AD8联合MOCA量表对中老年体检人群认知功能障碍筛查分析
2020-05-06 13:28王丽娟刘欣鲁翠红王红霞刘荧吕娜
中国医学创新 2020年7期
王丽娟 刘欣 鲁翠红 王红霞 刘荧 吕娜
【摘要】 目的:分析AD8聯合MOCA量表对中老年体检人群认知功能障碍筛查情况。方法:采用方便抽样的方式以体检人群为研究对象,均进行痴呆筛查问卷(AD8)、蒙特利尔认知功能评估(MOCA)、焦虑量表(GAD-7)和抑郁量表(PHQ-9),分析体检人群中认知障碍情况患病情况及影响因素。结果:(1)共收集140例体检者,AD8问卷≥2分的24例(17%),主要以记忆力下降为主。MOCA认知测评发现40例(29%)≤25分,其中26例(19%)存在轻度认知功能障碍(mild cognitive impairment,MCI);GAD-7焦虑自评量表筛查中大于4分22例(16%);PHQ-9抑郁自评量表筛查中大于4分24例(17%)。(2)在高龄、低教育水平组,AD8分值明显高于低年龄组、高教育水平组。MOCA量表测评中高龄、低教育水平组得分明显小于低年龄、高教育水平组,差异有统计学意义。(3)在年龄<55岁人群中,PHQ-9量表及GAD-7量表得分均高于年龄≥55岁人群。(4)多因素分析发现,年龄是认知功能下降的独立危险因素,而教育水平是保护因素。(5)在AD8、MOCA的诊断试验及ROC曲线中发现,MOCA测评敏感度、特异度及ROC曲线下面积明显优于AD8及AD8+MOCA,差异均有统计学意义(P<0.05)。结论:对于年龄≥55岁体检人群,应早期进行MOCA认知筛查,具有较高的敏感度,可早期发现轻度认知功能障碍人群;对于年龄<55岁人群,应关注焦虑、抑郁等神经心理功能的筛查。
【关键词】 体检 认知障碍 中老年人
[Abstract] Objective: To analyze the AD8 combined with MOCA scale in screening for cognitive impairment in middle-aged and elderly people undergoing physical examination. Method: They were given the convenient sampling method, the subjects of physical examination were all investigated by dementia screening questionnaire (AD8), Montreal cognitive function assessment (MOCA), anxiety scale (GAD-7) and depression scale (PHQ-9). The prevalence and influencing factors of cognitive disorders in physical examination population were analyzed. Result: (1)A total of 140 subjects were collected, of which 24 cases (17%) received AD8 questionnaire≥2 scores, mainly dueto memory decline, MOCA cognitive assessment found that 40 cases (29%) ≤25 scores, among which 26 cases (19%) had mild cognitive impairment (MCI). In DAD-7 self-rating scale screening, 22 cases (16%)> 4 scores, PHQ-9 self-rating depression scale screening was greater than 4 scores in 24 cases (17%). (2) In the old age and low education group, the AD8 score was significantly higher than the low age and