
Camrelizumab (SHR-1210) leading to reactive capillary hemangioma in the gingiva: A case report
2020-05-14 01:51
World Journal of Clinical Cases 2020年3期
Qing Yu, Wen-Xia Wang, Department of Periodontology, School and Hospital of Stomatology,Shandong University, Shandong Key Laboratory of Oral Tissue Regeneration, Shandong Engineering Laboratory for Dental Materials and Oral Tissue Regeneration, Jinan 250012,Shandong Province, China
Abstract
BACKGROUND
Oncologic immunotherapy is attracting attention as an effective strategy for cancer treatment. Currently, there are two kinds of inhibitors: Anti-PD-1 antibodies and anti-PD-L1 antibodies. These inhibitors have shown significant implications in improving the outcomes of certain cancer types in recent years.However, along with its effectiveness, adverse events cannot be ignored. As an anti-PD-1 antibody, camrelizumab (SHR-1210) has some side effects in tumor immunotherapy. The most common adverse event is reactive capillary hemangioma. While it is widely reported to occur in the skin, gingival reactive capillary hemangioma is rarely reported.
CASE SUMMARY
A 54-year-old man complained of gingival overgrowth on the anterior aspect of the maxilla and mandible for more than 6 mo. He had been placed on SHR-1210 for lung cancer for 7 mo. A gingival mass extending from canine to canine was noted on the lingual surfaces of the mandible. Gingival enlargement was noted in the front teeth. A clinical diagnosis of gingival reactive capillary hemangioma and chronic periodontitis was made. The treatment involved a complex local treatment (repeated local applications of an antibiotic paste, scaling and root planning, and surgery). The excised tissue was sent for histopathological examination, which confirmed the diagnosis of capillary hemangioma. After the operation, most of the gingival enlargement was reduced. At the 2-mo follow-up,it was noted that the gingival overgrowth was immediately reduced after the replacement of the anti-PD-1 agent with an anti-PD-L1 agent.
CONCLUSION
As the prescription for SHR-1210 has increased considerably in recent years, the occurrence of its possible side effects, including gingival reactive capillary hemangioma, has increased. It is recommended that regular oral examinations be performed before and during the treatment of tumors with SHR-1210.
Key words: Camrelizumab; Adverse effects; Reactive capillary hemangioma; Gingiva;Case report
INTRODUCTION
Oncologic immunotherapy is attracting attention as an effective strategy for cancer treatment. The PD-1 pathway inhibits the T cell antitumor immune response in the local tumor microenvironment[1,2]. Currently, there are two kinds of inhibitors that inhibit the PD-1 pathway: Anti-PD-1 antibodies and anti-PD-L1 antibodies[3]. These inhibitors have shown significant implications in improving the outcomes of certain cancer types in recent years, such as melanoma, renal cell carcinoma, non-small cell lung cancer, small cell lung cancer, and gastric cancer[4]. However, along with its effectiveness, adverse events cannot be ignored, including diarrhea, rash, pruritus,dry mouth, vitiligo,etc.[5-8].
Camrelizumab (SHR-1210) is a kind of anti-PD-1 antibody. It was reported that a unique treatment-related adverse event was reactive capillary hemangioma[9-11].Notably, most reactive capillary hemangiomas occur in the skin[10], and this side effect is rarely seen in oral tissues. In this report, we describe the case of a patient who experienced gingival reactive capillary hemangioma during SHR-1210 treatment for lung cancer.
CASE PRESENTATION
Chief complaints
A 54-year-old man visited the Department of Periodontology, Stomatological Hospital of Shandong University, China with a complaint of gingival overgrowth on the anterior aspect of the maxilla and mandible, which had been present for more than 6 mo.
History of present illness
The patient had been placed on SHR-1210 (200 mg through intravenous transfusion biweekly) for lung cancer for 7 mo. During the treatment, the patient had taken nifedipine for 1 mo. Then, he noted overgrowth on the anterior aspect of the maxilla and mandible later. After the cessation of nifedipine, the enlargement decreased in size on the palatal surfaces of the maxillary anterior teeth and gradually increased in size on the lingual surfaces of the mandibular anterior teeth. He used metronidazole,which was not effective.
History of past illness
A review of the patient’s medical history revealed nothing significant other than lung cancer and hypertension.
