
Rectosigmoid perforation after high-pressure air jet exposure: A case report
2020-11-09 08:23:42SumanRastogiAnandhiDevendiranDivankurKhannaNandaKishoreMarojuKNJPrakashRaju
Journal of Acute Disease 2020年6期
Suman Rastogi, Anandhi Devendiran✉, Divankur Khanna, Nanda Kishore Maroju, KNJ Prakash Raju
Department of 1Emergency Medicine & Trauma, 2Surgery, Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), Puducherry,India
ABSTRACT Rationale: Colonic barotrauma induced by high-pressure air compressors has been reported more frequently these days due to the widespread use of air compressors in industries. Such enormous pressure into the rectum can lead to devastating injuries.Patient’s concern: A 35-year-old male was referred to our emergency department with an alleged history of directing high pressure compressed air jet towards the anus. There was diffuse subcutaneous emphysema over the neck, chest, abdomen, and extremities, and he presented with hemodynamic instability and respiratory failure.Diagnosis: Rectosigmoid perforation due to exposure to high-pressure air jet causing tension pneumoperitoneum,pneumomediastinum, pneumothorax, and extensive subcutaneous emphysema.Intervention: In view of tension pneumoperitoneum, urgent percutaneous needle decompression was performed using 16 G needle, 5 cm superomedial to the anterior superior iliac spine.The gush of air was released along with reduction in abdominal distension and improvement in hemodynamics.Outcome: The patient succumbed two days later due to septic shock.Lessons: This case highlighted the importance of promoting education about work safety among industrial workers especially in developing countries like India.
KEYWORDS: Compressed air; Ruptured colon; Colonic barotraumas; Mediastinal emphysema
1. Introduction
Colon barotrauma includes colon mucosal traumas and colon perforation due to elevated intraluminal pressure, which is mainly caused by high-pressure air. Air insufflation during colonoscopy procedure is the most common cause of iatrogenic colon barotrauma. Few cases of multiple perforations of the colon due to non-iatrogenic barotrauma are also mentioned in the literature.Compressed air is being widely used in industries and daily life for a variety of purposes. However, improper or negligent use of compressed air equipment may lead to devastating events[1]. The air pressure used in industrial purposes is usually over-exceed those used in medical applications such as colonoscopy. High air pressures can cause extensive injuries to the intestines leading to high mortality[2]. Compressed air injuries should be considered as a life-threatening trauma because the high pressure of compressed air into the rectum in a very short time can overcome barriers of clothes and anal sphincter and deliver a tremendous amount of pressurized air into the rectum, resulting in rectal and colonic perforation, and tension pneumoperitoneum[3]. We reported a fatal case of highpressure air compressor induced colonic perforation causing tension pneumoperitoneum, pneumomediastinum, and pneumothorax.
2. Case report
Informed consent was obtained from the relatives of the patient.A 35-year-old male was sent to our emergency department with an alleged history of directing high pressure compressed air jet (Figure 1)towards the anus while playing practical jokes with his colleague in a rice mill industry.
He presented with complaints of severe dyspnea and abdominal distension. He was drowsy, tachypneic with room air saturation of 35% (normal value: >94%). His pulse rate was 113/min with cold extremities and blood pressure was 70/40 mm Hg (normal value:120/80 mm Hg). There was diffuse subcutaneous emphysema over the neck, chest, abdomen, and extremities. The abdomen was grossly distended, tense, rigid, not moving with respiration, and with hyper resonant on percussion. Multiple lacerations were found in perianal region with a lax anal tone. His blood gases were pH=7.0 (normal value: 7.35-7.45), pCO2=77.5 (normal value: 35-45), HCO3=11.7(normal value: 22-26), PaO2=54 (normal value: 75-100), lactate=6.2(normal value: <2). In view of type 2 respiratory failure, emergency intubation was done with a 7.5 mm ET tube after pre-medicating with fentanyl 100 mg IV and ketamine 100 mg IV. Crystalloids were rushed using two wide bore intravenous cannula. Point-ofcare ultrasound was suboptimal due to subcutaneous emphysema.In view of tension pneumoperitoneum, urgent percutaneous needle decompression was performed using 16 G needle, 5 cm superomedial to the anterior superior iliac spine. The gush of air was released along with reduction in abdominal distension and improvement in his blood pressure to 110/70 mmHg.
