
Development of Primary Percutaneous Coronary Intervention as a National Reperfusion Strategy for Patients with ST-Elevation Myocardial Infarction and Assessment of Its Use in Egypt
2020-07-30 13:59MohamedSobhyMDPhDAhmedElshalMDNohaGhanemMVScPhDHosamHasanAliMDPhDNabilFaragMDPhDNireenOkashaMDPhDElSayedFaragMDPhDMohamedSadakaMDPhDHishamAboElEneinMDPhDSamehSalamaMDPhDHazemKhamisMDPhDKhaledShokryMDPhDHa
Mohamed Sobhy,MD,PhD ,Ahmed Elshal,MD ,Noha Ghanem,MVSc,PhD ,Hosam Hasan-Ali,MD,PhD ,Nabil Farag,MD,PhD ,Nireen Okasha,MD,PhD ,El Sayed Farag,MD,PhD ,Mohamed Sadaka,MD,PhD ,Hisham Abo El Enein,MD,PhD ,Sameh Salama,MD,PhD ,Hazem Khamis,MD,PhD ,Khaled Shokry,MD,PhD 0,Hany Ragy,MD,PhD ,Amany Elshorbagy,MD,PhD and Radwa Mehanna,MD,PhD
1 Cardiology Department,Faculty of Medicine,Alexandria University Hospital,Alexandria,Egypt
2 International Center for Organization and Marketing,Alexandria,Egypt
3 Cardiology Department,Faculty of Medicine Assiut University Hospital,Assiut Governorate,Egypt
4 Cardiology Department,Faculty of Medicine Ain Shams University Hospital,Heliopolis,Egypt
5 Cardiology Department,Nasser Institute,Cairo,Egypt
6 Cardiology Department,Faculty of Medicine,Zagazig University Hospital,Zagazig,Egypt
7 Cardiology Department,Faculty of Medicine,Banha University Hospital,Banha,Egypt
8 Cardiology Department,Faculty of Medicine,Kasr El Ainy Hospital,Kasr Al Ainy,Egypt
9 Cardiology Department,Wady El Nile Hospital,Zeitoun,Egypt
10 Cardiology Department,Military Hospital,Heliopolis,Cairo,Egypt
11 Cardiology Department,National Heart Institute,Heliopolis,Cairo,Egypt
12 Physiology Department,Faculty of Medicine,Alexandria University,Alexandria,Egypt
Abstract
Keywords:ST-elevation myocardial infarction;primary percutaneous coronary intervention;door to balloon time;f irst medical contact to balloon time
Introduction
Primary percutaneous coronary intervention (PCI) is a lifesaving treatment for acute coronary syndromes,particularly ST-elevation myocardial infarction (STEMI).It is used to reopen blocked arteries and thus restore blood flow to the heart [1].In many patients a stent is inserted into the artery during primary PCI to reduce the chance of the dangerous blockage recurring.There is indisputable scientific evidence that myocardial revascularization in patients with acute forms of coronary artery disease reduces mortality,the recurrence of heart attack,and risk of stroke as compared with the previous standard therapies (pharmacological treatment,including thrombolytic therapy for STEMI) [2].Initiating this treatment rapidly - ideally within 2 hours of an STEMI - is key to preventing long-term damage to the heart [3].Patient access to PCI differs considerably between European countries,ranging from around 5 to 92% [4].The accessibility of STEMI patients in Egypt to this lifesaving treatment is not yet known.Additionally,the lack of organized primary PCI networks means fewer patients overall receive some form of reperfusion therapy,which results in poor prognosis.
Registry studies and surveys have been conducted in Egypt for STEMI and non-STEMI patients [5],but a description of the whole process,including the onset of acute episodes,the consequent changes in clinical conditions,and the management strategies,is not available.A survey able to capture all the relevant clinical information regarding patients with STEMI,including the attack onset,symptoms,and time and strategy of management,together with the full medical history of the patient,would enable us to improve our knowledge of the risks,burdens,obstacles,and outcomes regarding real-world patients with this clinical condition.
This study aims to identify the mean time to primary PCI (door to balloon time) for STEMI patients and thus assess the percentage of primary PCI for STEMI patients and its success rate in Egypt.It also aims to evaluate different patterns of treatment for STEMI patients by the assessment of treatment modality rates for thrombolytic therapy or PCI (balloon dilation and/or stenting).Further objectives include the evaluation of the organization of primary PCI management across Egypt and how the recommendations of the most recent European guidelines regarding pharmacological and nonpharmacological treatments are adopted in clinical practice,and finally to what extent their application can impact patient outcomes.
