Morphological changes of macular soft drusen and drusenoid DPED after subthreshold micropulse laser treatment
2020-06-08 00:24:08QingShanChenLuChenXiaZhao2MiaoHongChenYuHangYangZhiLi
国际眼科杂志 2020年6期
Qing-Shan Chen, Lu Chen, Xia Zhao2, Miao-Hong Chen, Yu-Hang Yang, Zhi Li
Abstract
•KEYWORDS:macular drusen; drusenoid pigmental epithulium detachment; subthreshold micropulse laser treatment; fundus autofluorescence
INTRODUCTION
Drusen is a kind of metabolite on the outer segment of photoreceptor between retinal pigmental epithulium (RPE) and Bruchs membrane[1], which acts as a biomarker of earlyage-related macular degeneration(AMD). Drusen is classified as hard drusen and soft drusen according to its diameter[2]. Soft drusen fusion can induce drusenoid retinal pigment epithelium detachment (DPED)[3]. DPED, also known as reticular pseudodrusen, is closely related to late geographic atrophy (GA) and choroidal neovascularization (CNV)-induced AMD[4]. Although some soft drusen and DPED may collapse or be absorbed naturally[5], AREDs studies showed that 36% of large soft drusen may develop to progressive AMD, 42% of DPED may develop to advanced AMD within 5y, and 55% of DPED may develop to focal geography atrophy[6-7]. Therefore, the treatment of soft drusen and DPED is beneficial to prevent the development of AMD and GA. Previous studies have shown that conventional retinal subthreshold photocoagulation was rarely used clinically due to the uncertain safety and efficacy in treatment of macular RPE[8-9]. Subthreshold micropulse laser treatment (SMLT) has been applied for the treatment of central serous chorioretinopathy (CSC) and DMEF in the macula subfoveal or parafoveal areas since it can regulate the RPE bioactive factors and RPE micro-damages, and remodel the intravascular barrier of RPE[10]. In this study, SMLT was adopted to treat the patients of soft drusen and DPED, and the results are as follows.
SUBJECTSANDMETHODS
SubjectsA retrospective, cross-sectional study was conducted. Fourteen patients (20 affected eyes), who were clinically confirmed in the internal medicine department of fundus, Shenzhen Eye Hospital from August 2016 to March 2018, were included in this study, including 14 eyes affected by soft drusen and 6 eyes affected by DPED. Among these included patients, there were 7 males and 5 females, with the age of 65-82 years old. Inclusion criteria of soft drusen and DPED: age >50 (Table 1); at least one drusen with a diameter of > 250 μm; drusen fusion with PED with a diameter > 350 μm; exclusion criteria: neovascular AMD, serous and hemorrhagic PED were excluded[11]. The study complied with Declaration of Helsinki and was reviewed and approved by the Medical Ethics Committee of Shenzhen Eye Hospital (The Ethic number 20180508). All patients accepted SMLT treatment and signed the informed consent form voluntarily.
MethodsAll patients have got best corrected visual acuity (BCVA), slit-lamp microscopy, fundus photography (Visucam Carl Zeiss Meditec, Jena, Germany, or TRC-50DX Topcon, Japan), fundus autofluorescence (FAF), microperimetry (MP-3, NIDEK, Japan), fluorescein fundus angiography (FFA) and indocyanine green angiography (ICGA) (Spectralis HRA; Heidelberg Engineering; Heidelberg, Germany) and spectral-domainoptical coherence tomography (SD-OCT) (Carl Zeiss Meditec, Jena, Germany). Choroidal neovascularization was excluded through FFA and ICGA.
StudyProtocolMeasurement of soft drusen or DPED and SMLT treatment area management.C0-C4 standards was adopted for measurement of the size of soft drusen through fundus photography; drusen or DPED with the diameter of larger than 250 μm was included into SMLT treatment[12]; drusen or DPED was positionedviastandard grid classified by AMD on the 488 nm FAF picture of Spectralis HRA (Figure 1). SMLT treatment area was drawn by hand within the scope of 1000-3000 μm[13].
MeasurementoftheDiameter,HeightandAreaoftheDrusenorDPEDSD-OCT was adopted in B scan and Brm was taken as the reference plane. The diameter of drusen or DPED, and the height from Brm to the boundary of RPE were measured with RPE advanced analysis software. The area was the product of diameter and height of drusen or DPED[11,14].