Contrast enchanced CT abdomen revealed pneumoperitoneum,pneumopericardium, and left-sided pneumothorax (Figure 2).A left-sided intercostal chest drain was inserted in view of pneumopericardium communicating with left pleural cavity. On emergency exploratory laparotomy, gush of air was released on opening peritoneum, and findings were 1 L of hemoperitoneum,grossly distended small bowel, multiple lacerations with serosal tears, and full-thickness 12 cm perforation in the sigmoid colon.Resection of perforated sigmoid with recto-descending colon anastomosis and transverse loop colostomy was done.Post-operation, he was admitted to the intensive care unit on double inotropic support. But he succumbed two days later due to septic shock.

Figure 1. High pressure compressed air jet equipment.
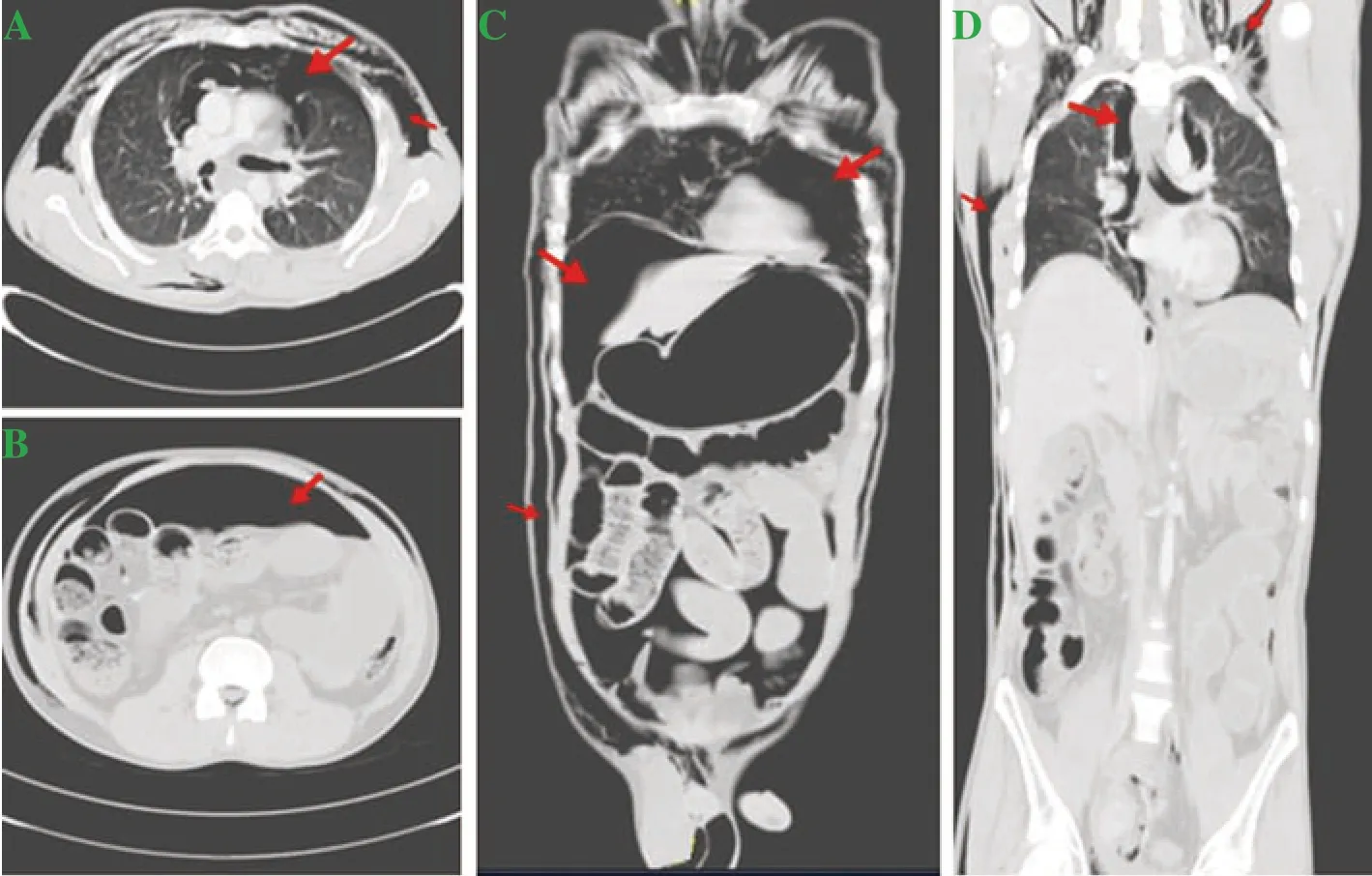
Figure 2. Contrast enchanced CT abdomen reveals pneumoperitoneum, pneumopericardium, and left-sided pneumothorax. A&B: Transverse section shows pneumoperitoneum, pneumopericardium, and left pneumothorax (red arrow). C&D: Coronal section shows air under the diaphragm with pneumopericardium,pneumothorax and extensive subcutaneous emphysema (red arrow).
