
Bedside score predicting retained common bile duct stone in acute biliary pancreatitis
2020-05-14 01:54:10
World Journal of Clinical Cases 2020年8期
Tawfik Khoury, Anas Kadah, Mahmud Mahamid, Amir Mari, Wisam Sbeit, Faculty of Medicine in the Galilee, Bar-Ilan University, Safed 1311502, Israel
Tawfik Khoury, Anas Kadah, Wisam Sbeit, Department of Gastroenterology, Galilee Medical Center, Nahariya 22100, Israel
Tawfik Khoury, Mahmud Mahamid, Amir Mari, Gastroenterology and endoscopy units, The Nazareth Hospital EMMS, Nazareth 16100, Israel
Abstract
BACKGROUND
Retained common bile duct (CBD) stone after an acute episode of biliary pancreatitis is of paramount importance since stone extraction is mandatory.
AIM
To generate a simple non-invasive score to predict the presence of CBD stone in patients with biliary pancreatitis.
METHODS
We performed a retrospective study including patients with a diagnosis of biliary pancreatitis. One hundred and fifty-four patients were included. Thirty-three patients (21.5%) were diagnosed with CBD stone by endoscopic ultrasound (US).
RESULTS
In univariate analysis, age (OR: 1.048, P = 0.0004), aspartate transaminase (OR:1.002, P = 0.0015), alkaline phosphatase (OR: 1.005, P = 0.0005), gamma-glutamyl transferase (OR: 1.003, P = 0.0002) and CBD width by US (OR: 1.187, P = 0.0445)were associated with CBD stone. In multivariate analysis, three parameters were identified to predict CBD stone; age (OR: 1.062, P = 0.0005), gamma-glutamyl transferase level (OR: 1.003, P = 0.0003) and dilated CBD (OR: 3.685, P = 0.027),with area under the curve of 0.8433. We developed a diagnostic score that included the three significant parameters on multivariate analysis, with assignment of weights for each variable according to the co-efficient estimate. A score that ranges from 51.28 to 73.7 has a very high specificity (90%-100%) for CBD stones, while a low score that ranges from 9.16 to 41.04 has a high sensitivity(82%-100%). By performing internal validation, the negative predictive value of the low score group was 93%.
CONCLUSION
We recommend incorporating this score as an aid for stratifying patients with acute biliary pancreatitis into low or high probability for the presence of CBD stone.
Key words: Stones; Common bile duct; Predictors; Biliary; Pancreatitis
INTRODUCTION
Gallstones are considered the most common cause of acute pancreatitis[1]. According to previous studies they represent about 40%-50% of all causes of acute pancreatitis[2-4].Gallbladder stones are considered a major health problem in developed countries,with an overall prevalence among adult populations between 10%-20%[5,6].
Acute biliary pancreatitis (ABP) results from migration of gallbladder stone through the cystic duct into the common bile duct (CBD) which causes either transient or persistent obstruction of the pancreatic duct, resulting in subsequent development of pancreatitis. Most gallstones are smaller than 5mm in diameter[7-9]. Only a small percentage, around 25% of patients presenting with ABP will have retained CBD stones, while the majority of CBD stones will pass spontaneously given their small size[10-12]. Therefore, CBD imaging is necessary to identify those patients with ABP who have persistent CBD stones[13]. Modalities available for investigation include endoscopic ultrasound (EUS), magnetic resonance cholangiopancreatography(MRCP), laparoscopic ultrasound, and intraoperative cholangiography[14]. In clinical practice, the decision to clarify suspicion of CBD stone by imaging or to proceed directly to endoscopic retrograde cholangiopancreatography (ERCP) due to strong suspicion, is based on a combination of clinical, laboratory and ultrasound or computed tomography findings, in addition to diagnostic methods and resources available in each medical center. However, before proceeding to ERCP with its complication rate of about 5%-10% including post-ERCP pancreatitis (PEP),cholangitis, perforation, and hemorrhage[15-17], presence of CBD stone should be ascertained. The American Society of Gastrointestinal Endoscopy (ASGE) has proposed a strategy to assign the risk of CBD stones in patients with symptomatic cholelithiasis based on clinical, laboratory and sonographic parameters. They were divided according to strength of the parameters into “very strong”, “strong” and“moderate” predictors. The proposed strategy advocate proceeding to ERCP in patients with one “very strong” or two “strong” predictors, or performing an investigative procedure in patients with parameters ranked otherwise[14]. A recent study reported that the specificity of the ASGE very strong predictors was 74% and the positive predictive value (PPV) was 64% with more than one-third of patients undergoing diagnostic ERCP[18]. Although no single parameter consistently and strongly predicts the existence of CBD stones, previous studies have shown that combining clinical, laboratory and imaging predictors together improve the diagnostic accuracy of CBD stones[19-21]. In these guidelines, clinical gallstone pancreatitis by itself received moderate strength in predicting CBD stones[14].