high education level. The sores of MOCA in the old age and low education level were significantly lower than the low age and high education level group. (3) In people who less than 55 years old, the scores of PHQ-9 scale and GAD-7 scale were higher than those of people aged ≥55 years old. (4) Multi factor analysis showed that age was an independent risk factor for cognitive decline, while education level was a protective factor. (5) In the ROC curve diagnostic test of AD8 and MOCA, the sensitivity, specificity and ROC curve of MOCA were sigrrificantly better than those of AD8 and AD8 + MOCA (P<0.05). Conclusion: The results provide support for the MOCA, has a high senstivity, in identifying mild cognitive impairment for ageing more than 55 years people in physical examination. However, for less than 55 years old, we should pay more attention to the anxiety and depression.[Key words] Physical examination Cognitive impairment Middle-aged and elderly peopleFirst-authors address: Beijing Zhongguancun Hospital, Beijing 100190, China
随着我国老龄化程度加重,痴呆发病率逐年升高,严重影响老年人的身体健康。据报道我国每年痴呆的发生率是4%[1],随着我国60岁以上人口的增多,目前我国痴呆患病数占世界总体痴呆人数的25%[2],痴呆是我国老年人群重要疾病之一,给患者、家庭、社会带来沉重的负担[3]。然而,虽然我国目前痴呆人口较多,发病率高,但知晓率与诊断率远低于高等水平国家,尤其是在农村[4]。王鲁宁[5]教授提倡建立老年人年度例行记忆体检制度,并将痴呆筛查和评估置于常规医疗服务项目中,早期发现认知功能下降人群,早期治疗,针对可治疗因素给予积极控制,逆转或减慢痴呆的发展,提高老年人生活质量,可明显减少痴呆发生。本研究通过对北京市海淀区中关村医院部分体检人群进行认知功能筛查,初步了解体检人群中认知障碍的发病情况及影响因素,提高社区医疗卫生机构对认知障碍的关注,现报道如下。
1 资料与方法
1.1 一般资料 连续收集2017年11月-2018年4月在中关村医院体检中心体检、年龄≥40岁以上人群为研究对象,共140例,男76例,女64例,平均年龄(53±10)岁。纳入标准:年龄≥40岁的体检人群。排除标准:严重的神经功能缺损或伴有精神障碍、严重心脏系统、呼吸系统、肝肾功能损害。该项课题已通过医院伦理学委员会批准,所有调查对象均同意本测评与调查。
1.2 方法 所有调查对象均进行AD8、MOCA、抑郁量表(PHQ-9)、焦虑量表(GAD-7),同时记录调查对象的一般资料(性别、年龄、文化程度、职业、既往史)与相应化验指标。由中关村神经内科课题组统一培训的专科医师在独立安静环境下,进行面对面、一对一的完成AD8、MOCA量表问卷调查。抑郁量表(PHQ-9)、焦虑量表(GAD-7)在充分告知评估方法后由体检者独立完成。问卷结果由课题组人员进行核查,对于不清楚、填写错误、缺项的电话联系核实后再次录入。结果采用双遍录入,保证调查结果的可靠性、准确性。