3. Discussion
The first case report of pneumatic colon injury was mentioned by Stone[4] in 1904 and reviewed by Brownet al.[5] in 1942.Burt[6] investigated the relationship between air pressure and intestinal rupture in 1931. The study had revealed that mucosa was the strongest of the four layers of the intestinal wall, and when pressure was increased progressively, the muscle and serosa ripped apart first, followed by the mucosa. It was also postulated that pressure of 3.99 psi could tear the muscle and serosa, and 4.07 psi could rupture the entire thickness of the intestinal wall and create a perforation. In compressed air equipment, the usual pressure used is 100-213 psi which is 10-30 times greater than the pressure required to perforate intestine. In our case, the machine could exert pressure from 128 to 170 psi.
The majority of perforations occurred in the rectosigmoid junction while the ascending colon, hepatic flexure, and transverse colon are less injured parts. Injury to the small intestine due to compressed air has been rarely reported. The anatomical configuration of the buttock and perineum is like a funnel, allowing easy delivery of compressed air into the anal orifice. Clothes do not alter the effect of compressed air. As the anal canal and descending rectum is well supported by outside structure. The anti-mesenteric border of the rectosigmoid is the first part of colon strike by column of compressed air and hence is the most common site of perforation[7].
Clinical manifestation depends upon the extent of intraluminal pressure that causes colonic perforation and leads to tension pneumoperitoneum. Tension pneumoperitoneum compresses the vena cava, decreases venous return to the heart, and induces hypotension and circulatory collapse[8]. Colonic perforation can occur at single or multiple sites[5]. Abdominal pain and distension develop rapidly if colon perforation occurs, and peritoneal irritational sign will also be presented. Frequently,respiratory distress can be seen because pneumoperitoneum can reduce diaphragmatic movements. Hyperventilation could result in mild to moderate respiratory alkalosis. Higher pressure within the peritoneal cavity may lead to subsequent migration of air through the oesophageal hiatus resulting in pneumomediastinum,pneumothorax, and extensive subcutaneous emphysema[9].
Abdominal paracentesis using a needle or trocar is a simple, useful technique to reduce respiratory distress. For hemodynamically unstable patients, immediate abdominal decompression is highly recommended. It may not adequately relieve the tension of pneumoperitoneum but may help reduce the pressure to some extent to prevent abdominal compartment syndrome. It is a temporary time-buying measure to improve the patient’s ventilatory capability and hemodynamics as the patient is getting transferred to definitive surgical treatment. The sites of abdominal wall recommended for needle decompression are (1) Two centimeters below the umbilicus at midline (vialinea alba), after bladder catheterization; (2) Five centimeters superomedial to the anterior superior iliac spine on either side. The decompression should immediately be followed by surgical exploration at the operation theatre. After recovery from the initial stock, peritonitis due to faecal contents of the peritoneal cavity should be treated immediately. With modern treatment and antibiotics, diffuse peritonitis carries mortality of about 10%.Tension pneumoperitoneum is a rare presentation of colonic barotrauma and has a high mortality rate of about 65%.
In conclusion, colonic injury due to pressurized air is a unique pathology that is now being reported increasingly with the extensive use of compressed air in this industrial era. This condition must be taken seriously because its consequences could be devastating. This case underlines the necessity of educating and spreading awareness among industrial workers who handle such dangerous compressed air devices at their workplaces.
Conflict of interest statement
The authors report no conflict of interest.
Authors’ contributions
S.R.: Manuscript preparation; A.D.: Manuscript editing, manuscript review; D.K.: Clinical management; N.K.M.: Manuscript preparation manuscript editing, manuscript review; K.N.J.P.R.: Manuscript editing, manuscript review.
 Journal of Acute Disease2020年6期
Journal of Acute Disease2020年6期
- Journal of Acute Disease的其它文章
- Acute ascites as a clinical manifestation of dengue: A case report
- Risk factors of COVID-19 infection among policemen: A case-control study
- Risk factors of Clostridium difficile infection in ICU patients with hospital-acquired diarrhea: A case-control study
- Clinical features, management and outcomes of pediatric pleural empyema: A retrospective, multicenter cross sectional study
- A scoping review of vestibular paroxysmia: An acute disabling clinical entity
- Expert consensus on emergency diagnosis and treatment procedures for acute upper gastrointestinal bleeding