However, we believe that this group is not homogeneous and includes a diverse population with different probabilities of suffering from retained CBD stone.Therefore, this probability may be influenced by additional parameters that deserve clarifying in order to offer the appropriate treatment for each patient.
The aim of the present study was to develop a simple, practical, non-invasive score combining routinely-determined and easily available clinical, laboratory and radiological parameters to predict the presence of CBD stones in patient’s presenting with acute biliary pancreatitis
MATERIALS AND METHODS
The study cohort consisted of all patients over 18 years old with acute pancreatitis based on clinical, laboratory and radiological criteria, and hospitalized in Galilee Medical Center, Israel, between 2012-2018. The diagnostic criteria for acute pancreatitis included typical abdominal pain, elevation of pancreatic enzymes at least three times the upper normal limit and the presence of typical findings of pancreatic inflammation at imaging.
All underwent EUS examination for investigation of suspected underlying biliary stones [abnormal bilirubin, elevated liver enzymes or dilated CBD on ultrasound(US)], and showed evidence of gallbladder stones by US. In our medical center, EUS is the procedure of choice for suspected CBD stones. A recent meta-analysis found EUS to have high sensitivity of 84%-100% and specificity of 94%-100% in detecting CBD stones[22]and EUS has recently been proposed as the new gold standard in the diagnosis of CBD stones[23]. Exclusion criteria included patients with established alternative cause for acute pancreatitis (such as hyperlipidemia, hypercalcemia,alcohol, congenital pancreatic anomalies and genetic predisposition).
All medical records of eligible patients were reviewed and the following parameters were collected: Demographic data (age, gender), laboratory tests [alanine aminotransferase (ALT), aspartate transaminase, alkaline phosphatase, gammaglutamyl transferase (GGT), total bilirubin, white blood cells], and radiologic findings(gallbladder and CBD stones by US and EUS, CBD width as assessed by imaging).The laboratory parameters and the ultrasonographic measurement were assessed up to 24 h prior to the EUS performance.
CBD width up to 6 mm was considered normal; while greater values were considered dilatation of the duct even in patients after cholecystectomy since a search of the professional literature did not yield firm values of the diameter in patients after cholecystectomy. All EUS examinations throughout the study were performed by an experienced endoscopist with a high volume of examinations over 15 years’experience in the field of advanced endoscopy. The study protocol was approved by our medical center’s IRB. Written informed consent was waived by the IRB due to the retrospective, non-interventional nature of the study.
Statistical analysis
Before any statistical processing and analysis, data were visually inspected and checked for outliers. Descriptive statistics performed for the purpose of comparison between the two groups of patients, with and without common bile duct stones.Continuous variables were computed as arithmetic mean and standard deviation,whereas categorical variables were expressed as percentages. Univariate and multivariate logistic regression models were generated to calculate the odds ratios(OR) of several parameters with a backward selection type used. For the purpose of generation of a new multivariate regression model that encompassed parameters including (age, CBD width by US and GGT enzyme level), we credited a weight to each factor based on its coefficient estimates. Receiver operator characteristics (ROC)curve, odds ratio and positive likelihood ratio were used for diagnostic accuracy estimation. Results withP< 0.05 were considered statistically significant. Analyses were performed by using the statistical analysis software [SAS Vs 9.4 Copyright (c)2016 by SAS Institute Inc., Cary, NC, United States].
