TEG can increase the probability of venous or arterial thrombotic complications in certain patients. The presence of hypercoagulability, represented by TEG variables, can be predictive of thromboembolic complications in patients following surgery. In the present study, we aimed to verify if patients who developed hepatic artery or portal vein thrombotic complications showed predictive thromboelastographic indices which can be used for early detection of these complications in patients at greater risk.
Research methods
To achieve our objective, we adopted a retrospective case-control study. The goal was to determine if there was an association between the risk factor (specific TEG variables) and the outcome of interest [hepatic artery thrombosis (HAT) and portal vein thrombosis (PVT)]. We hypothesized that TEG performed 120’ postreperfusion is more comprehensive and clinically reliable than at basal for evaluating the coagulative status of the patients.
Research results
A comparison between the case and control groups showed some statistically significant differences in the duration of surgery (longer in the case group;P= 0.032) and in two thromboelastographic parameters (G value measured at basal and 120’ postreperfusion time and LY60 measured at 120’ postreperfusion time). G value, a mathematical conversion of the MA value, was higher, although within the reference range, in the case group than in the control group (P= 0.001 andP< 0.001, respectively). In addition, LY60 measured at 120’ postreperfusion time was lower in the case group than in the control group (P= 0.035). This parameter is representative of a fibrinolysis shutdown in 85% of patients who experienced a thrombotic complication, resulting in a statistical correlation with HAT and PVT. Given the retrospective nature of our study, further research is needed in this area, but postoperative TEG seems to be a more accurate surrogate marker for the "real" hemostatic balance in recipients, possibly identifying those patients with a postoperative condition that increases the risk of HAT or PVT.
Research conclusions
Our study suggests that TEG can be used to identify patients at an increased risk of thromboembolic events due to postoperative normal clot strength or fibrinolysis reduction, directing appropriate and more intense investigations to detect early HAT and PVT. Thromboelastography identification of an increased thrombotic risk, may also suggest the more frequent use of thromboprophylaxis.
Research perspectives
Our findings suggest that a reduction in fibrinolytic activity and a normal clot strength (G value) detected by viscoelastic tests, identify some patients at risk of both PVT and HAT. This causal relationship requires further research to prove a conclusive link. Large randomized controlled trials could help in the stratification of patients with a higher postoperative thrombotic tendency eventually directing postoperative thromboprophylaxis and more intense surveillance to maximize the likelihood of early diagnosis.
猜你喜欢
现代仪器与医疗(2022年3期)2022-08-12
好日子(2022年3期)2022-06-01
当代陕西(2021年21期)2022-01-19
一重技术(2021年5期)2022-01-18
湘潮(上半月)(2021年4期)2021-07-20
电子制作(2019年22期)2020-01-14
汽车维修与保养(2019年7期)2020-01-06
陕西画报(2018年6期)2018-02-25
数码精品世界(2009年3期)2009-03-30
中学数学杂志(高中版)(2006年4期)2006-07-19
 World Journal of Transplantation2020年11期
World Journal of Transplantation2020年11期
- World Journal of Transplantation的其它文章
- Torque teno virus in liver diseases and after liver transplantation
- Lenvatinib as first-line therapy for recurrent hepatocellular carcinoma after liver transplantation: Is the current evidence applicable to these patients?
- Donor-specific cell-free DNA as a biomarker in liver transplantation: A review
- Obstetrical and gynecologic challenges in the liver transplant patient
- Extracellular vesicles as mediators of alloimmunity and their therapeutic potential in liver transplantation
- Exploring the safety and efficacy of adding ketoconazole to tacrolimus in pediatric renal transplant immunosuppression