TreatmentProcedureSupra 577 Yellow Laser was applied to carry out SMLT treatment (Quantel Medical Co, France). The parameters of micro-pulse laser are as follows: laser wavelength 577 nm yellow light, duty cycle (DC) of 5%, laser spot of 140-160 μm, high density pattern model was adopted; laser spots with the distance between each other of “0”; the time of exposure was 200ms. The energy titration was carried out on the retina of nasal upper quadrant in micro-pulse mode, to release level I stage spot energy in the mode of continuous impulse wave. Reduced 50% of such energy was performed for treatment[15]. SMLT treatment was carried out in all the patients for twice at enrollment and the third month of visit, respectively. The follow-up visit lasted for 6mo in this study. BCVA, FAF, OCT and fundus photography were taken as the indicators for evaluation of efficacy. The treatment results were analyzed independently by two doctors for ocular fundus disease (Table 2).
StatisticalAnalysisAll statistical analyses were performed using SPSS version 24.0 for Windows software (SPSS, Chicago, IL). BCVA was converted to the logarithm of the minimal angle of resolution (LogMAR) before statistical analyses. The data were expressed as the Mean±Standard deviation (SD). Continuous variables (parametric data distridutions) were performed using Student’st-test.P<0.05 was defined as statistical significance.
RESULTS
Before SMLT treatment, BCVA for soft drusen was 0.318±0.255. After 6mo treatment, BCVA was 0.224±0.205 (P=0.260). Before DPED treatment, BCVA was 0.105±0.090. After 6mo treatment, BCVA was 0.129±0.191 (P=0.736). The difference in the vision of patients in soft drusen group before and after treatment was not statistically significant, so did in DPED group (Table 3). Cod with the baseline values, the vertical diameter and cross-sectional area of soft drusen reduced