RESULTS
Demographics and laboratory findings
Overall, 1750 patients underwent EUS during the study period. Among them, a total of 154 patients fulfilled the diagnostic criteria for acute pancreatitis who underwent EUS for assessment of CBD stone were included in the study. Among them, 121 patients (78.5%) did not have CBD stones according to EUS (group A) compared to 33 patients (21.5%) who did (group B). The mean age in groups A and B were 54.8 ± 18.8 and 68.9 ± 14.3 years, respectively. Fifty-seven patients in group A and 11 in group B were males. The mean CBD width by US was higher in group B compared to group A(7.3 mmvs6.4 mm). Table 1 demonstrates demographic and laboratory parameters.
Parameters associated with CBD stones on univariate regression analysis
In univariate regression analysis, several predictors of CBD stones in acute biliary pancreatitis were statistically significant (Table 2), including: Age (OR: 1.048, 95%CI:1.021-1.076,P= 0.0004), aspartate transaminase (OR: 1.002, 95%CI: 1.001-1.004,P=0.0015), alkaline phosphatase (OR: 1.005, 95%CI: 1.002-1.008,P= 0.0005), GGT (OR:1.003, 95%CI: 1.001-1.004,P= 0.0002) and CBD width by US (OR: 1.187, 95%CI: 1.004-1.402,P= 0.0445). On the other hand, total bilirubin shows non-statistically significant difference between the two groups (OR: 1.033, 95%CI: 0.964-1.108,P= 0.35) (Table 2).In multivariate regression analysis, three parameters were identified to significantly predict CBD stones: Age (OR: 1.062, 95%CI: 1.026-1.097,P= 0.0005), GGT level (OR:1.003, 95%CI: 1.001-1.004,P= 0.0003) and dilated CBD (OR: 3.685, 95%CI: 1.160-11.711,P= 0.027), with area under the curve of 0.8433 determined by a ROC curve (Figure 1).
Building of diagnostic score
For the purpose of structuring a diagnostic score, rounded co-efficient estimates were calculated and accordingly each significant parameter on multivariate regression analysis was assigned a weight according to the estimates (Table 3). Then we developed a diagnostic equation [0.5 × age (years) + 0.02 × GGT (U/L) + 10 × CBD width (mm) by US] that generates cut-off points of the parameters included into the equation (age in years, and GGT (U/L) and CBD width in millimeters by US) with their corresponding sensitivity, specificity, PPV and negative predictive value (NPV),with ROC curve for this diagnostic score of 0.8423 (OR: 1.136, 95%CI: 1.079-1.196,P<0.0001, likelihood ratio 39.6) (Figure 2). Table 4 demonstrates the equation cut-off points with their corresponding statistic diagnostic values. As shown, score that ranged from 51 to 74 had a very high specificity (90%-100%) for CBD stones,suggesting that these patients might be referred directly to ERCP. By performing internal validation, we found that in this group of 23 patients, 15 were found to have CBD stone (65.2%). On the other hand, a score that ranges from 9 to 41 has a high sensitivity (82%-100%), suggesting that these patients might be managed without further endoscopic intervention. This group consisted of 97 patients, and only seven were found to have CBD stone (7.2%) with NPV of 93%. The third group, with a score of 41-51, needed further investigation by EUS or MRCP to rule out CBD stone. In this group of 34 patients, 11 patients were diagnosed with CBD stone (32.3%).