Method
Observational Study
A long-term prospective,cross-sectional,multicenter registry study of patients presenting to cardiac centers in Egypt was designed.The registry study was conducted at eight governorates in Egypt,and included 17 centers/hospitals:eight public hospitals,eight university hospitals,and one nongovernmental organization.
Standard treatment of patients was by the diagnostic and therapeutic interventions routinely performed in each center for patients presenting with signs and symptoms of myocardial infarction.Drug prescriptions and indications to perform diagnostic/therapeutic procedures were left to the participating cardiologist’ s decision.No specific protocols or recommendations for evaluation,management,and/or treatment were proposed during this observational study.
The inclusion criteria for enrolled patients were as follows:patients with diagnosed myocardial infarction,according to the clinical judgment of the participating centers’ responsible cardiologist,either with ST elevation or without ST elevation,admitted to the catheterization laboratory or not admitted,treated with thrombolytic therapy or by intervention,or admitted for an acute episode in the participating center during the enrollment period.The only exclusion criterion was age younger than 18 years.
Patients were free to withdraw from the study at any time without giving a reason.Patients were advised if they requested to withdraw from the study,at any time during the trial,then this would have no negative consequences.
Because the study was fully observational,a formal sample size was not calculated.However,a sample of 1000 enrolled patients was estimated as the minimum number to fulfill the level of quality for assessment at a national level.
Site and Patient Selection
Selection of each participating city or governorate was done by our targeting a sample of hospitals of different levels of complexity from which patients were recruited according to the inclusion criteria and exclusion criterion focusing on capturing a broad spectrum of myocardial infarction patients so as to build up a network of centers representing the Egyptian reality.
The Clinical Research Form
The clinical research form (CRF) (supplementary data) was created by the scientific committee and given to the participating centers as an electronic version with login username and password for each participating center/hospital.The CRF was completed with use of the original hospital documents for each patient and which included the diagnosis,investigations,and treatment strategies.It also included the “ door to balloon time” and the “ first medical contact to balloon time,” where “ door” corresponds to the admission time and “ balloon” merged variables,including the time of admission to the catheterization laboratory,admission for primary PCI to catherization laboratory time,and the time of coronary balloon angioplasty.
Follow-up
A follow-up visit by the patients 3,6,and 9 months after the initial admission was arranged to collect information on morbidity and mortality.If it was impossible for the patient to reach the clinical center for logistic reasons,the follow-up clinical visit was replaced by a phone call.
Ethics Approval and Consent
The study was performed in compliance with the requirements of the Ethics Committee of the Faculty of Medicine of Alexandria University.Full regulatory approval was granted under IRB number 00007555-FWA NO:00015712.
All patients provided written informed consent to participate in the study before being recruited.The patient information sheet detailed the aims,method,potential risks,and anticipated benefits of the study,and these were further explained by an investigator.The patient signed the consent form to indicate that the information had been explained and understood.The patient was given a copy of the informed consent form for information.The original copy of the informed consent form was kept in a confidential file in the investigators’ center.
Training and Education
Educational meetings were conducted with the investigators involved in the registry study to update the guidelines and training on the CRF data entry,after which a consent form was signed by each center approving its participation according to the given terms and conditions.Usernames and passwords were sent confidentially to each center to start the enrollment.Meetings between key decision makers throughout Egypt (e.g.,leading interventional cardiologists,Minister of Health,ambulance service managers,medical device and pharmaceutical companies,and the telecommunication industry) were held to support the execution of the registry study.
Auditing Process
Periodically,the participating centers were selected for monitoring on the basis of the risk strategy (e.g.,number of patients enrolled,high number of data management queries) through onsite visits,which were performed by trained monitors.Confirmation of the accuracy of filling in the CRF in comparison with the original documents for randomly selected patients and verification of the signed informed consent forms was carried out.
Variables and Evaluation Criteria
Data were evaluated as follows:population characteristics (total population);population characteristics by sex;patient distribution;treatment strategy (total population);treatment strategy by sex;treatment strategy by year;success rate (complete revascularization) according to the strategy.
Safety Evaluation
Adverse Events
Any adverse event observed as a result of the therapeutic strategy used (interventional or medical) was recorded in the CRF.