at the 6mo after treatment, and the differences were statistically significant (P=0.008,P=0.034) (Table 4); Figures 2 (A, B) and Figures 3 (A, B). The differences in diameter, height and cross-sectional area of DPED before and after treatment were not statistically significant (Table 5); Figures 4 (A,B) and Figures 5(A,B,C,D).
Figure 1 Standard red grid on FAF imagine(B), manual painted showed SMLT on soft drusen or DPED area(A).
Table 1 Overview of demographic characteristics of the patients in the drusen group and the drusenoid ped group

GroupsCases/EyesSex (M/F)Age(y)Right eye,n (%)Drusen11/146/575.89±7.962(22.2)Drusenoid PED6/65/180.67±3.334(66.7)
Table 2 All patients information summary
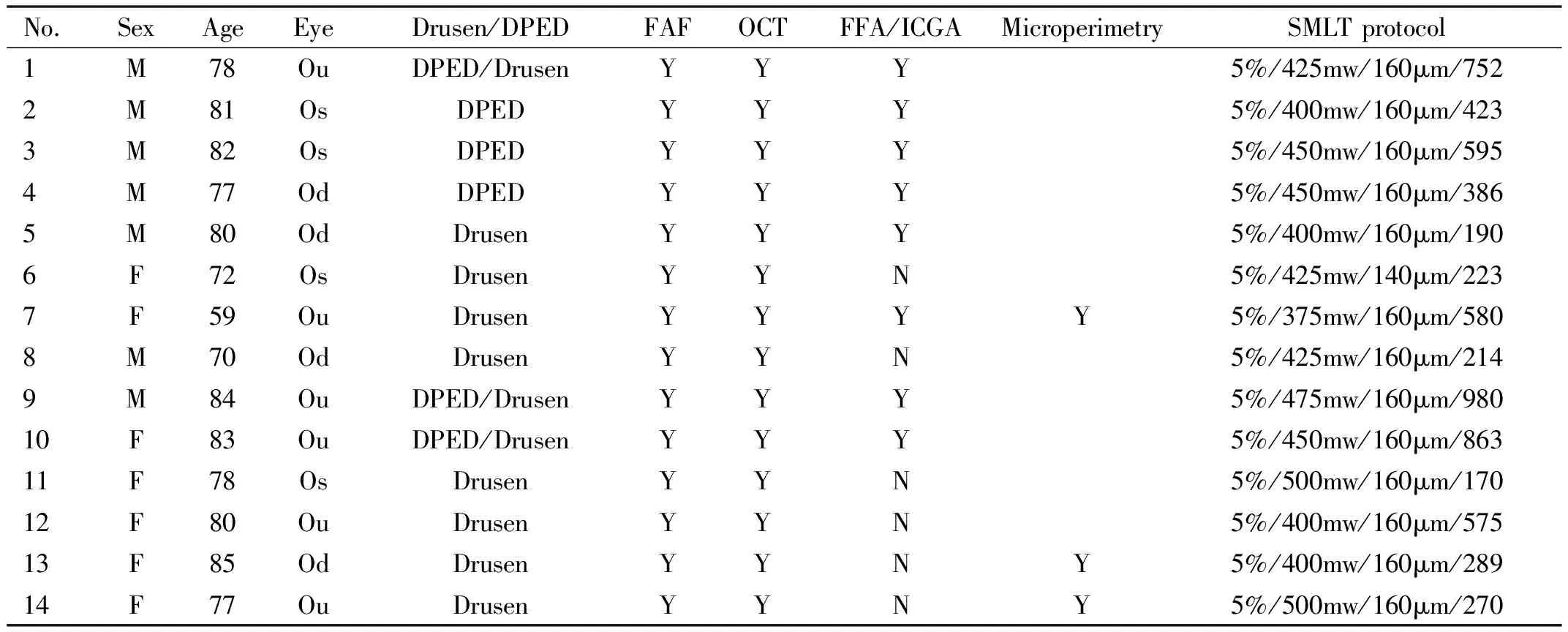
No.SexAgeEyeDrusen/DPEDFAFOCTFFA/ICGAMicroperimetrySMLT protocol1M78OuDPED/DrusenYYY5%/425mw/160μm/7522M81OsDPEDYYY5%/400mw/160μm/4233M82OsDPEDYYY5%/450mw/160μm/5954M77OdDPEDYYY5%/450mw/160μm/3865M80OdDrusenYYY5%/400mw/160μm/1906F72OsDrusenYYN5%/425mw/140μm/2237F59OuDrusenYYYY5%/375mw/160μm/5808M70OdDrusenYYN5%/425mw/160μm/2149M84OuDPED/DrusenYYY5%/475mw/160μm/98010F83OuDPED/DrusenYYY5%/450mw/160μm/86311F78OsDrusenYYN5%/500mw/160μm/17012F80OuDrusenYYN5%/400mw/160μm/57513F85OdDrusenYYNY5%/400mw/160μm/28914F77OuDrusenYYNY5%/500mw/160μm/270
DPED: Drusenoid pigmental epithulium detachment; 5%/425mw/160μm/752, Duty cycle 5%/425mw/160μm/752 spots.

Table 3 Patients’ visual acuity before and after treatment (LogMAR)
Table 4 Summary of morphometric dimensions of drusens treated with subthreshold micropulse laser

Measured parametersMean baseline6moPMin baseline6moMax baseline6moHorizontal diameter,μm468.06±44.78292.64±20.830.166188442010843Vertical diameter,μm127.38±38.5984.26±46.750.008a6729190185s.s-Area,μm264484.5±7672.2528249.31±2595.200.034a15410224432361079659
aDenotes statistically significant; s.s. Area: Cross-sectional area.