DISCUSSION
Although the majority of CBD stones causing acute pancreatitis, pass spontaneously through the papilla, still about 20%-30% of these stones are retained in the bile ducts with the potential of causing recurrent acute pancreatitis or cholangitis that may lead to adverse outcome[10-12]. This subset of patients comprises the most problematic group among those hospitalized with ABP and all diagnostic efforts should be carried out in order to identify them and offer treatment to release the obstructing bile duct stone.Early ERCP in patients with persistent CBD stone decreases the rate of biliary complications such as cholangitis, and improves clinical outcomes[24,25]. Previous studies have attempted to assess various clinical, laboratory and radiological parameters including liver function tests and ultrasound findings to predict CBD stone[26,27]. However, individual components of liver function test and US findings(CBD width) have limited diagnostic yield[28]. The ASGE-proposed strategy assigns risk of CBD stone in patients with symptomatic cholelithiasis according to strength of parameters where clinical gallstone pancreatitis is considered a moderate predictor.However, those parameters have limited diagnostic accuracy[14]. Several imaging tools are available for the diagnosis of CBD stones, including MRCP, EUS and ERCP;however, these tools are either invasive or associated with certain morbidity and mortality (ERCP and EUS) or they are expensive, such as MRCP[29]. These modalities are usually used to confirm or treat suspected CBD stone based on clinical, laboratory and US or computed tomography findings. Although the ASGE-proposed strategy to assign risk of CBD stone considers clinical gallstone pancreatitis a moderate predictor of CBD stone, this is a non-homogeneous group of patients with diverse clinical presentations under the same diagnosis of acute pancreatitis, and thus have different probabilities of suffering from retained CBD stone. These probabilities may be influenced by additional parameters that deserve clarifying in order to offer the appropriate treatment for each patient.
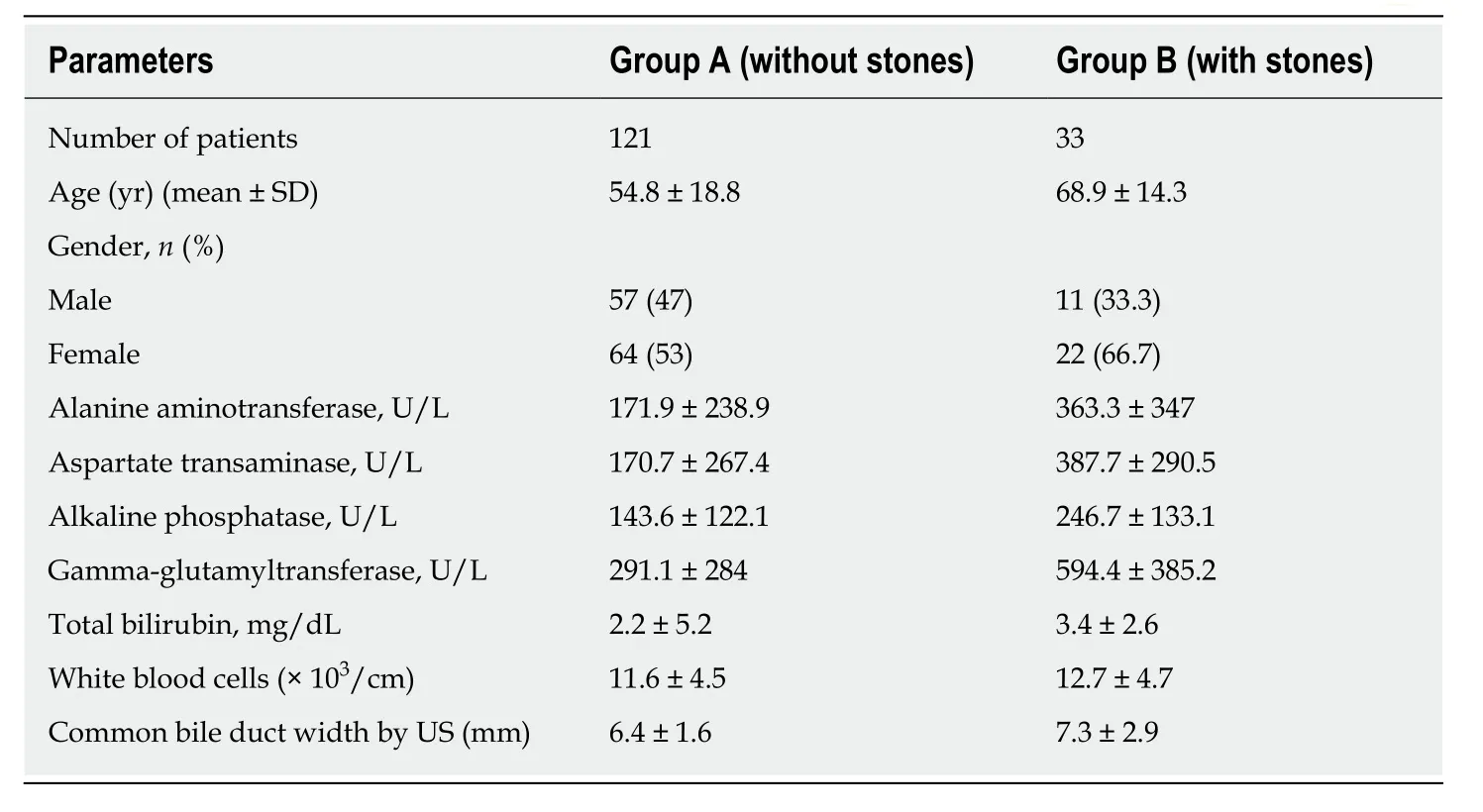
Table 1 Demographics and laboratory characteristics of study cohort
In an attempt to isolate and identify this small, albeit high-risk group of patients with retained CBD stone, we retrospectively identified and integrated clinical,laboratory and radiological parameters that were most predictive of the presence of CBD stones in patients with acute pancreatitis into a simple bedside diagnostic score.Those patients would most benefit from direct referral to therapeutic ERCP, saving them the potential complications of invasive and costly diagnostic procedures such as EUS and MRCP. We could identify that advanced age, abnormal GGT level and dilated CBD by US were the most powerful factors predicting the presence of bile duct stone in biliary pancreatitis patients. Our results are in line with previous studies; it is well known that the prevalence of gallstone diseases including CBD stones increases with age[19]. A former study showed that among patients referred for EUS for