
Successful treatment of systemic sclerosis complicated by ventricular tachycardia with a cardiac resynchronization therapydefibrillator: A case report
2020-04-25 05:00YuanYuanChenHuiYanJianHuaZhu
World Journal of Clinical Cases 2020年5期
Yuan-Yuan Chen,Hui Yan,Jian-Hua Zhu
Yuan-Yuan Chen,Hui Yan,Jian-Hua Zhu,Department of Cardiology,The First Affiliated Hospital,School of Medicine,Zhejiang University,Hangzhou 310003,Zhejiang Province,China
Abstract
BACKGROUND
Systemic sclerosis is a rare connective tissue disease characterized by localized or diffuse skin thickening and fibrosis,which usually accumulates in various organs throughout the body.Tachyarrhythmia is a common clinical manifestation of cardiovascular damage in systemic sclerosis patients.However,few studies have reported the use of catheter ablation and an implantable cardioverter defibrillator in patients with systemic sclerosis complicated by ventricular tachycardia.
CASE SUMMARY
A 39-year woman with an 11-year history of systemic sclerosis was referred to our hospital due to three syncopal episodes in the past 6 mo.The results of an electrocardiogram and a transthoracic echocardiogram revealed ventricular tachycardia and left ventricular systolic and ventricular septum segmental motion abnormalities,respectively.The results of an electrocardiogram showed a sinus rhythm with complete blockage of the left bundle branch.In light of the progressive nature of systemic sclerosis,the presence of a left bundle branch block,and the decreased ejection fraction,a cardiac resynchronization therapydefibrillator was implanted.The patient's clinical conditions improved,and at the 3-mo follow-up,the patient was free of ventricular tachycardia and all cardiac symptoms.
CONCLUSION
We report the first case of systemic sclerosis complicated by ventricular tachycardia that was successfully treated with a cardiac resynchronization therapy-defibrillator.
Key words:Systemic sclerosis;Ventricular tachycardia;Cardiac resynchronization therapy-defibrillator;Case report
INTRODUCTION
Systemic sclerosis is a rare connective tissue disease characterized by localized or diffuse skin thickening and fibrosis,which usually accumulates within various organs throughout the body.It can be classified into two subtypes: Diffuse cutaneous systemic sclerosis and limited cutaneous systemic sclerosis.Systemic sclerosis patients also present with various cardiovascular diseases,with myocardial fibrosis revealed in 80% of subjects during autopsy[1].Tachyarrhythmia is a common clinical manifestation in systemic sclerosis patients.In a previous study,24-h Holter recordings were carried out on 183 patients with systemic sclerosis.Ventricular ectopic beats were observed in 67% of the patients,and ventricular tachycardia was noticed in 7% of the patients.Most importantly,the occurrence of ventricular abnormalities has been reported to be closely associated with death[2].
CASE PRESENTATION
Chief complaints
A 39-year-old woman with a history of systemic sclerosis was admitted to our hospital for treatment following three syncopal episodes within the past 6 mo.
History of present illness
The patient's cardiac symptoms started 6 mo ago and worsened in the past 1 mo.
History of past illness
The patient was diagnosed with diffuse systemic sclerosis based on Raynaud's phenomenon and presented with pain;sclerodactyly;sclerotic changes extending from the fingers to the forearms,as well as on the face and trunk;and positive results of an anti-Scl70 antibody test and a skin biopsy at our hospital 11 years ago.Timeline of the diagnosis and treatment is shown in Table 1.The patient was well controlled by treatment with prednisone,colchicine,and hydroxychloroquine until 2017,after which her conditions progressively worsened.The results of an electrocardiogram(ECG) at rest showed a sinus rhythm with QS waves from V1 to V3,an intraventricular conduction block(QRS duration,118 ms),and a change of the ST-T wave(Figure 1A).The results of a transthoracic echocardiogram(TTE) showed left ventricular diastolic dysfunction,normal left ventricular systolic function with an ejection fraction of approximately 59%,and tachycardia.The results of coronary computed tomography angiography showed no abnormality(Figure 1B and C),whereas those of chest computed tomography showed lung nodules.The cardiothoracic ratio was 54%.In laboratory tests,the serum creatine kinase level was 323 IU/L,and the creatine kinase-muscle brain level was 31 IU/L.The erythrocyte sedimentation rate was 30 mm/h,and the cardiac troponin I level was 0.613 ng/mL.The patient's clinical conditions improved greatly after treatment with prednisone and aspirin.
Personal and family history
The patient was a farmer and had no family history of any major diseases.

Table 1 Timeline of the diagnosis and treatment
Physical examination
The patient had New York Heart Association class II cardiac status.A physical examination revealed Raynaud's phenomenon,skin tightening,waxy luster,depressed scars,escharosis of the fingertips,and a facial rash.The heart rate ranged from 60 to 90 bpm,and the blood pressure was 92/58 mmHg.On auscultation,no cardiac murmur was detected.
Laboratory examinations
Besides microcytic hypochromic anemia(hemoglobin level,110 g/L),the results of laboratory tests were normal.Antinuclear antibodies were present at a titer of 1:80,and the patient was positive for the anti-Scl-70 antibody.
