
Use of mobile-stroke risk scale and lifestyle guidance promote healthy lifestyles and decrease stroke risk factors
2020-11-26 13:00KelanaKusumaDharmaParellangi
Kelana Kusuma Dharma ,Parellangi
a School of Nursing,Politeknik Kesehatan Kementerian Kesehatan Pontianak,Indonesia
b School of Nursing,Politeknik Kesehatan Kementerian Kesehatan Kalimantan Timur,Indonesia
Keywords:Health promotion Life style Mobile applications Risk factors Stroke
ABSTRACT Objective:The purpose of this study was to determine the effectiveness of Mobile-Stroke Risk Scale and Life Style Guidance (M-SRSguide) in promoting a healthy lifestyle and reducing stroke risk factors in atrisk persons.Methods:This research was an clinical trial with a pre-test and post-test control group design.The accessible population is persons at risk of stroke in the community(West and East Kalimantan Province,Indonesia).Thirty-two participants in the intervention group and 32 participants in the control group participated in this study.The sampling method was systematic random sampling.We allocate the sample into the intervention and control groups using a randomized block design.The intervention group used the M-SRSguide.The control group used manual book for a self-assessment of stroke risk.The measurement of a healthy lifestyle and the stroke risk factors was performed before and six months after the intervention.Results:There are no significant differences in healthy lifestyle and stroke risk factors between the two groups after the intervention (P > 0.05).Analysis of healthy lifestyle behavior assessment items in the intervention group showed an increase in healthy diets,activity patterns,and stress control after the use of the M-SRSguide (P < 0.01).Conclusion:The use of M-SRSguide is effective in promoting a healthy lifestyle.
What is known?
· Long-time rehabilitation periods after a stroke lead to significant economic burdens on the health care system.
· The use of information technology that can be installed in the smartphone is potentially developed to prevent stroke attack.
· The Mobile-Stroke Risk Scale and Life Style Guidance (MSRSguide) is a simple open-source progressive web application that can be installed on a smartphone or accessed on the website,used to determine stroke risk,offers instructions for a healthy lifestyle based on current risk levels,and information on health programs at public health centers closest to an individual’s home.
What is new?
· The use of the M-SRSguide application can increase healthy lifestyles especially in healthy diets,activity patterns,and stress control.
1.Introduction
The World Health Organization (WHO) estimates that noncommunicable diseases (NCDs) are the biggest causes of death:41 million people die every year because of NCDs(71%of all deaths globally) [1].Data from basic health research shows that stroke prevalence in Indonesia based on diagnosis by health professionals or symptoms was 12.1 per million in people 15 years and older in 2013[2].An increase in the number of stroke patients,a decrease in quality of life,and long-time rehabilitation periods lead to significant economic burdens on the health care system.It is estimated that the total direct and indirect costs due to stroke in the United States in 2008 was US$65.5 billion.Direct costs accounted for 67%of the total costs,while the remaining 33%were from indirect costs[3].Funding through health insurance will not be enough if degenerative diseases such as stroke are not controlled and prevented.Preventive efforts are needed by using information technology relevant to developments in the era of globalization and industry 4.0.Today,most people in urban and rural areas use smartphones not only for communicative functions but also to access various information and share stories on social media.A survey from the Indonesian Internet Service Providers Association showed that the number of internet users in Indonesia in 2018 was 171.18 million or approximately 64.8% of the total population [4].
We need to develop a web progressive or smartphone application for a self-assessment of stroke risk that is linked to the recommended healthy life according to a person’s needs,which are determined in consultation with the health care provider.This mobile health (m-health) application can be integrated into the national health service system that is used to increase awareness of healthy living and prevent degenerative diseases,especially stroke,in at-risk populations.Several studies have developed m-health applications containing information about health and disease that aims to promote health,prevent disease,and treat patients.The mhealth application features widely used in previous studies include the assessment of disease symptoms,health program reminders,or feedback for participants who provide their data in the application[5].To date,there is no integrated m-health application that has been developed to determine the level of risk of people suffering from disease and at the same time giving healthy lifestyle guidance according to the level of risk they experience,or providing homecare instructions and information about the nearest health facility accessible to patients.
The Mobile-Stroke Risk Scale and Life Style Guidance (MSRSguide)is a simple open-source progressive web application that can be installed on a smartphone/computer or accessed on the website.It is used to determine stroke risk and offers instructions for a healthy lifestyle based on current risk levels.It provides access to stroke information media offering general information as well as information about signs and initial symptoms,early stroke treatment at home,post-stroke rehabilitation,and information on health programs at public health centers or hospitals closest to an individual’s home.This mobile application aims to give information to people at risk of stroke,increase self-awareness about stroke risk,guide healthy lifestyles,and to offer information on the closest health facilities.