Serious Adverse Events and Other Significant Adverse Events
A document for serious adverse events was created and given to all centers to be f illed in and submitted within 24 hours of their appearance.
Pharmacovigilance
Drug safety was monitored by recording adverse drug reactions in the follow-up period.Serious adverse events were to be recorded anytime in the follow-up period.
Statistical Analysis
Results were compared with use of the chi square test or Fisher’ s exact test as appropriate for categorical variables and the Mann-WhitneyUtest or independent samplesttest for continuous variables as appropriate.P > 0.05 was considered significant.
Results
The registry period was 40 months,including the follow-up period.Seventeen centers/hospitals in eight governorates participated,and the total number of patients enrolled was 1661,of which 1650 patients were analyzed;the remaining 11 patients did not have STEMI and were thus excluded from the study.Patients who missed their follow-up visit dates by 1 week were contacted by telephone.
Patient Distribution and Types of Hospitals/Centers Involved in the Study
The centers and hospitals that participated in the study were either public or private with a catheterization laboratory working 24 hours for the whole week,a catheterization laboratory not working 24 hours per day or not working for the whole week,or no catheterization laboratory.The number and percentage of patients admitted to the centers and hospitals of the above-mentioned categories are given in Figure1 and in Table1 in the supplementary material.
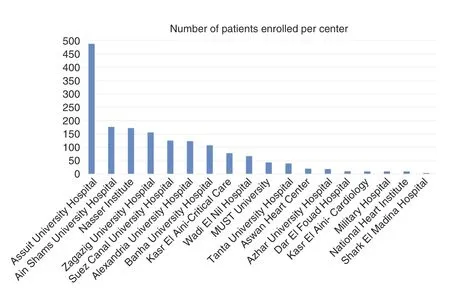
Figure1:Number of Patients Enrolled Per Center.

Table1 Treatment Strategy for Total Population.
Patient Data and Baseline Characteristics
In 2014,480 STEMI patients were enrolled,227 were enrolled in 2015,231 were enrolled in 2016,and 712 were enrolled in 2017.All numbers given were analyzed as no withdrawals occurred during the study.The age,risk factors,and family history of the patients are shown in Table2 in the supplementary material.
The median age of the men and women in the study was 56 and 60 years,respectively,showing no significant difference between the sexes.
Obesity,diabetes,hypertension,and hypercholesterolemia were evaluated as prognostic and risk factors,and it was found that the rates for women were significantly higher than those for men:54.8% of women were obese versus 33.4% of men;69.5% of women had diabetes versus 42.6% of men;67.7% of women had hypertension versus 47.8% of men;and 58.9% of women had hypercholesterolemia versus 42.1% of men.
On the other hand,the picture was reversed concerning smoking,where the proportion of nonsmoker men was significantly lower than that of nonsmoker women,being 17.4 and 79.7%,respectively.Also,the proportion of current smokers was significantly higher for men (74.9%) than for women (18.1%).A family history of coronary artery disease was more frequent in women (25.4%) than in men (20.4%):see Table3 in the supplementary material.
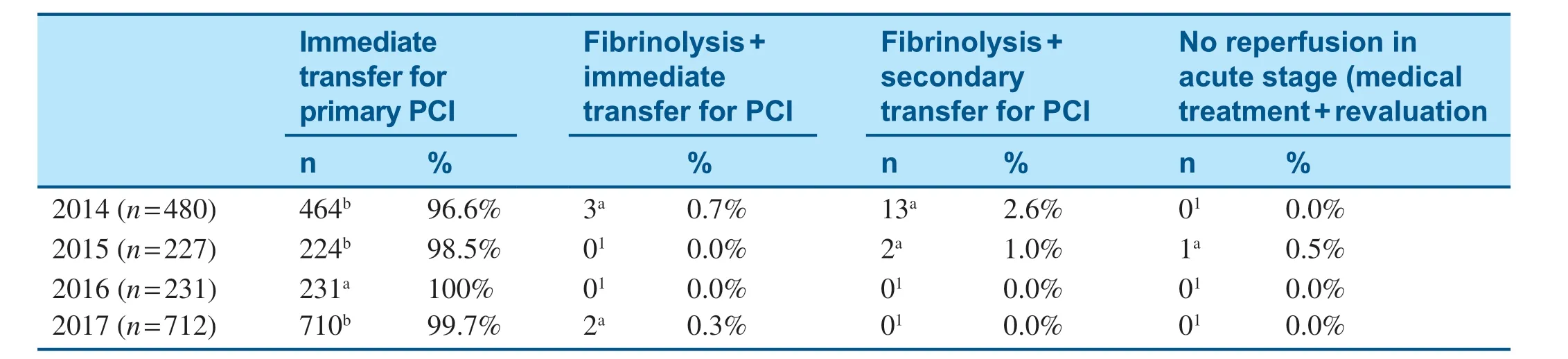
Table2 Treatment Strategy for Total Population Analyzed According to the Year.