evaluation of CBD stone, the prevalence has increased up to 32% in patients above 70 years of age as compared to 14% in patients less than 70 years of age[20].Another study demonstrated that CBD width above 6 mm showed significant positive correlation with CBD stones[30]. However, the sole dilatation of CBD on abdominal imaging tends to support the diagnosis of gallstone pancreatitis with variable and limited sensitivity of 55%-91%. Moreover, GGT level was shown to be the most significant predictor for CBD stones as being demonstrated by previous two studies[31,32], with the highest NPV among other non-invasive parameters[31], but had limited PPV and sensitivity. Therefore, several investigators addressed the performance of multiple variables in predicting high probability of CBD stone[19-21].
By integrating patient age in years, GGT value in U/L and dilated CBD as defined by > 6 mm in width by US, we could generate a simple diagnostic score. This method can provide practitioners with a simple bedside tool to stratify patients into three different groups according to the above-mentioned equation and offer them the appropriate treatment while saving unnecessary investigations. According to this equation score that ranges from 51 to 74 has a very high specificity (90%-100%) for CBD stones, this subset of patients might be referred directly to ERCP. A score that ranges from 9 to 41 has a high sensitivity (82%-100%), suggesting that this group might not benefit from invasive costly investigative procedures and may be managed conservatively without further endoscopic intervention. The third group with a score of 41 to 51 merits additional investigation such as EUS or MRCP because of intermediate probability of CBD stone. These results clearly show that the probability of having a retained CBD stone in patients with acute biliary pancreatitis is influenced by additional parameters. Thus, they should not be regarded as a homogenous group,as this strategy may lead to unnecessary investigations where the probability of choledocholithiasis is high enough to warrant therapeutic ERCP or low enough to refrain from further investigation.
The limitations of our study are its retrospective nature of data collection and the fact that it was conducted in a single center. another limitation is that we didn’t validate our findings in an independent validation cohort. Thus, our findings should be validated by an external validation cohort.

Figure 1 Receiver operating characteristic curve analysis for age, gamma-glutamyltransferase level and dilated common bile duct on multivariate regression analysis. AUC: Area under the curve.
In conclusion, we have developed a scoring system based on three parameters to predict the presence of CBD stone in patients admitted with ABP. Our study has clinical implications, as it might be used as an important aid for practitioners to guide them towards a more prudent decision regarding therapeutic plans for their patients.In this way, they may offer therapeutic ERCP when the probability of CBD stone is high, and avoid unnecessary investigations in patients with low probability of CBD stone.