There are no significant obstacles to using M-SRSguide because most of Indonesia’s population now use smartphones and are connected to the Internet.Telecommunications providers are now entering rural areas,making it easier for residents to get access to information or applications through websites.Respondents can also use M-SRSguide offline.However,this limits the ability to find the nearest health care facilities available and prevents online communication with health professionals.Using M-SRSguide does not require high costs because this application is an open-source progressive web application.Respondents only need to use an Internet data package every day to access this application.
Using M-SRSguide does not require special training.There is a manual book containing instructions for using the application,including how to install the application and steps for using the features of the application.M-SRSguide can be easily replicated and disseminated because it is open-source and can be used by many operating systems on smartphones/computers.All content and information are in line with the government health programs and national guidelines for handling non-communicable diseases.MSRSguide is an intervention for the promotion and prevention of stroke in people at risk that can be integrated into health information systems at public health centers throughout Indonesia.Using this application is personal,confidential,and can be easily used by respondents and health professionals,so it can be widely accepted and spread in the community.The content and language of M-SRSguide are Indonesian,but it will be developed in English so that it can be used worldwide.The purpose of this study is to determine the effectiveness of M-SRSguide in promoting healthy lifestyles and reducing stroke risk factors in at-risk people.
2.Method
2.1.Research design
It was a clinical trial with a pre-and post-test control group design.
2.2.Setting and sample
We recruited people at risk of stroke who met the eligibility criteria for the sample:having a risk of stroke in the category of moderate or severe,aged 40-65 years,never had a stroke before,and not undergoing treatment because of chronic illness.We used the Stroke Risk Scorecard(SRS)to determine the risk of stroke.The list of accessible populations (name,address,sex,marital status,education level,occupation,age) was obtained from medical records at 2 Public Health Centers (PHCs) in Singkawang City,2 in Pontianak City West Kalimantan Province,and 4 in Samarinda City East Kalimantan Province (patients go to PHCs for medical checkups).The sampling method used in this study was systematic random sampling.After determining the sample,we conducted a random assignment using a randomized block design.We used a random number table to determine the sequence numbers of the sample which will allocate.The selected sample was entered into the intervention group (A) or the control group (B) using a sequence of 2 blocks.If the numbers 0-4 appear according to the random number table,then the order of sample allocation is AB(intervention-control).Meanwhile,if the numbers 5-9 appear,the sample allocation sequence is BA (control-intervention).We conducted home visits to give interventions to the sample selected.
2.3.Sample size calculation
We used the formula of hypothesis testing for the difference between two population means (two-sided test) to calculate the sample size as [6]:

Based on the formula above,the minimum number of samples for each group is 32 samples.We base it on calculations of the mean difference of healthy lifestyles between the two groups(δ=4),the assumption of maximum lost-to-follow-up of 0.82%,5% α,and power of the test of 80%.There were no samples dropped out or loss of follow-up during the study.
2.4.Procedure
2.4.1.Intervention
M-SRSguide is an open-source progressive web application that can be accessed via smartphone/tablet/computer online to determine the level of stroke risk independently,find individual healthy lifestyle guidelines,information media explaining stroke,early signs and symptoms,initial treatment at home,post-stroke home care information for high-risk individuals,and information about nearby health care facilities.This application also provides features for respondents to communicate with health professionals,so they can find out information about stroke prevention and healthy lifestyles.The infrastructure needed to operate M-SRSguide includes smartphone/tablet/computer with many suitable operating systems,M-SRSguide software that can be accessed and installed by visiting the link https://app-M-SRSguide.id/,and an Internet network to connect the respondent’s device with the MSRSguide website(Appendix A).
The development process of the M-SRSguide application is evidence-based through the following stages:1)developing the MSRSguide workflow and its features; 2) developing a database containing the scale of stroke risk,information about stroke and instructions for individual healthy living;3)inputting the database into the application system;4)compiling a manual book;5)testing the content validity of the application database by consulting with a clinical neurologist consultant; 6) testing the use of the MSRSguide application in a small group;7)and revising the database and application features.The flow of the M-SRSguide application and its features can be seen in Fig.1.
The intervention of the M-SRSguide group was carried out in 3 stages:intervention,monitoring,and evaluation.