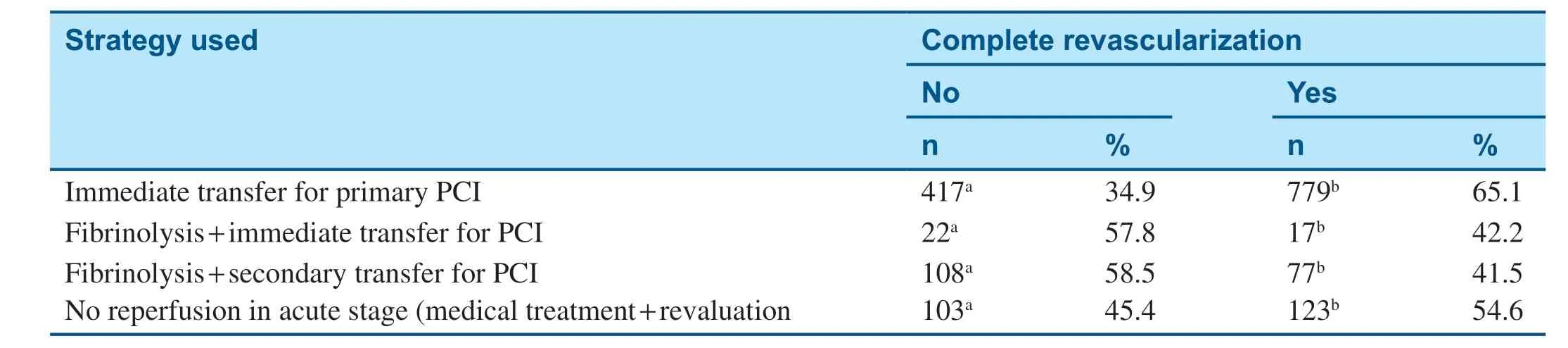
Table3 Rate of Treatment Success (Complete Revascularization) According to the Strategy.
Evaluated Data
No missing data were observed in the CRF as it was designed in a way that its submission will not be completed unless all fields have been filled in.
Treatment Strategies
Treatment Strategy for the Total Population
The number of patients who were immediately transferred for primary PCI was 1198 (72.6%),while 40 underwent fibrinolysis and immediate transfer for PCI (2.4%) and 186 underwent fibrinolysis and secondary transfer for PCI (11.3%).The number of patients for whom no reperfusion was performed in the acute stage but who instead were subjected to medical treatment and revaluation was 226 (13.7%);see Table1.
Treatment Strategies for the Total Population Analyzed according to Sex
The number of male and female patients who were immediately transferred for primary PCI was 921 (74.2%) and 275 (67.5%),respectively,while the number who underwent fibrinolysis and immediate transfer for PCI was 28.1 (2.3%) and 11 (2.6%),respectively,and the number who underwent fibrinolysis and secondary transfer for PCI was 127 (10.3%) and 58 (14.4%),respectively.The number of patients in whom no reperfusion was performed in the acute stage but who instead were subjected to medical treatment and revaluation was 162 (13.1%) and 64 (15.6%),respectively,where the number of men subjected to all treatment strategies mentioned was significantly higher than the number of women (P < 0.001) except for fibrinolysis + immediate transfer for PCI,for which there was no significant difference between the two sexes ( Figure2 and Table4 in the supplementary material).
