
老年人工关节置换术患者术后谵妄的影响因素
2020-08-27 12:58李敏刘娣程向阳
中国医药导报 2020年19期
李敏 刘娣 程向阳
[摘要] 目的 研究老年人工關节置换术患者术后谵妄的影响因素,为有效防治老年患者术后谵妄提供依据。方法 选取蚌埠医学院第一附属医院骨科2018年10月~2019年8月收治的151例人工关节置换术患者作为研究对象。术前采用衰弱量表测定患者衰弱程度,记录患者年龄、性别、焦虑评分(APAIS)、Charlson共病指数(CCI)、日常生活活动能力评分(ADL)、白蛋白水平、美国麻醉学会分级(ASA)等一般资料。根据谵妄量表(CAMCR)筛选出发生术后谵妄的患者,将患者分为谵妄组和非谵妄组,分析术后谵妄影响因素。 结果 谵妄组共37例,非谵妄组共114例。术后谵妄的发生率为24.5%。与非谵妄组比较,谵妄组年龄较大、术前焦虑评分较高、Charlson评分较高、ADL评分较低、术前衰弱人数较多,差异均有统计学意义(均P < 0.05)。二元回归分析显示术前衰弱、焦虑、并存多种疾病、日常活动能力下降是术后谵妄发生的独立影响因素(P < 0.05)。 结论 衰弱、焦虑、并存多种疾病及日常活动能力下降,是老年人工关节置换术患者术后谵妄的独立影响因素。
[关键词] 人工关节置换术;老年患者;术后谵妄;衰弱;危险因素
[中图分类号] R687.4 [文献标识码] A [文章编号] 1673-7210(2020)07(a)-0082-04
[Abstract] Objective To study the influence factors of postoperative delirium in olderly patients with artificial joint replacement, so as to provide basis for effective prevention and treatment of postoperative delirium in elderly patients. Methods A total of 151 cases of artificial joint replacement patients undergoing prosthetic replacement surgery at the Department of Orthopedics of the First Affiliated Hospital of Bengbu Medical College from October 2018 to August 2019 were selected as the subjects. The frailty scale was used to measure the frailty of the patients before surgery, and the age, sex, anxiety score (APAIS), Charlson comorbidities index (CCI), daily activity score (ADL), albumin level, American Society of Anesthesiology grading (ASA) and other general data were recorded. Patients with postoperative delirium were screened out according to delirium scale (CAMCR). The patients were divided into the postoperative delirium group and the non-postoperative delirium group, and risk factors of postoperative delirium were analyzed. Results There were 37 cases in the postoperative delirium group and 114 cases in the non-postoperative delirium group. The incidence of postoperative delirium was 24.5%. Compared with the non-postoperative delirium group, the postoperative delirium group was older, the preoperative anxiety score was higher, the Charlson score was higher, the ADL score was lower, and the numbers of debilitating was more, the differences were statistically significant (all P < 0.05). Binary regression analysis showed that weakness, anxiety, co-existence of various diseases and decreased ability of daily activities were independent risk factors for postoperative delirium (P < 0.05). Conclusion Frailty, anxiety, comorbidities and decreased ability of daily activities are independent influence factors for postoperative delirium in elderly patients undergoing artificial joint replacement.