(1) Intervention:
a.We taught participants in a demonstration on how to install and use the M-SRSguide application on a smartphone within 1 h.
b.We asked participants to conduct a self-assessment of stroke risk factors and save the results in the application.
c.We asked participants to read the instructions for the individual healthy lifestyle.
d.We asked participants to give a checklist in the monitoring sheet each time they conducted a self-assessment of stroke risk and read instructions for a healthy lifestyle.For those with a high level of risk,reading about the signs and symptoms of a stroke and initial management at home was recommended.
e.We asked participants to access features related to health care facilities closest to their location to find out the services available,including non-communicable disease prevention services.
f.If participants experienced difficulties,they could communicate with clinical staff through the message features available in the application.We used the clinical staff to manage this application because it will be integrated into the current promotional and preventive health program.
(2) Monitoring:Monitoring was carried out in the fourth week of every month for 6 months (6 times monitoring).The researcher looked at participants’ notes on the monitoring sheet.We gave feedback to the participant if we found some unusual information on the monitoring sheet.
(3) Evaluation:The evaluation was carried out at the end of the sixth month to determine healthy living behavior and stroke risk factors.
2.4.2.Control
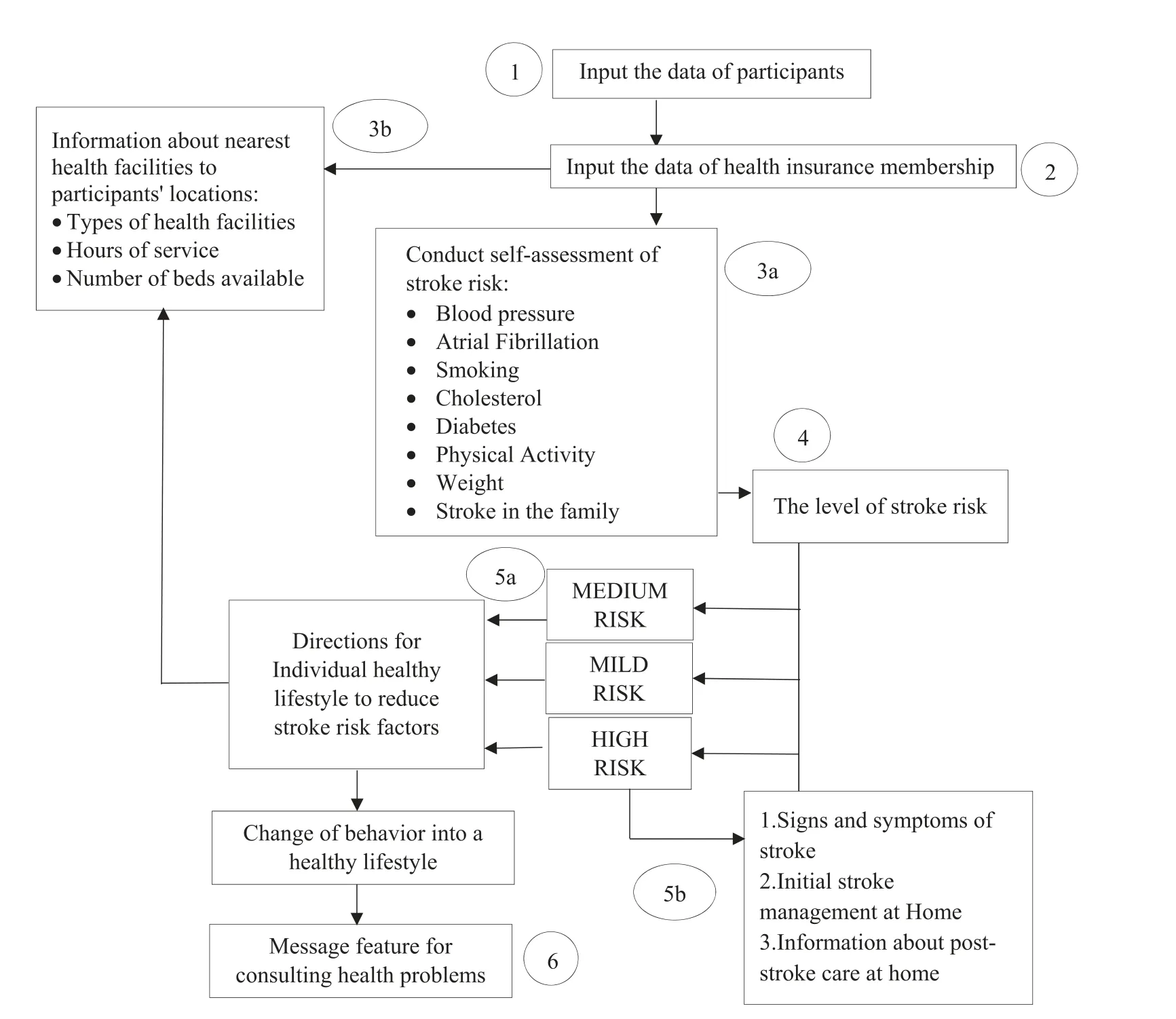
Fig.1.Flowchart of Mobile-Stroke Risk Scale and Life Style Guidance feature.