Treatment Strategies for the Total Population Analyzed according to the Year
The number of patients in 2014,2015,2016,and 2017 who were immediately transferred for primary PCI was 464 (96.6%),224 (98.5%),231 (100%),and 710 (99.7%),respectively,while the number who underwent fibrinolysis and immediate transfer for PCI was 3 (0.7%),0 (0%),0 (0%),and 2 (0.3%),respectively,and the number who underwent fibrinolysis and secondary transfer for PCI was 13 (2.6%),2 (1%),0 (0%),and 0 (0%),respectively.The number of patients in whom no reperfusion was performed in the acute stage but who instead were subjected to medical treatment and revaluation was 0 (0%),1 (0.5%),0 (0%),and 0 (0%),respectively,where the strategy of immediate transfer for PCI was significantly more frequent than all other strategies through the 4 years of enrollment ( Table2).
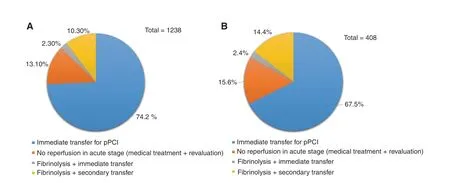
Figure2:Treatment Strategies:(A) for Men;(B) for Women.pPCI,Primary percutaneous coronary intervention.
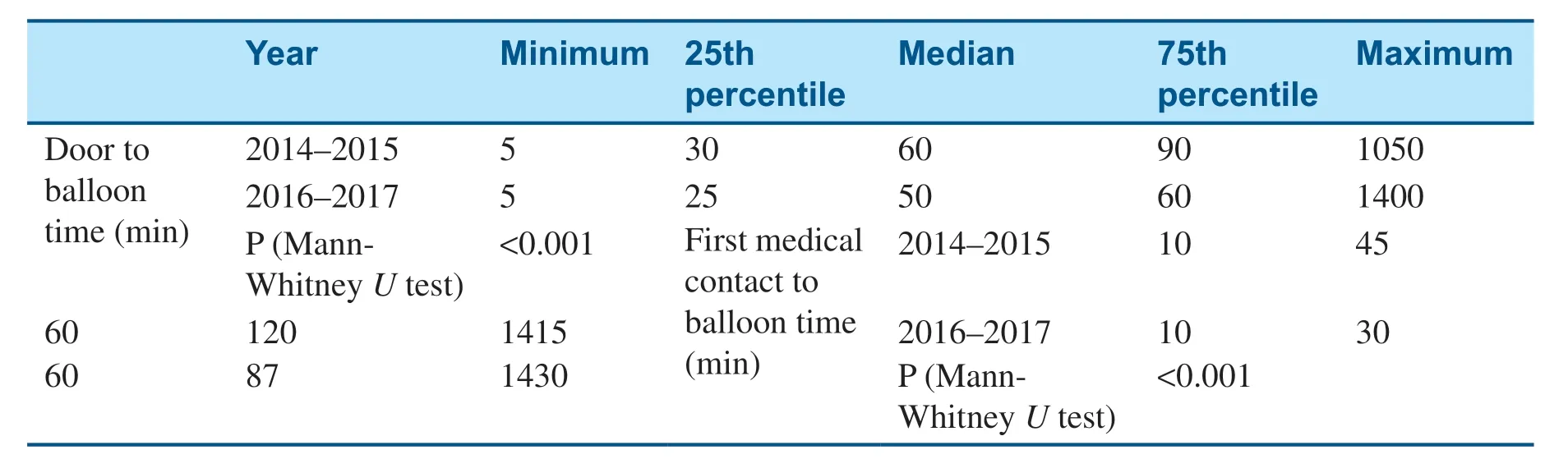
Table4 Door to Balloon Time and First Contact to Balloon Time for the Total Population.
Rate of Treatment Success (Complete Revascularization) According to the Strategy
The success of each treatment strategy was analyzed according to the occurrence of complete revascularization.The success rate of immediate transfer for primary PCI was 65.1% (779 patients) versus 34.9% (417 patients) where revascularization was not complete,while the success rate of fibrinolysis plus immediate transfer for PCI was 42.2% (17 patients) versus 57.8% (22 patients) and the success rate of fibrinolysis plus secondary transfer for PCI was 41.5% (77 patients) versus 58.5% (108 patients).The success rate for no reperfusion in the acute stage (medical treatment and revaluation) was 54.6% (123 patients) versus 45.4% (103 patients).The complete revascularization (success) rates were significantly higher for all strategies mentioned ( Table3).