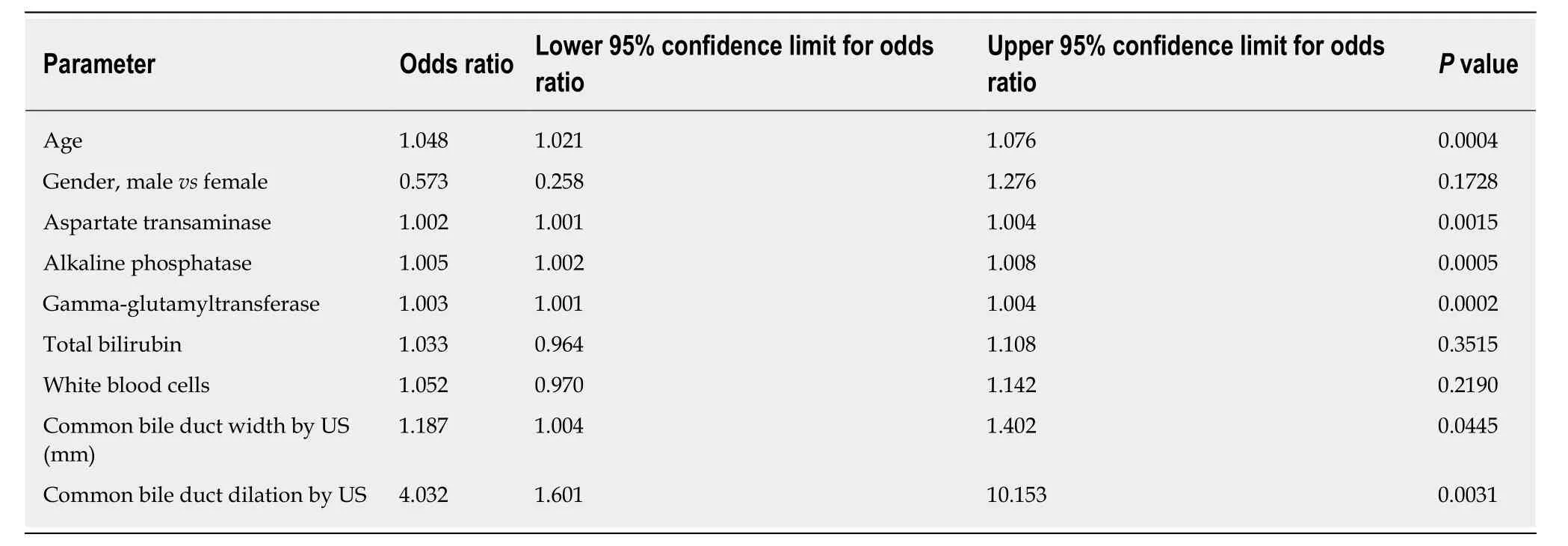
Table 2 Univariate analysis of parameters associated with common bile duct stones

Table 3 Variables that were independently associated with common bile duct stones and their corresponding weight points given according to coefficient estimates

Table 4 Equation generated cut-off points with their corresponding diagnostic statistics [age (yr) × 0.5 + gamma-glutamyl transferase(U/L) × 0.02 + common bile duct width by ultrasound (mm) × 10]
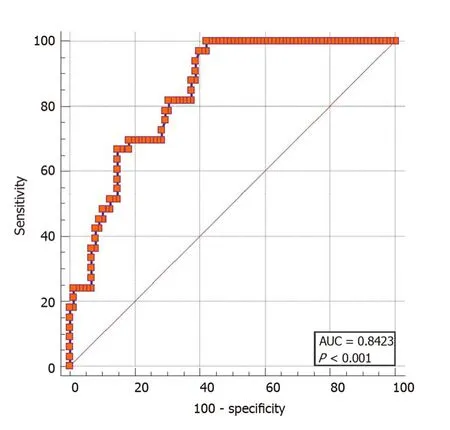
Figure 2 Receiver operating characteristic curve analysis of the score developed [0.5 × age + 0.02 × gamma-glutamyltransferase (U/L) + 10 × common bile duct width by ultrasound]. AUC: Area under the curve.