The control group obtained a manual book for a self-assessment of stroke risk,general information on strokes,and tips for a healthy lifestyle to prevent stroke.We taught participants how to use the manual book,including how to do a self-assessment of stroke risk and learn a healthy lifestyle from the manual book provided.The information in the manual book is the same as that in the MSRSguide application.We monitored and evaluated the control group in the same way as the M-SRSguide group.
2.5.Data collection
We collected the data for 6 months,from January to June 2019.We use trained and standardized observers to measure healthy lifestyles and stroke risk.We used the principle of single-blind measurement; the observers did not know to which group the measured samples were allocated.The tools used to collect the data were The Simple Lifestyle Indicator Questionnaire (SLIQ) to measure the healthy lifestyle variable[7]and the Stroke Risk Scorecard(SRS) to measure stroke risk [8].We collected the data twice-before the intervention and the sixth month after the intervention.
The SLIQ consists of 12 questions in 5 categories(3 on diet,3 on physical activity,3 on alcohol consumption,2 on smoking,and 1 on stress).Psychometric testing of the SLIQ proved this instrument has a very good test-retest reliability,good internal consistency,and good external validity.Test-retest reliability coefficients of each question on the SLIQ ranged from 0.63 to 0.97.The correlation coefficient(r)between SLIQ scores and blinded reviewers’scores was 0.77 (P=0.001) [7].The SRS consisted of 8 items such as blood pressure,atrial fibrillation,smoking,cholesterol,diabetes,exercise,weight,and stroke in the family.Each item was given a score of 0-2 according to the appropriate category,while body weight was scored using a body mass index.The higher the score,the more risk a person has of a stroke.The SRS has been widely used in research,including Alzahrani et al.[9],Srywahyuni et al.[10],Hasan et al.[11],and Aycock et al.[12].
2.6.Data analysis
Data analysis in this study was conducted using bivariate and multivariate tests.We conducted the bivariate test to check the equality of characteristics between the two groups,the equality of the pre-test between groups,the difference in post-test results between groups(independent t-test),and differences between the pre-test and post-test in each group (paired t-test).This analysis aimed to determine the effectiveness of the M-SRSguide application on promoting a healthy lifestyle and reducing stroke risk factors.
2.7.Ethical aspects
This study was passed the ethical research review by The Ethical Clearance Division before the clinical trail,and participants’written informed consents were obtained before data collection.
3.Results
Participants who took part in this study totaled 64 people,32 in the intervention group and 32 in the control group.No participants were dropping out or lost during follow-up in this study (Fig.2).Table 1 shows the descriptive statistic of participants in this study.There were no significant differences in the participant characteristics in terms of gender,marital status,education,occupation,and age between the two groups.
The independent t-test showed no significant differences between the groups in lifestyle behavior before intervention (pretest)(Table 2).Healthy lifestyle behaviors increased in both groups after the intervention.The mean score for lifestyle behavior in the intervention group increased from 16.59 to 19.16,while in the control group it increased from 16.75 to 18.06.Further analysis showed that there were no significant differences between the groups in healthy lifestyles after the intervention.These results prove that the two interventions can promote healthy lifestyles in people at risk of stroke,but the use of the M-SRSguide indicated greater improvement.Analysis of healthy lifestyle behavior assessment items in the intervention group showed an increase in healthy diets,activity patterns,and stress control after the use of the M-SRSguide.There were no respondents consume alcohol in this study.There was no change in smoking habits after the use of this application (Table 3).The results confirm that the use of MSRSguide can improve healthy lifestyle behavior in terms of diet,activity,and control of stress.
The independent t-test showed no significant differences between groups in stroke risk factors before intervention (Table 2).Stroke risk after the intervention significantly decreased in both groups.The risk factor score in the intervention group decreased from 32.91 to 30.47 after the intervention,whereas in the control group it decreased from 32.19 to 30.81.The independent t-test revealed that there was no significant difference between the groups in stroke risk factors after the intervention.Although both groups had a decrease in stroke risk factors,the M-SRSguide group had a greater decrease.These results prove that both interventions reduce stroke risk factors in at-risk people,but the use of the MSRSguide led to a greater reduction in stroke risk factors.