1.3 观察指标与评价标准 (1)AD8痴呆筛查问卷共包括8个问题,通过询问患者本人来评估记忆力、定向力等认知功能。根据回答“是”或“否”进行评估,在痴呆的极早期阶段,AD8≥2项者被评定可疑有记忆功能障碍,该量表具有较好的信度和效度,敏感度和特异度分别为85.7%、77.6%[6]。AD8阳性标准:AD8评分≥2分,阴性标准:AD8评分<2分。(2)MOCA量表包括视空间结构、执行能力、注意力、记忆力、语言功能、抽象思维、计算和定向力等8个认知领域,可以快速筛查轻度认知功能领域,总分30分,≥25分为正常。检查痴呆的灵敏度为78%,特异度为89%[7],教育年限≤12年者可加一分,分值越高提示认知功能越好。MOCA阳性标准:MOCA评分<25分,阴性标准:MOCA评分≥25分。(3)PHQ-9抑郁自评量表共包括9个问题,最高分27分,最低分0分,分值>4分可能存在抑郁。(4)GAD-7焦虑自评量表,共7个问题,最高分21分,最低分0分,分值>4分可能存在焦虑。(5)MCI诊断依据2003年国际工作组制定的MCI诊断标准[8]:①患者或知情人报告或临床医师发现认知的损害;②存在一个或多个认知领域损害的客观证据;③复杂的工具性日常能力轻微损害,但保持独立的日常生活能力;④未达到痴呆诊断。联合诊断阳性标准:AD8评分≥2分+MOCA评分≤25分,阴性标准:AD8评分<2分+MOCA评分>25分。
1.4 统计学处理 采用SPSS 20.0软件对所得数据进行统计分析,计量资料符合正态分布用(x±s)表示,两样本比较采用独立样本t检验;不符合正态分布采用M(P25,P75)表示,两个独立样本比较采用Wilcoxon秩和检验;多因素分析采用二分类Logistic回归分析;诊断试验评价ROC曲线下面积及敏感度及特异度。以P<0.05为差异有统计学意义。
2 结果
2.1 海淀区体检中心140例健康体检者一般资料 本研究共收回140份调查结果,男76例(54%),女64例(46%);年龄:40~49岁60例(43%),50~59岁32例(23%),60~69岁34例(24%),70~79岁12例(9%),80岁及以上2例(1%);文化程度:小学2例(1%),初中及高中30例(21%),大专46例(33%),大学及以上62例(44%)。AD8自评量表,24例(17%)≥2分;MOCA认知测评,<25分40例(29%);PHQ-9抑郁自评量表,>4分24例(17%);GAD-7焦虑自评量表,>4分22例(16%)。AD8+MOCA测评双阳性结果10例(7%);PHQ-9+GAD-7自评量表均大于4分共14例(10%)。
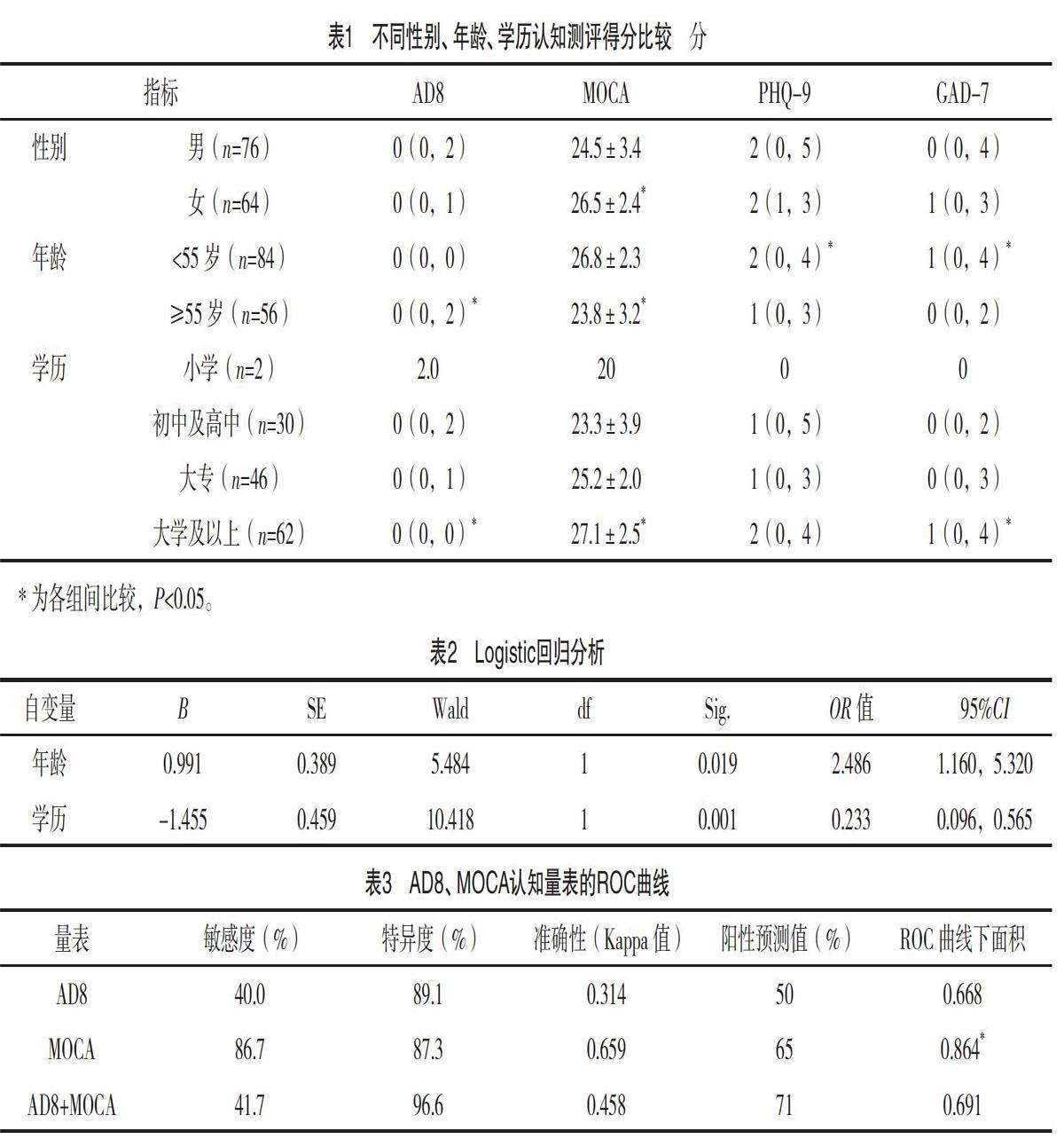
2.2 不同性别、年龄、学历AD8、MOCA、PHQ-9、GAD-7量表得分比较 AD8测评,年龄≥55岁、低教育水平AD8得分均明显高于年龄<55岁、高教育人群(P<0.05)。MOCA认知测评量表,年龄≥55岁人群、低教育人群总分明显低于年龄<55岁、高教育人群(P<0.05);MOCA认知测评中女性得分明显高于男性(P<0.05)。PHQ-9抑郁自评量表与GAD-7焦虑自评量表,年龄<55岁人群,自评得分明显高于年龄≥55岁人群(P<0.05)。大学及以上学历人群GAD-7中得分明显高于低学历人群(P<0.05)。见表1。
2.3 影响认知功能障碍的Logistic回归分析 因变量为是否存在痴呆或轻度认知功能下降(MCI),自变量包括年龄、性别、学历,多因素Logistic回归分析显示,年龄是认知功能下降的独立危险因素,而教育水平是认识功能下降的保护因素,见表2。
2.4 AD8聯合MOCA应用的ROC曲线分析 ROC曲线分析提示,在体检人群中筛查MCI,MOCA量表具有较高的敏感度及特异度,明显高于AD8及AD8+MOCA组,综合发现MOCA测评的ROC曲线下面积最大(P<0.005),见表3。
[4] Jia L,Quan M,Fu Y,et al.Dementia in China:epidemiology,clinical management,and research advances[J].Lancet Neurol,2020,19(1):82-92.