ARTICLE HIGHLIGHTS
Research background
Gallbladder stones are the commonest cause of acute biliary pancreatitis. Despite that most of the stones are expelled spontaneously through the papilla due to their small size; about 20% to 30%of patients with acute biliary pancreatitis will have persistent common bile duct (CBD) stones.Thus, it is important to identify this subset pf patients since they will need endoscopic stone removal. In real clinical practice, the decision to perform an imaging modality for clarifying a suspicion of CBD stone or to proceed directly to endoscopic retrograde cholangiopancreatography (ERCP) because of strong suspicion of CBD stone is mostly based on combinations of clinical, laboratory and ultrasound findings. Many investigators have noted that the probability of CBD stones is higher in the presence of multiple predictors. We characterized clinical, laboratory and radiological parameters which are easily available that can predict the presence of retained CBD stones among patients hospitalized with acute biliary pancreatitis.
Research motivation
The main driver for performing this study was to develop simple bedside score based on easily available parameters that predicts the presence of retained biliary stones, since identification of CBD stone is crucial to relieve biliary obstruction. This score might stratify patients into low or high-risk probability for retained CBD stone and subsequently assist clinicians in performing further confirmatory/therapeutic tests.
Research objectives
Given that retained biliary in the setting of acute biliary pancreatitis required performing certain imaging such as endoscopic ultrasound (EUS) or magnetic resonance cholangiopancreatography(MRCP) which are either invasive or not widely available, we aimed to explore simple easily available clinical, laboratory and imaging parameters that predict CBD stone with good statistical performance.
Research methods
We performed a single center retrospective case control study including 154 patients with presumed diagnosis of acute biliary pancreatitis who underwent EUS. The strength of our study is that we relied on EUS as a gold standard for the diagnosis of CBD stones, and second that we aimed to combine several parameters to generate scoring system that could predict CBD stone with high probability.
Research results
After assessment of several clinical, laboratory and radiological parameters, we were able to identify 3 parameters that were statistically significant on univariate and multivariate regression analysis including age, GGT level and CBD width by US. Using these variables, we generated a score predicting the presence of retained CBD stones. A score that ranges from 51.28 to 73.7 has a very high specificity (90%-100%) for CBD stones, while a low score that ranges from 9.16 to 41.04 has a high sensitivity (82%-100%), as the patients with the higher score might be referred immediately for ERCP without the need for further investigations, while the low score cut-off points might benefit from watch and see strategy or other confirmatory tests for CBD stones.
Research conclusions
For the first time, we were able to generate a simple scoring system that predicts the presence of retained CBD stones among patients with acute biliary pancreatitis. Currently, the professional societies including the American Society of Gastrointestinal Endoscopy and the ESGE are relying on individualized predictors of CBD stones. The ability to incorporate several variables into one scoring system further improve the diagnostic accuracy of this score, as is known that combining several predictors for CBD stone is superior to each predictor alone. Thus, our score might be already introduced into the daily clinical practice that guide therapeutic decisions.
Research perspectives
The diagnosis of retained CBD stone in acute biliary pancreatitis is somehow challenging as it based on single abnormal laboratory or ultrasonographic tests. However, once a suspicion is raised, most clinicians proceed to other confirmatory tests, mainly EUS which is invasive test or MRCP which is costly and not easily available. However, as we shown that combining predictors for CBD stone into one scoring system had an excellent diagnostic performance. This will allow clinicians to avoid performing other unnecessary imaging studies. Large prospective cohort studies assessing combination of several CBD stone simple predictors are warranted.
 World Journal of Clinical Cases2020年8期
World Journal of Clinical Cases2020年8期
- World Journal of Clinical Cases的其它文章
- Clinicopathological differences and correlations between right and left colon cancer
- Stability and infectivity of coronaviruses in inanimate environments
- Status, challenges, and future prospects of stem cell therapy in pelvic floor disorders
- Unusual presentation of congenital radioulnar synostosis with osteoporosis, fragility fracture and nonunion: A case report and review of literature
- Predictive factors for central lymph node metastases in papillary thyroid microcarcinoma
- Suicide attempt using potassium tablets for congenital chloride diarrhea: A case report