DISCUSSION
Drusen is the most typical manifestation of early stage AMD, the drusen with small macular area does not combine with
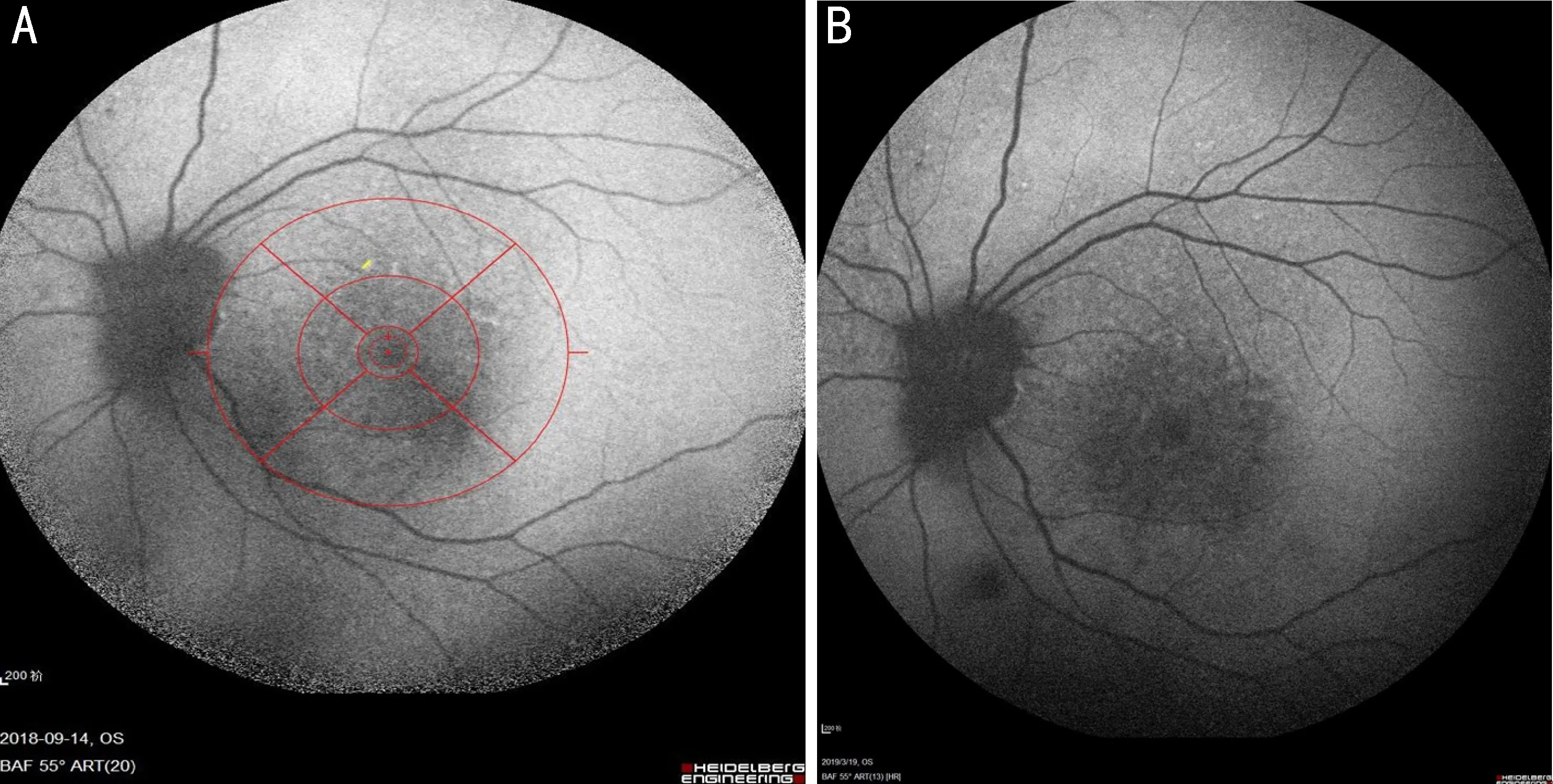
Figure 2 A 59y woman diagnosed soft drusen of both eyes A: SMLTcompared with pre-SMLT; B: FAF imagine showed numbers of soft drusen of left eye reduced after.

Figure 3 Soft drusen OCT imagine showed before and after SMLT Figure B OCT B scan showed soft drusen vertical diameter reduced compared with Figure A(blue arrow).
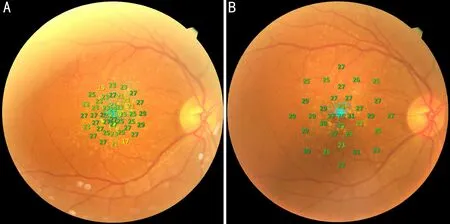
Figure 4 Right eye of the same patient’s microperimetry before SMLT Figure B showed microperimetry sensitivity improved after SMLT compared with Figure A.