Personal and family history
The patient has no significant personal or family history.
Physical examination upon admission
The extraoral examination was normal. The intraoral examination revealed an interdental papilla enlargement in the upper anterior region, with moderate gingival overgrowth presenting on the facial aspects of the lower anterior region and a gingival mass extending from canine to canine on the lingual surfaces of the mandible(Figure 1). The mass was magenta colored, discrete, pedunculated, and bleeding on palpation. In addition, mobility examination revealed grade I mobility in tooth 43;grade II mobility in teeth 11, 21, and 32; and grade III mobility in teeth 31, 41, and 42.
Laboratory examinations
All routine blood investigations were unremarkable.
Imaging examinations
The radiographic examination showed severe horizontal bone resorption in teeth 31 and 41 and mild horizontal bone resorption in the upper front teeth. It also revealed moderate horizontal bone resorption in the upper and lower alveolar bone (Figure 2).
FINAL DIAGNOSIS
Reactive capillary hemangioma; chronic periodontitis.
TREATMENT
The treatment plan was oral hygiene instructions, supra- and sub-gingival scaling,repeated local applications of an antibiotic paste (tetracycline), surgical removal of the epulis, and supportive periodontal treatment. The instructions consisted of mechanical toothbrushing and a chlorhexidine (0.12%) rinse. After obtaining informed consent from the patient, the lingual lesion around the lower anterior teeth was completely excised under local anesthesia using a semiconductor laser. The excised tissue was sent for histopathological examination.
OUTCOME AND FOLLOW-UP
Microscopic examination showed a stratified squamous surface epithelium. The connective tissue stroma was composed of loosely arranged collagen fiber bundles interspersed with moderate chronic inflammatory cell infiltration of lymphocytes and plasma cells and many blood vessels containing red blood cells (Figure 3). The histopathological features confirmed the diagnosis of capillary hemangioma.
At the 2-wk postoperative appointment, the surgical site healed uneventfully with gingival color normalization and slight swelling (Figure 4A). The mobility of teeth 31,41, and 42 improved to grade II. However, the interdental papilla overgrowth around the upper anterior teeth was magenta colored and soft in consistency (Figure 4B and C). Concerns were raised that SHR-1210 might be the cause of epulis. The patient’s oncologist changed his antineoplastic medication 2 mo later by replacing the anti-PD-1 agent with an anti-PD-L1 agent. He then reported a reduction in gingival overgrowth immediately after the cessation of SHR-1210.
DISCUSSION
Immunotherapy has been accepted as an alternative therapy to surgery,chemotherapy, and radiotherapy for tumors. Anti-PD-1 and anti-PD-L1 agents have been suggested to be effective for certain tumors[4]. However, some adverse events have been reported[8]. SHR-1210 is a kind of anti-PD-1 agent. Since it was applied to clinical management, SHR-1210 has been reported to cause skin capillary hemangioma. The average time to occurrence was 23 d[10].
The patient developed gingival enlargement after the application of SHR-1210 and nifedipine (Figure 1). As a calcium channel blocker, nifedipine can induce gingival hyperplasia. Here, an important question is what the true underlying cause of the gingival overgrowth and epulis was. It was reported that spontaneous regression of capillary hemangioma is observed after the termination of SHR-1210[10]. There is evidence that cessation of nifedipine can reduce excessive gingival growth[12,13]. The mass was still present after the patient stopped taking nifedipine. However, the patient’s gingival mass disappeared after the cessation of SHR-1210. In addition,histological examination showed capillary hemangioma (Figure 3). Thus, it could be considered that epulis was caused by SHR-1210.

Figure 1 Initial aspects of the gingiva. A: A gingival mass extending from canine to canine on the lingual surfaces of the mandible; B: A moderate gingival overgrowth presenting on facial aspects of the lower anterior region; C: An interdental papilla enlargement in the upper anterior region.