4.Discussion
This study proves that the use of the M-SRSguide in the intervention group and the self-assessment guide book for stroke risk/individual guidelines for healthy living in the control group both increase healthy behavior and reduce stroke risk factors in at-risk people.However,the use of the M-SRSguide application reveals an increase in healthy living behaviors compared to the use of conventional books.Analysis of the M-SRSguide’s effect on healthy living behavior shows that the use of this application can support a healthy lifestyle about diet,activity patterns,and control of stress.
The use of information technology in the prevention of noncommunicable diseases has opportunities to be widely developed,especially those that can be integrated into smartphones.This is possible because of the widespread use of smartphones at the moment.The spread of smartphone and internet users is prevalent not only in urban areas but also in rural areas due to service provider network expansion[4].In the past year,there has been an increase in people’s interest in using information technology to support changes in their health behavior.This contributes to increasing self-control over one’s health and lifestyle choices.Using information technology in assisting treatment,rehabilitation,and self-care efforts can save on costs and be potentially widely accepted by the community [13].This is in line with a systematic review of the impact of using m-health applications on patient clinical outcomes,treatment processes,treatment costs,and quality of life in low-and middle-income countries.The results of the review prove that m-health is a potential tool for increasing access and covering health services as well as reducing health service gaps in developing countries.Interventions using m-health have a positive impact on chronic diseases in low-and middle-income countries [14].
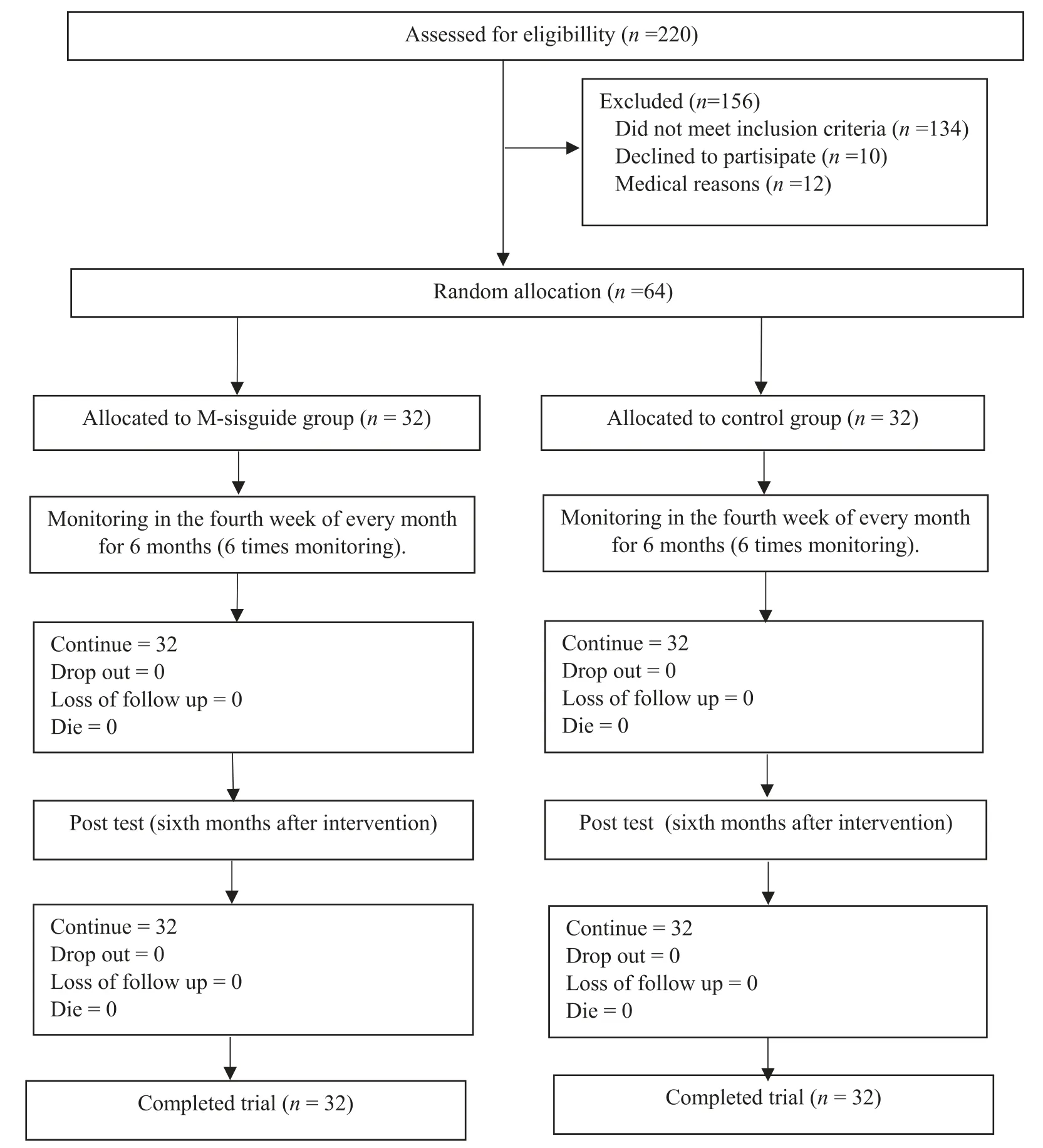
Fig.2.Flowchart of the trial.