[Key words] Orthopaedic surgery; Elderly patients; Postoperative delirium; Frailty; Influence factors
骨科手术经常发生严重的外科和医疗并发症。术后谵妄(postoperative delirium,POD)是骨科手术患者最常见的并发症之一[1]。POD是指患者在经历外科手术后24~72 h出现的意识、注意力和认知功能的急性紊乱,是常见的老年患者术后并发症[2]。临床医生如不及时恰当地处理,将增加患者的住院时间,导致持续性的认知功能障碍,甚至导致永久性脑损害、痴呆或死亡[3]。本研究通过对151例老年髋关节或膝关节置换术患者的临床资料进行分析,探讨与POD相关的影响因素,为针对性地采用干预措施,降低POD的发生率提供依据,对促进老年患者快速康复具有重要的临床价值。
1 对象与方法
1.1 研究对象
经蚌埠医学院第一附属医院(以下简称“我院”)医学伦理委员会批准,选取我院关节骨科2018年10月~2019年8月,老年择期髋关节或膝关节单侧置换术的患者151例,男44例,女107例;年龄65~87岁,平均(71.47±5.63)岁;行单侧髋关节置换术59例,单侧膝关节置换术92例;ASAⅡ~Ⅲ级,其中Ⅱ级89例,Ⅲ级62例。
纳入标准:①年龄≥65岁;②老年择期髋关节或膝关节置换术;③患者及家属知情同意。
排除标准:①术前简易心智状态问卷调查表(SPMSQ)[4]诊断认知障碍者;②术前谵妄量表(CAMCR)[5]诊断为谵妄者;③语言交流障碍,无法完成认知功能测试。
1.2 方法
1.2.1 一般资料 患者的一般资料主要包括年龄、性别、体重指数(BMI)、APAIS焦虑评分(APAIS)[6]、Charlson共病指数(CCI)[7]、日常生活活动能力(ADL)评分[8]、白蛋白水平、ASA分级等资料。CCI评分越高提示患者并存疾病越严重。
1.2.2 衰弱评估 采用FRAIL量表[9]进行衰弱评分。包括5项:①疲劳感;②阻力感:上1层楼梯即感困难;③自由活动下降:不能行走1个街区;④多种疾病共存:≥5个;⑤体重减轻:1年内体重下降>5.0%。其中0~1分为无衰弱;2~3分为轻度衰弱;>3分为衰弱。
1.2.3 POD评估 术后1~3 d应用CAMCR量表评估POD的发生情况,根据患者是否急性起病、注意力、思维、定向力、意识、记忆力、知觉、精神状态、睡眠-觉醒周期等进行评分,评分>19分即诊断为POD。
1.3 统计学方法