Table 5 Summary of morphometric dimensions of drusenoid PED treated with subthreshold micropulse laser

Measured parametersMean baseline6moPMin baseline6moMax baseline6moHorizontal diameter,μm615.11±397.45538.05±489.180.71915611612781677Vertical diameter,μm151.11±61.95118.77±72.700.3257044260266Area,μm2109973 ±11391.6493105.56±14191.670.785109206160332280446082
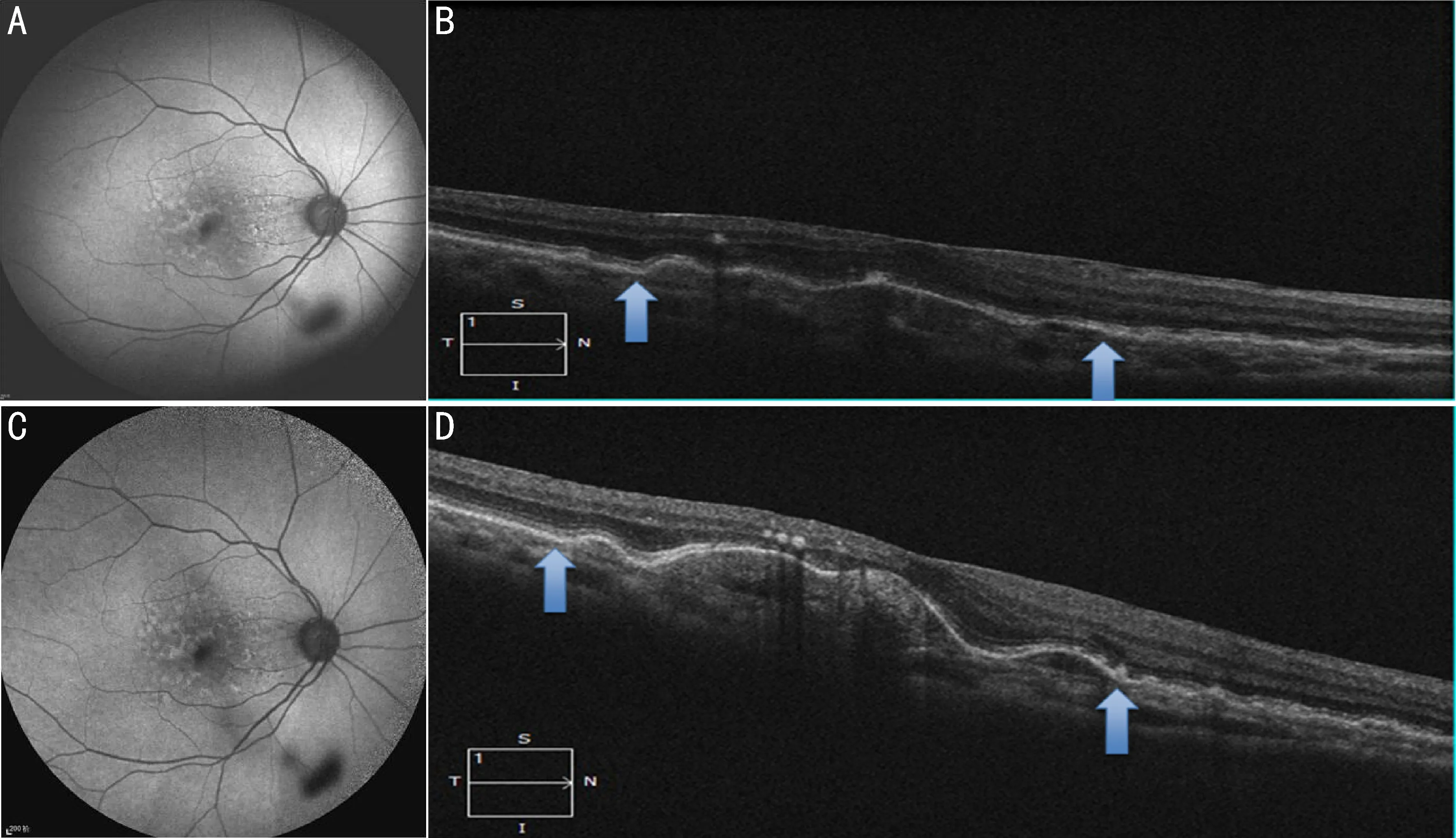
Figure 5 Right eye drusenoid PED showed no significant difference on FAF and OCT imagine before (Figures A, B) and after (Figures C, D) SMLT (blue arrow).