The M-SRSguide allows participants to know their current level of stroke risk and specific suggestions for reducing these risk factors.The availability of this feature increases their awareness of the stroke risk factors,thus motivating them to seek further information about what they need to do to reduce risk factors and prevent strokes.This is evidenced by the respondents’ answers to the survey question:“After knowing the level of stroke risk from the M-SRSguide application,do you wish to have specific suggestions for avoiding a stroke?”,All respondents at high risk of stroke(100%) said that they wanted to know the specific advice for themselves,while 80% of the respondents at moderate risk were very curious,and 20%were not interested.This data shows that the more respondents know about their risk of stroke,the higher their intention to find specific suggestions for lifestyle changes and reduce the level of stroke risk.The six-month program using the MSRSguide application is enough to change the behavior of participants,including adding physical activity at least once a week and changing the diet to a healthier one,as recommended.Likewise,the ability to control stress increases with increasing awareness of how to prevent a stroke.Using the M-SRSguide could not change smoking behavior due to many other factors that influence smoking behavior,such as environmental factors and family support.
Education on healthy living for people at risk is needed to reduce the risk factors of stroke and prevent stroke recurrence.Research shows there are high-risk factors for stroke in patients before they have a stroke.Research conducted on 4467 stroke patients aged 40-51 years revealed the highest risk factors were smoking (55.5%),lack of physical activity (48.2%),hypertension(46.6%),dyslipidemia (34.9%),and obesity (22.3%).Increasing age will increase risk factors such as lack of physical activity,hypertension,dyslipidemia,obesity,and diabetes mellitus [15].Some studies also prove that most post-stroke patients still exhibit unhealthy living behaviors,thereby increasing the risk of recurrent strokes.Redfern et al.prove that one year after a stroke,22% of patients still smoked,36% were obese,and 4% still consumed alcohol[16].Koenig et al.proved most patients(52%)did not know the risk factors for stroke,35% could not explain the initial treatment if a family member had a stroke,28% did not comply with treatment,and 26% did not do the medical checkup [17].
Using the M-SRSguide as a tool to assess the risk of stroke and provide information about a healthy lifestyle has been shown to reduce stroke risk factors.Decreasing stroke risk factors can reduce the incidence of strokes.Sone et al.proved that the incidence of stroke recurrence in the group of participants who were givenlifestyle interventions was lower than in the conventional group[18].Other research conducted by Zang et al.proves that healthy living behaviors are associated with stroke risk:the more respondents apply healthy living behaviors,the fewer risk factors for stroke they have[19].There is an inverse relationship between the number of healthy lifestyle indicators and the total risk of stroke,the incidence of ischemic stroke,and hemorrhagic stroke.