采用SPSS 19.0软件对所得数据进行分析。计量资料满足正态分布则采用均数±标准差(x±s)表示,组间比较采用t检验,不符合正态分布则采用[M(P25,P75)]表示,组间比较采用秩和检验;计数资料采用百分率表示,组间比较采用χ2检验;将所得资料进行单因素分析后P < 0.1所对应的因素纳入二元 logistic回归分析筛选出独立的危险因素。以P < 0.05为差异有统计学意义。
2 结果
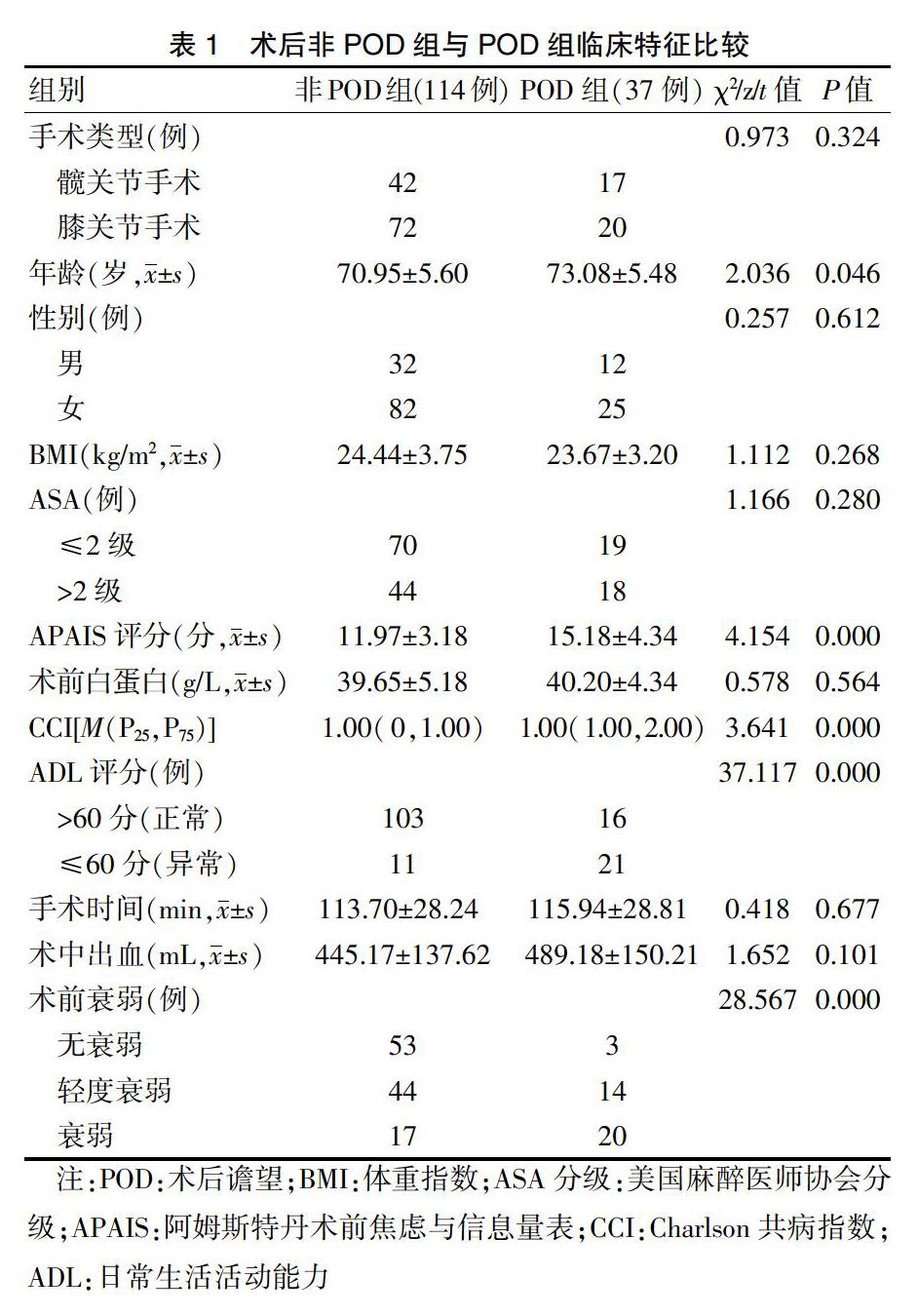
2.1术后非POD组与POD组临床特征比较
151例骨科老年手术患者临床资料,根据CAMCR筛选出发生术后POD的患者,将患者分为POD组(37例)和非POD组(114例),术后POD的发生率为24.5%。与非POD组比较,POD组年龄较大、APAIS评分较高、CCI较高、ADL评分较低、术前衰弱人数较多,差异均有统计学意义(均P < 0.05)。见表1。
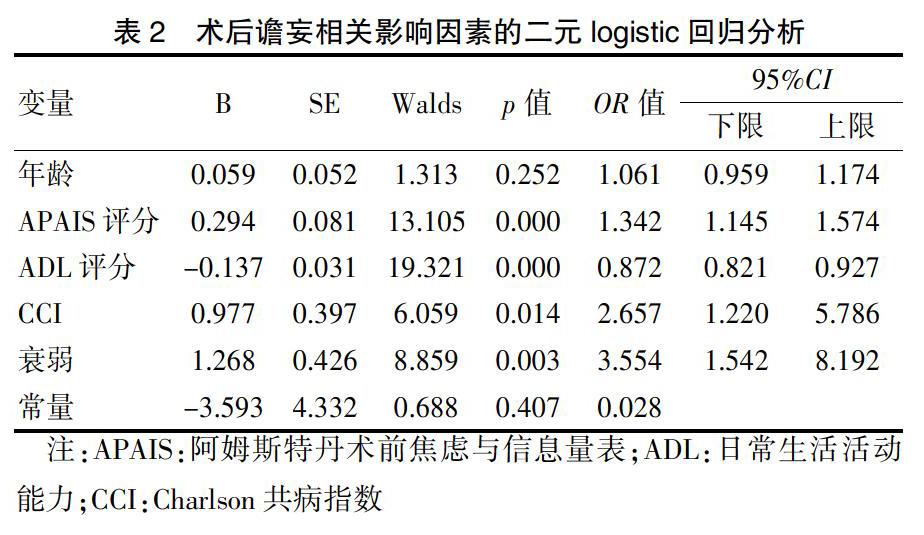
2.2 二元logistic回归分析
将单因素分析中P < 0.1的相关因素作为自变量(其中赋值:无衰弱=1,轻度衰弱=2,衰弱=3),是否发生POD为因变量(赋值:术后非POD=0,术后POD=1),进行二元logistic 回归分析。结果显示术前衰弱、APAIS焦虑评分、CCI、ADL评分可以独立预测POD的发生,差异均有统计学意义(均P < 0.05)。见表2。
3 讨论
POD是骨科患者术后最严重的并发症之一,它会导致患者出院延迟,医疗费用增加,同时增加坠落、创伤、意外拔管等并发症的发生风险。成功的干预措施可显著降低POD的发生率,因而靶向干预有发生POD风险的患者尤为重要。然而目前POD发生的影响因素仍不明确,可能由多种影响因素共同作用。这些影响因素常见的有认知功能下降、痴呆、脑卒中、术前营养不良等[10]。本研究着重探讨术前及术中可能影响POD的影响因素。本研究发现老年人工关节置换术患者POD的发生率为24.50%,与Scholtens等[11]的研究结果一致。然而,Bruce等[12]指出髋部骨折手术患者的POD发生率为4.0%~53.3%。笔者认为不同诊断标准及评分量表的采用、评估时段不同(可能遗漏病例)、手术及麻醉技术、围术期护理等都是造成这种差异的原因。
近年来,衰弱在外科患者中的重要性引起人们的广泛关注。老年人的神经系统、心血管系统等可产生功能退变和失调,引发衰弱综合征,增加跌倒、残疾、患病和死亡等风险,更易出现术后不良结局[13-14]。衰弱评估是衡量机体整体的功能储备,可以作为多系统疾病的筛查工具。研究发现老年人衰弱与术后并发症密切相关[15-17],而衰弱是否是POD的风险因素鲜有报道。本研究采用FRAIL量表评估老年人工关节置换术患者术前衰弱,发现术前衰弱与POD的发生存在显著相关性。相关学者发现[18]患有阿尔茨海默病的患者在死亡前表現为衰弱,提出衰弱可能是痴呆的前兆。炎性因子标志物C-反应蛋白或者白细胞介素与衰弱和认知损伤有关[19-20]。衰弱和POD可能有一个共同的病因。