Door to Balloon Time and First Contact to Balloon Time
Door to Balloon Time and First Contact to Balloon Time for the Total Population
The time was evaluated according to the minimum,25thpercentile,median,75thpercentile,and maximum time.Analysis of data was done according to the period 2014- 2015 versus 2016- 2017,which showed a highly significant decrease in the time taken from door to balloon and from first contact to balloon in 2016- 2017 compared with 2014- 2015 (P < 0.001).This result was mostly obvious for the 75thpercentile,where the door to balloon time was decreased from 90 minutes to 60 minutes and the first contact to balloon time was decreased from 120 minutes to 87 minutes in 75% of the enrolled population across the two periods analyzed ( Table4).
Door to Ballon Time and First Contact to Balloon Time according to Sex
The time was evaluated for men and women according to the minimum,25thpercentile,median,75thpercentile,and maximum time.
In men,the door to balloon time was 5.00,25.00,50.00,150.00,and 1425.00 minutes,respectively,while the first contact to balloon time was 5.00,45.00,70.00,240.00,and 1435.00 minutes,respectively.In women,the door to balloon time was 5.00,30.00,60.00,135.00,and 1410.00 minutes,respectively,while the first contact to balloon time was 5.00,45.00,65.00,260.00,and 1430.00 minutes,respectively.
There was no significant difference between the two sexes (Table5 in the supplementary material).
Mortality
Mortality was evaluated at the hospital and at 3,6,and 9 months.It was found that 2.8% of patients died in hospital and 4% had died at 3 months,0.5% had died at 6 months,and 0.6% had died at 9 months of follow-up (Table6 in the supplementary material).
Safety Evaluation
No adverse events were reported.No serious adverse events were reported,only errors in the electronic CRF submissions.
Discussion
Initiating appropriate treatment for STEMI patients rapidly - ideally within 2 hours of an STEMI - is key to preventing long-term damage to the heart.The study aimed to identify the mean time to primary PCI (door to balloon time and first medical contact to balloon time) for STEMI patients and to identify the percentage of primary PCI for STEMI patients and its success rate.
In our study the mean age of the STEMI patients was 57 years,which is lower than the mean age of STEMI patients in other studies published in developed countries,but is more or less equal to that of STEMI patients in studies published in developing countries.This could be attributed to the high prevalence of diabetes,dyslipidemia,obesity,and smoking in Egypt despite the public health effort done to limit tobacco use and control body weight.
We believe that the phrase “ every minute of delay counts” should be brought into perspective,so in our study we estimated the first medical contact to balloon time,which revealed that focusing on shortening the time to treatment from the first medical contact or the symptom onset and not only after the arrival of the patient at the hospital is a necessity.This was also recommended by other studies [6- 8]showing that each 30 minutes of delay from symptom onset is associated with a relative risk for death at 1 year.
The results of this study demonstrated a significant shortening of the time from the first contact with the patient by a medical service (first contact to balloon time) or the time from admission of the patient to a hospital until primary PCI (door to balloon time) in 2016- 2017 compared with 2014- 2015,which were included in this study and also in a similar study we conducted in 2011 concerning the Egyptian population [5].The median door to balloon time was 50 minutes in 2016- 2017 and 60 minutes in 2014- 2015 versus 70 minutes in 2011 as shown in the previous study [5],while the median first contact to balloon time was 60 minutes in 2016- 2017 and 2014- 2015 versus 320 minutes in 2011 [5].This improvement is believed to be attributed to the patient education campaigns held throughout the study period,which focused on raising patients’ awareness of the importance of the time between the first symptom they experience and seeking medical advice,and which was done through “ Meet the Experts” public sessions in all cardiology conferences held in Egypt,media campaigns such as radio and TV advertisements,and press releases and social media campaigns.Furthermore,continuous medical education of the investigators regarding the updated guidelines for managing these cases as well as the importance of immediate transfer of patients for primary PCI,where more than 35 satellite meetings were held for education of physicians with a total attendance of 3700 cardiologists.Paramedic training programs were also launched as well as several programs for the referral physicians.Our improved results were in accordance with De Luca et al.[6],whose results suggest that every minute of delay in primary angioplasty for STEMI affects 1-year mortality,even after adjustment for baseline characteristics.Furthermore,Terkelsen et al.[9],who evaluated the associations between system,treatment,patient,and door-to-balloon delays and mortality in patients with STEMI concluded that system delay was associated with mortality in patients with STEMI treated with primary PCI.In addition,the results reported by the American Heart Association Mission:Lifeline program (a long-standing STEMI improvement process initiative) revealed that the quality of care for patients with STEMI was improved over time because of increased use of reperfusion therapy and faster times to treatment [10].Therefore,all efforts should be made to shorten the total ischemic time,not only for thrombolytic therapy but also for primary angioplasty.