Reactive capillary hemangioma is a unique adverse effect related with camrelizumab treatment[11], and a total of 85.7% of patients with advanced solid tumors who received camrelizumab monotherapy developed reactive capillary hemangioma[14]. The exact mechanisms of SHR-1210-related gingiva capillary hemangioma are still under investigation. A possible explanation is that SHR-1210 is a potent agonist of human VEGFR-2[15]. VEGFR-2 can drive hemangioma development by activating vascular endothelial cell proliferation. In addition, the incidence of reactive capillary hemangioma was 12.1% when those patients were treated with a combination of camrelizumab and apatinib (a VEGFR-2 inhibitor)[16]. Another possible reason may be oral bacterial plaque. Bacterial plaque is the initiator of oral periodontal diseases[17]. The inflammation of the gingiva induced by inadequate oral hygiene seems to enhance the interaction between the drug and gingival tissue[18].
Generally, treatment was not required in the majority of cases, because reactive capillary hemangioma lesions could spontaneously regress after the discontinuation of SHR-1210[14]. Only lesions occurred on the body area prone to friction or with a high risk of bleeding were treated with local therapy, such as laser or surgical resection[14,19].However, in this case, the reactive capillary hemangioma lesion mainly occurred on the lingual aspects of the lower anterior teeth, which was related to difficulty in eating and speaking clearly. In addition, the patient suffered chronic periodontitis.Therefore, we performed several scaling and root planning sessions on the patient.After obtaining informed consent from the patient, the lingual lesion around the lower anterior teeth was completely excised under local anesthesiaviaa semiconductor laser (Figure 4A). After 2 mo, the patient’s oncologist changed his antineoplastic medication to an anti-PD-L1 agent. He then reported spontaneous regression of gingival enlargement immediately after the discontinuation of SHR-1210.
CONCLUSION
As the prescription for SHR-1210 has increased considerably in recent years, the occurrence of its possible side effects, including gingiva reactive capillary hemangioma, has increased. It is recommended that regular oral examination be performed before and during the treatment of tumors with SHR-1210.
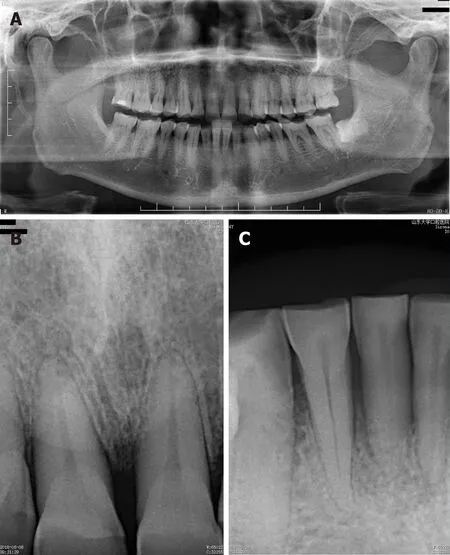
Figure 2 Radiographic aspects. A: Moderate horizontal bone resorption in the upper and lower alveolar bone; B: Mild horizontal bone resorption in the upper front teeth; C: Severe horizontal bone resorption in teeth 31 and 41.

Figure 3 Histopathological findings. A: Many blood vessels in the connective tissue stroma (Hematoxylin and eosin staining; magnification, 40 ×); B: Stratified squamous surface epithelium (Hematoxylin and eosin staining; magnification, 100 ×); C: The connective tissue stroma was composed of loosely arranged collagen fiber bundles interspersed with moderate chronic inflammatory cell infiltration of lymphocytes and plasma cells and many blood vessels containing red blood cells(Hematoxylin and eosin staining; magnification, 100 ×).

Figure 4 Gingival aspects at two weeks after surgery. A: Surgical site healed uneventfully with gingival color normalization and slight swelling; B and C: The interdental papilla overgrowth around the upper anterior teeth.
 World Journal of Clinical Cases2020年3期
World Journal of Clinical Cases2020年3期
- World Journal of Clinical Cases的其它文章
- Comprehensive review into the challenges of gastrointestinal tumors in the Gulf and Levant countries
- Can cyclin-dependent kinase 4/6 inhibitors convert inoperable breast cancer relapse to operability? A case report
- Ruptured splenic peliosis in a patient with no comorbidity: A case report
- Successful kidney transplantation from an expanded criteria donor with long-term extracorporeal membrane oxygenation treatment: A case report
- Boarding issue in a commercial flight for patients with cavitary pulmonary tuberculosis: A case report
- Cytomegalovirus ileo-pancolitis presenting as toxic megacolon in an immunocompetent patient: A case report