[5]王鲁宁.建立适用于我国临床环境的痴呆筛查和诊断标准化系统[J].中华内科杂志,2018,57(12):865-866.
[6]毛睿智.<
[7] Hsu J L,Fan Y C,Huang Y L,et al.Improved predictive ability of the Montreal Cognitive Assessment for diagnosing dementia in a community-based study[J].Alzheimers Res Ther,2015,7(1):69-76.
[8] Winblad B,Palmer P J,Kivipelto M,et al.Mild cognitive impairment-beyond controversies,toward a consensus:report of the International Working Group on Mild Cognitive Impairment[J].Internal Med,2004,256(3):240-246.
[9] Word Alzheimer report2018[EB/OL].https://www.alz.co.uk/research/World Alzheimer Report 2018.
[10]田金洲,解恒革,秦斌.中国痴呆诊疗指南[M].北京:人民卫生出版社,2017.
[11] Dubois B,Feldman H H,Jacova C,et al.Advancing research diagnostic criteria for Alzheimers disease:the IWG-2 criteria[J].Lancet Neurol,2014,13(6):614-629.
[12]韓璎.中国阿尔茨海默病临床前期主观认知下降诊治策略流程与规范专家共识[J].中国临床医学影像杂志,2018,29(8):534-538.
[13] Sun Y,Yang F C,Lin C P,et al.Biochemical and neuroimaging studies in subjective cognitive decline:progress and perspectives[J].CNS Neurosci Ther,2015,21(10):768-775.
[14] Visser P J,Tijms B.Brain Amyloid Pathology and Cognitive Function:Alzheimer Disease Without Dementia?[J].Jama,2017,317(22):2285-2287.
[15] Xue J,Li J,Liang J,et al.The Prevalence of Mild Cognitive Impairment in China:A Systematic Review[J].Aging Dis,2018,9(4):706-715.
[16] Ciesielska N,Sokolowski R,Mazur E,et al.Is the Montreal Cognitive Assessment(MoCA) test better suited than the Mini-Mental State Examination(MMSE) in mild cognitive impairment(MCI) detection among people aged over 60? Meta-analysis[J].Psychiatr Pol,2016,50(5):1039-1052.
[17] Chen H H,Sun F J,Yeh T L,et al.The diagnostic accuracy of the Ascertain Dementia 8 questionnaire for detecting cognitive impairment in primary care in the community, clinics and hospitals:a systematic review and meta-analysis[J].Fam Pract,2018,35(3):239-246.
[18] Brown D S,Bernstein I H,McClintock S M,et al.Use of the Montreal Cognitive Assessment and Alzheimers Disease-8 as cognitive screening measures in Parkinsons disease[J].Int J Geriatr Psychiatry,2016,31(3):264-272.
[19] Word Health Organization.Investing in treatment for depression and anxiety leads to fourfold return. Secondary Investing in treatment for depression and anxiety leads to fourfold return[EB/OL].
https://www.who.int/news-room/fact-sheets/detail/depression.2016.
[20] Chio O I,Yip P K,Liu Y C,et al.Detection of cognitive impairment using self-rated AD8 and informant-reported AD8[J].J Formos Med Assoc,2018,117(1):42-47.
(收稿日期:2019-09-04) (本文编辑:程旭然)
猜你喜欢
中国典型病例大全(2022年13期)2022-05-10
中国典型病例大全(2022年7期)2022-04-22
祝您健康(2019年8期)2019-08-09
环球时报(2019-06-21)2019-06-21
养生大世界(2018年10期)2018-10-18
恋爱婚姻家庭·养生版(2018年6期)2018-08-01
瞭望东方周刊(2018年13期)2018-04-11
环球时报(2015-06-26)2015-06-26
共产党员·下(2014年9期)2014-09-18