此外,POD發生时的心理因素尚未得到充分考虑。入院患者在经历身体疾病、疼痛、噪音和身处病房等都会有一定程度的心理压力[21]。Park等[22]研究发现术前焦虑会导致更多的术后并发症,患者的恢复期延长和住院时间增加。本研究术前对患者采用APAIS焦虑量表评估患者焦虑程度,发现术前焦虑是POD独立的风险因素。焦虑可能与氧化应激、神经递质的丢失有关,与POD的发生机制相同[23]。可见术前及时适当的心理安慰,减轻患者的心理压力对降低POD的发生极为重要。对于老年患者,并存疾病及日常活动耐量也是不可忽视的因素。并存疾病往往提示多个器官系统受累或存在代谢紊乱,可导致POD风险增加[24]。ADL评分为功能状态的评估,反映患者的日常生活能力和生活质量。术前存在活动耐量降低,生理功能下降足以导致POD的发生。术前加强功能锻炼,提高生活自理水平可以降低术后POD的发生风险。
本研究仅针对老年人工关节置换手术的患者,而外科系统病种复杂,研究结果不能反映整个外科手术患者的术后POD。同时,样本量的大小也是本研究的局限所在,尚需大样本研究证实。FRAIL量表、APAIS焦虑量表等具有主观性,不同的评估人员可能得到不同的评分,联合其他量表评估更能提高准确性。
综上所述,术前衰弱、焦虑、多种疾病并存、日常活动能力下降是老年人工关节置换术患者POD发生的独立影响因素。术前系统地实施老年综合评估,针对高风险患者进行干预包括术前调整全身状况、运动锻炼、营养支持、优化他们的身体机能、心理治疗减轻患者的焦虑等意义重大。
[参考文献]
[1] Merchant RA,Lui KL,Ismail NH,et al. The relationship between postoperative complications and outcomes after hip fracture surgery [J]. Ann Acad Med Singapore,2005,34(2):163-168.
[2] Robinson TN,Raeburn CD,Tran ZV,et al. Postoperative delirium in the elderly [J]. Ann Surg,2009,249:173-178.
[3] 刘丹,王东信.危重患者术后谵妄对远期生存率的影响[J].重庆医学,2015,44(9):1229-1231.