The statistical analysis of data in this study was based on the median,25thpercentile,and 75thpercentile of the population involved,which are better measures of variability reflecting a more valuable assessment of the results.In addition,the study also aimed to evaluate different patterns of treatment for STEMI patients and to assess rates of treatment by medical treatment,thrombolytic therapy,or PCI (balloon dilation and/or stenting).The results showed that different treatment strategies for STEMI patients were used,among which primary PCI was the strategy most often used,accounting for 72.6% of the total treatment strategies,followed by medical treatment then revaluation,with a rate of 13.7%,as well as thrombolytic treatment with PCI transfer,also with a rate of 13.7%.This was in accordance with the 2017 European Society of Cardiology guidelines for the management of STEMI,which state that STEMI patients should undergo primary PCI unless the anticipated absolute time from STEMI diagnosis to PCI-mediated reperfusion is more than 120 minutes,when fibrinolysis should be initiated immediately (i.e.,within 10 minutes of STEMI diagnosis).In our study,the success rate of complete revascularization resulting from primary PCI relative to other revascularization strategies was 65.1%.
It is worth mentioning that the percentage of primary PCI for STEMI patients enrolled during the study was 72.6% compared with 5% as previously reported for 2011 in Egypt [5].This result revealed a highly significant increase in use of this treatment strategy in Egypt within the appropriate time for rescuing STEMI patients and thus decreasing the morbidity rate and mortality associated with myocardial infarction.
Prognostic factors including age,comorbidities,the presence of diabetes,and previous myocardial infarction may result in differences in outcome beyond the stated objectives in this study.From the results we were also able to assess two important entries:firstly,the incidence of these prognostic factors,which are also considered as risk factors,including obesity,diabetes,hypertension,dyslipidemia and smoking,which could be further correlated to the occurrence of STEMI and to treatment modalities;secondly,the description of all results according to sex.
The sex difference was shown in several assessed entries,including the number of STEMI patients,which was significantly higher for men,while their age was significantly lower than that of women.In contrast,all prognostic/risk factors except smoking were significantly more frequent in women.
This study provides a database for the management of STEMI patients in Egypt,which can be used to compare its situation in relation to other countries and also build a future strategy for improving the treatment and prognosis of STEMI patients.International comparisons have demonstrated significant differences in infarct care organization and outcomes between countries,and national surveys have proven to be useful in improving the system and quality of care for STEMI patients [11,12].
The limitations of this study are believed to be in the generalization of the results across Egypt although the study included 17 centers/hospitals,but they were located in only eight governorates out of 27 in Egypt.More data need to be obtained from more areas across Egypt,but accessibility to rural regions might be an obstacle.
Conclusion
This registry provided a successful tool for assessing the present situation in Egypt regarding STEMI patients and also provided different methods for the improvement of implementing the best treatment strategy with respect to the time factor so as to give a better outcome for such patients.
From the registry study results we were able to assess the progress Egypt has achieved in the past few years concerning patient awareness,the application of guidelines,and the reduction in the causes of system delay when compared with the results of the pervious registry study in 2011 and which gives a better understanding of future plans for superior outcome.
Acknowledgement
The registry was financially supported by Sanofiwithout any influence on the process,data collection,data management,and/or the editorial process.
Conflict of Interest
The authors declare that they have no conflicts of interest.
 Cardiovascular Innovations and Applications2020年2期
Cardiovascular Innovations and Applications2020年2期
- Cardiovascular Innovations and Applications的其它文章
- Identification of Novel TTN Mutations in Three Chinese Familial Dilated Cardiomyopathy Pedigrees by Whole Exome Sequencing
- Association of Serum Chemerin Levels with Coronary Artery Disease:Pathogenesis and Clinical Research
- Discovery of Digenic Mutation,KCNH2 c.1898A > C and JUP c.916dupA,in a Chinese Family with Long QT Syndrome via Whole-Exome Sequencing
- The Accumulation of Visceral Fat and Preventive Measures among the Elderly
- Some Issues Related to STEMI and NSTEMI
- Chronic Effusive Pericarditis and Chronic Constrictive Pericarditis