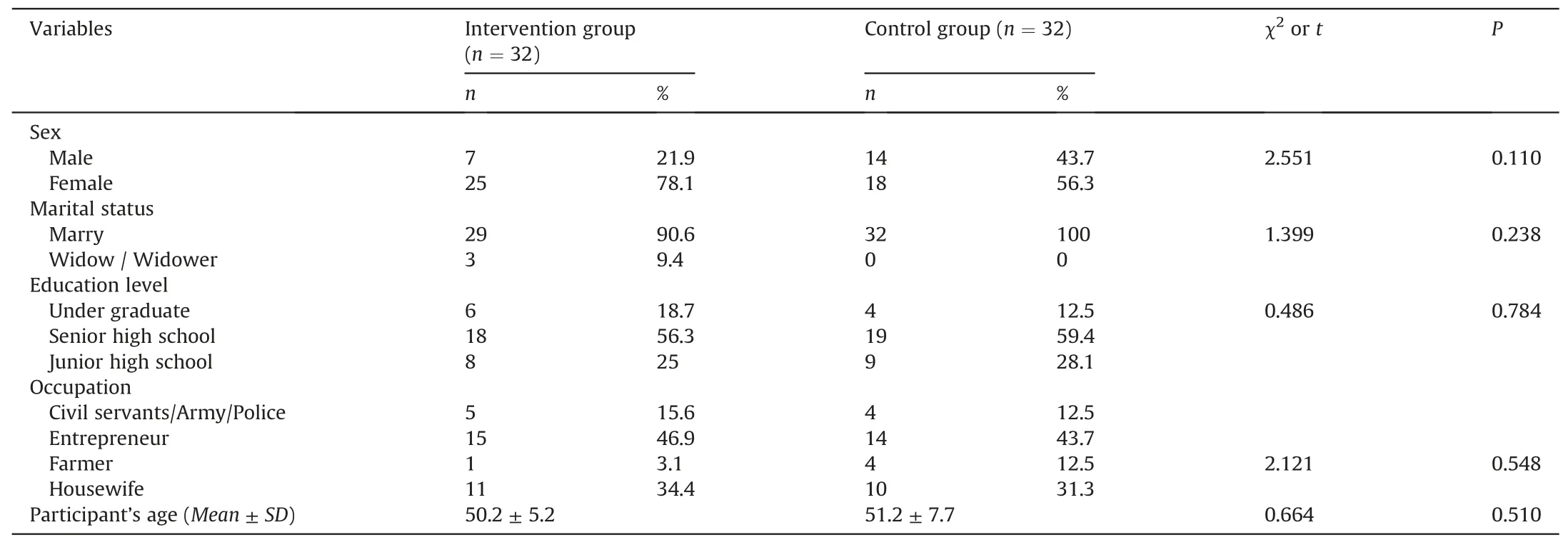
Table 1 The characteristics of participants (n=64).
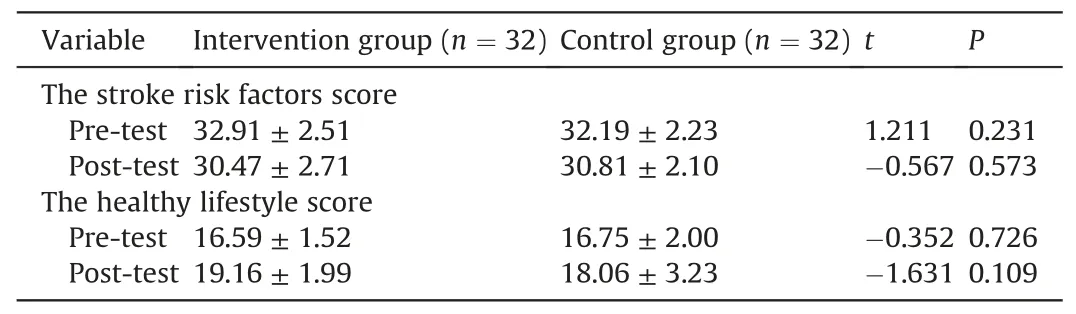
Table 2 The stroke risk factors score and healthy lifestyle score,pre-and post-test in the intervention and control groups(Mean ± SD).
Systematic reviews and meta-analyses about the positive impact of using m-health for secondary prevention in heart-disease patients verify that the group of respondents who received interventions using m-health experienced increased adherence to medical therapy,the ability to achieve optimal blood pressure targets,increased achievement of physical exercise goals,decreased anxiety and increased awareness of diet and exercise [20].The results of the review indicate the opposite:There is no increase in efforts to quit smoking,the ability to meet low-density lipoprotein(LDL) cholesterol targets are not increasing,and there is the same frequency of recurrence [20].Other studies on the feasibility of mobile applications for monitoring and management of stroke risk factors ascertain that respondents using this application have a significant increase in the achievement of target blood pressure andglycated hemoglobin(HbA1c)[21].Carter et al.confirm that the use of mobile health applications in obese patients encourages them to know their calorie intakes and physical activity more effectively than conventional interventions [22].