[4] Pfeiffer E. A short portable mental status questionnaire for the assessment of organic brain deficit in elderly patients [J]. J Am Geriatr Soc,1975,23(10):433-441.
[5] Inouye SK,van Dyck CH,Alessi CA,et al. Clarifying confusion:the confusion assessment method. A new method for detection of delirium [J]. Ann Intern Med,1990,113(12):941-948.
[6] Moerman N,van Dam FS,Muller MJ,et al. The Amsterdam preoperative anxiety and information scale (APAIS)[J]. Anesth Analg,1996,82(3):445-451.
[7] Roffman CE,Buchanan J,Allison GT. Charlson Comorbidities Index [J]. J Physiother,2016,62(3):171.
[8] Mahoney FI,Barthel DW. Functional evaluation:the Barthel index [J]. Md State Med J,1965(14):61-65.
[9] Morley JE,Malmstrom TK. A simple frailty questionnaire (FRAIL) predicts outcomes in middle aged African Americans [J]. J Nutr Health Aging,2012,16(7):601-608.
[10] Reddy SV,Irkal JN,Srinivasamurthy A,et al. Postoperative delirium in elderly citizens and current practice [J]. J Anaesthesiol Clin Pharmacol,2017,33(3):291-299.
[11] Scholtens RM,de Rooij SE,Vellekoop AE,et al. Preoperative CSF Melatonin Concentrations and the Occurrence of Delirium in Older Hip Fracture Patients:A Preliminary Study [J]. PLoS One,2016,11(12):1-11.
[12] Bruce AJ,Ritchie CW,Blizard R,et al. The incidence of delirium associated with orthopedic surgery:a meta-analytic review [J]. Int Psychogeriatr,2007,19(2):197-214.
[13] 宋維,王家杰,刘佳文.老年衰弱综合征的研究[J].脑与神经疾病杂志,2018,26(9):579-582.
[14] 施红.老年人衰弱综合征[J].中华老年病研究电子杂志,2016,3(3):11-15.
[15] Charles H Brown 4th,Laura Max,Andrew Laflam,et al. The Association Between Preoperative Frailty and Postoperative Delirium After Cardiac Surgery[J]. Anesth,Analg,2016,123(2):340-435.
[16] 张文,刘殿刚,吕建阳,等.衰弱评分与老年患者行经尿道前列腺电切术围手术期并发发生率关系的研究[J].临床和实验医学杂志,2015,14(11):895-898.
[17] Gleason LJ,Benton EA,Alvarez-Nebreda ML,et al. FRAIL Questionnaire Screening Tool and Short-Term Outcomes in Geriatric Fracture Patients [J]. J Am Med Dir Assoc 2017,18(12):1082-1086.
[18] Buchman AS,Schneider JA,Leurgans S. Physical frailty in older persons is associated with Alzheimer disease pathology [J]. Neurology,2008,71(7):499-504.
[19] Puts MT,Visser M,Twisk JW,et al. Endocrine and inflammatory markers as predictors of frailty [J]. Clin Endocrinol(Oxf),2005,63(4):403-411.
[20] Weaver JD,Huang MH,Albert M,et al. Interleukin-6 and risk of cognitive decline:MacArthur studies of successful aging [J]. Neurology,2002,59(3):371-378.
[21] MacLullich AM. Who understands delirium? [J]. Age Ageing,2011,40(4):412-414.
[22] Park S,Chang HK,Hwang Y,et al. Risk factors for postoperative anxiety and depression after surgical treatment for lung cancer [J]. Eur J Cardiothorac Surg,2015,49(1):16-21.
[23] Black CN,Bot M,Scheffer PG. Oxidative stress in major depressive and anxiety disorders,and the association with antidepressant use; results from a large adult cohort [J]. Psychol Med,2017,47(5):936-948.
[24] Raats JW,Steunenberg SL,de Lange DC. Risk factors of post-operative delirium after elective vascular surgery in the elderly:A systematic review [J]. Int J Surg,2016,35:1-6.
(收稿日期:2020-01-02)
猜你喜欢
中国现代医生(2016年25期)2016-11-19
科技资讯(2016年19期)2016-11-15
中国实用医药(2016年24期)2016-10-17
养生保健指南(2016年4期)2016-03-22
养生保健指南(2016年4期)2016-03-22