RPE atrophy, the vision acuity of the patient will not be affected. When the large soft drusen or DPED collapse due to natural apoptosis, the vision acuity will even become better in a short period[5,11], but it will finally progress to GA or neovascular AMD. Cukrasetal[7]study showed that 11% and 25% of DPED will develop into CNV-related AMD after 3 years and 10 years respectively. 36% of large soft drusen will progress to progressive AMD, 42% of DPED can develop into advanced AMD, and 55% can progress to focal GA within 5y[6-7].
The literature research of choroidal neovascularization prevention trial (CNVPT) showed that prophylactic laser treatment of soft drusen cannot prevent the occurrence of CNV, and the occurrence rate of CNV in early stage was obviously higher than those in the group without laser treatment[6,8-9]. Some researchers improved the protocol of prophylactic laser treatment of soft drusen and adopted subthreshold micropulse laser with low intensity, short exposure time and minor impairment. The wavelength of the laser is changed from 514 nm argon green laser to 810 nm near infrared laser. The study result showed that traditional subthreshold laser treatment with minor impairment can decrease the quantity of drusen effectively but is not conductive to vision acuity improvement. Fundus photography through SD-OCT, SLO and FAF examination showed that subthreshold laser treatment with 810 nm near infrared laser still causes damage to retina ONL and photoreceptor layer[17]. These results indicated that traditional subthreshold or threshold prophylactic laser is all defective in treatment for soft drusen. Through, our study result showed that SMLT treatment for large soft drusen in the macular region could not improve the BCVA of soft drusen patients (P=0.260), but decrease the soft drusen’s verticalt diameter and cross-session area on OCT figures. Compared with the baseline values, the difference was significant after 6mo treatment (P=0.008; 0.034). FAF examination results indicated that soft drusen decreased and RPE was not damaged after treatment (Figures 5A, C). DPED is a kind of drusen with PED, which is formed by the growing and integration of soft drusen. Due to the apoptosis and autophagy of RPE cells, some DPED may collapse by itself and it will not progress to GA if the RPE layer is not damaged[5].However, as mentioned above, the proportion and risk of DPED turning into GA or CNV related AMD was much higher than those of soft drusen. Therefore, it was more urgent to treat DPED. Although therehave been reports showing that there is good efficacy for DPED with or without CNV in standard dosage PDT treatment or the treatment of continuous intravitreal injection of anti-VEGF[18-20]. However, due to the high cost and lack of indication of PDT and anti-VEGF treatment for DPED, the application is limited. SMLT has the function to regulate growth factors and enzyme; it can adjust blood vessels, leaked VEGF, PEDF, TGF-b2 and heat shock protein and restore the minor damage in RPE; it can be directly applied for the treatment of the chronic central serous chorioretinopathy (CSCR) leaked from RPE of the central fovea of macular, and so it can be used directly on the macularareato treatment of DME and has obtained confirmed efficacy[21].There was rare reports treatment of soft drusen and DPED by SMLT. In our study, there is no obvious impairment to the RPE layer for patients with soft drusen through FAF comparison and no atrophy of RPE layer of the macular region through OCT. The vertical diameter and cross-sectional area of patients with soft drusen decreased after treatment. The study results also indicated that subthreshold micropulse laser treatment is safe and effective; however, our study results showed that there was no significant change in the vertical diameter, horizonal diameter, BCVA after SMLT treatment of DPED compared with the baseline values (P>0.05). So there was no obvious effective in SMLT treatment for DPED. Standard grid was adopted in this study for management, positioning and measurement of drusen with autofluorescence or DPED for convenient therapy and following-up. However, samples in this study were few with short-time observation; there was no measurement for the volume of soft drusen/DPED and no control group was set for comparison. Therefore, the treatment of PED caused by soft drunsen or drusen with subthreshold micropulse laser still needs large samples, control trials and long-term follow-up observation to make further conclusion.