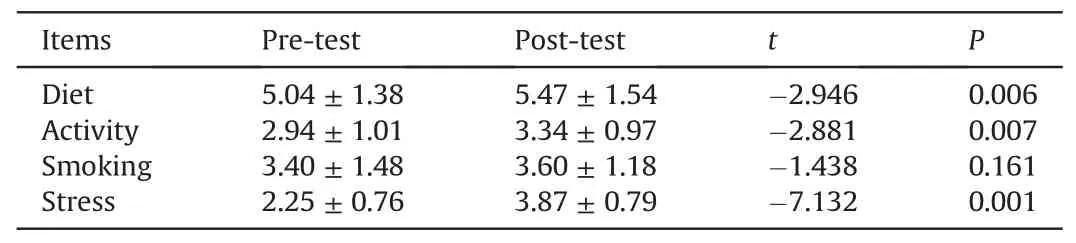
Table 3 The change of healthy life behavior pre-and post-intervention in the intervention group(Mean ± SD).
Using mobile health applications also provides high leverage in helping to improve outcomes in the management of chronic diseases.Several studies have demonstrated the effectiveness of mobile applications in improving health behavior,preventing disease,curing disease,and post-disease rehabilitation.A systematic review of the effectiveness of behavioral interventions using m-health applications in chronic disease management proves that the use of these applications is beneficial in improving self-management and some health outcomes.Ten randomized controlled trials(RCTs)out of a total of 12 reviewed showed significant improvements in several health outcomes [5].García et al.developed the m-health application to detect and monitor stroke signs and symptoms using cloud services.This application detects stroke through 3 signs and symptoms,including a smile to determine facial symmetry,voice to determine whether a sentence is pronounced correctly,and arm movements to determine motor ability in extremities.The results verified the ability of this application to detect stroke symptoms[23].The use of smartphone applications for diabetic patients combined with a weekly text message (SMS) support from healthcare professionals increased glycemic control in type 1 diabetes patients [24].Other studies have shown that patients attending cardiac rehabilitation and using smartphone-based applications have increased control of cardiovascular risk factors and decreased the risk of being hospitalized within 90 days after discharge [25].
This study shows a slight difference in stroke risk and a healthy lifestyle after the intervention in both groups.This shows that the use of the M-SRSguide application provides little leverage in promoting a healthy lifestyle and decrease stroke risk compared to the manual book.We analyze that this is because the substance of stroke risk self-assessment and personal healthy lifestyle information using the manual book in the control group is the same as the M-SRSguide application in the intervention group.A big difference can be achieved if participants read more information in the M-SRSguide application and apply it in everyday life.In this case,we need to simplify the use of features in the application and change the appearance of the M-SRSguide,so that it is more attractive for the participants.The other limitation of this study is in the area of generalization.The study is limited to the population at risk of stroke who have devices such as smartphones/laptops that are connected to the Internet.The results of this study cannot be applied to people who are not accustomed to smartphones and to those who have difficulty accessing information from mobile applications.
5.Conclusion
We conclude that the use of the M-SRSguide application and manual book for self-assessment of stroke risk as well as general information about strokes increase healthy lifestyles and decrease the risk factors for stroke among at-risk people.However,the use of the M-SRSguide is better for encouraging healthy lifestyles and decreasing stroke risk factors compared to the use of the manual book among people at risk.This application is a potential tool that can be used for self-assessment and as information media for people at risk of stroke.
CRediT authorship contribution statement
Kelana Kusuma Dharma:Conceptualization,Methodology,Formal analysis,Investigation,Data curation,Writing -original draft,Writing -review & editing,Supervision,Project administration,Funding acquisition.Parellangi:Software,Validation,Investigation,Resources,Data curation,Visualization.
Declaration of competing interest
There is no conflict of interest of all researchers in this study.
Acknowledgment
We thank the Politeknik Kesehatan Kementerian Kesehatan Indonesia,LB.01.01/I.1/2657/2019 for funding this study,the respondents for participating in this study,and Marshall Godwin for granting permission to use the Simple Lifestyle Indicator Questionnaire (SLIQ).
Appendix.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2020.08.001.
 International Journal of Nursing Sciences2020年4期
International Journal of Nursing Sciences2020年4期
- International Journal of Nursing Sciences的其它文章
- Demands of experiential training for ICU nurses in Hunan of China
- The risk factors of postpartum urinary retention after vaginal delivery:A systematic review
- Community health nursing courses in baccalaureate nursing programs in China:A descriptive study based on website information
- An exploration of the breastfeeding behaviors of women after cesarean section:A qualitative study
- Understanding autism spectrum disorder and coping mechanism by parents:An explorative study
- Theory-guided interventions for Chinese patients to adapt to heart failure:A quasi-experimental study