Imaging examinations
The results of an ECG performed during attack revealed monomorphic wide QRS complex ventricular tachycardia with a heart rate of 186 bpm(Figure 2A and B).The results of TTE showed left ventricular systolic dysfunction with an ejection fraction of 44% and ventricular septum segmental motion abnormalities.The patient recovered from syncope by electrocardiography at a local hospital and electrocardiogram recorded sinus rhythm and left bundle branch block(LBBB)(QRS duration,143 ms)(Figure 3A).
The results of an ECG performed during hospitalization showed a sinus rhythm with complete LBBB(QRS duration,126 ms).The heart rate was 74 bpm(Figure 3B).The results of TTE showed a normal left ventricular ejection fraction(LVEF) of 58%and normal cardiac chamber size with no structural abnormality of both ventricles(Figure 4).The results of a chest X-ray showed a cardiothoracic ratio of 58%.
FINAL DIAGNOSIS
Based on these findings,the final diagnosis was ventricular tachycardia caused by systemic sclerosis.
TREATMENT
In light of the progressive nature of systemic sclerosis,the presence of LBBB,and the decreased ejection fraction,the patient was successfully treated with a cardiac resynchronization therapy-defibrillator(St.Jude Medical Unify CD3231-40) on July 25,2019.
Implantation was performed under conscious sedation.We performed sinus venography from a left anterior oblique 30° angle and obtained images of the coronary vein.The target vein was subsequently identified(Figure 5A).The leads were advanced through the guidewire towards the right atrium and both ventricles.After setting the parameters of the cardiac resynchronization therapy-defibrillator,the leads were connected to the pulse generator(Figure 5B).Bisoprolol,methylprednisolone,amiodarone,and aspirin were started after the procedure.
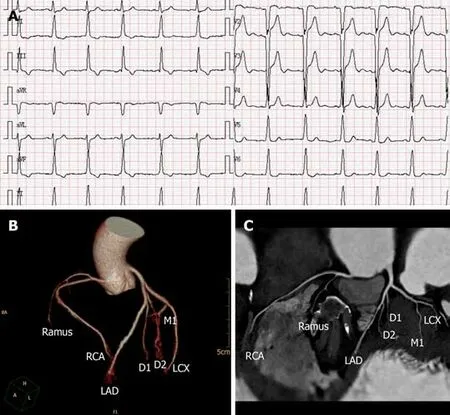
Figure 1 Electrocardiogram and coronary computed tomography angiography.
OUTCOME AND FOLLOW UP
The results of an ECG showed biventricular pacing and a reduction of the QRS complex duration by 22 ms(from 126 ms to 104 ms) after successful implantation of the cardiac resynchronization therapy-defibrillator(Figure 5C).During hospitalization,there was no syncopal episode,and the patient's clinical conditions improved greatly.
At the 3-mo follow-up,the patient reported an improvement in exercise tolerance and no cardiac symptoms(Figures 6 and 7) or ventricular tachycardia were observed.The last interrogation(October 2019) revealed a biventricular capture rate > 99%,with no ventricular tachycardia/ventricular fibrillation episodes.At the time of this writing(November 2019),the patient's clinical conditions were stable.
DISSCUSION
We describe a case of hemodynamically unstable ventricular tachycardia with an 11-year history of systemic sclerosis that was treated with a cardiac resynchronization therapy-defibrillator.To the best of our knowledge,this is the first report of sustained monomorphic ventricular tachycardia treatment with a cardiac resynchronization therapy-defibrillator.Previous reports have described the successful treatment of systemic sclerosis patients by catheter ablation and an implantable cardioverter defibrillator for ventricular tachycardia.In 1977,John and colleagues reported the first case of using a cryoprobe to ablate drug-resistant ventricular tachycardia in a systemic sclerosis patient by surgery[3].Subsequently,the first implantable cardioverter defibrillator was used to treat patients with systemic sclerosis complicated by ventricular tachycardia[4].Seven systemic sclerosis patients with sustained ventricular tachycardia were successfully treated by endocardial catheter mapping and transcatheter ablation in four studies from 1999 to 2012.At the 1-mo follow-up,only one patient died of cardiogenic shock after ablation.The remaining patients did not experience ventricular tachycardia episodes after ablation.These studies demonstrate that catheter ablation is safe and effective for systemic sclerosis patients with sustained ventricular tachycardia[5-8].Marsico and colleagues reported that tensystemic sclerosis patients with heart involvement received an implantable cardioverter defibrillator.Three out of the ten patients experienced ventricular tachycardia but recovered after electric shock.Their clinical conditions were improved at the 36-mo follow-up.Our results indicate that an implantable cardioverter defibrillator may prevent sudden cardiac death in patients with systemic sclerosis complicated by ventricular tachycardia[9].

Figure 2 Electrocardiogram.
Cardiac resynchronization therapy,which is primarily used for the treatment of patients with heart failure,can improve cardiac performance,alleviate cardiac symptoms,improve quality of life,and reduce morbidity and mortality.The highlevel recommendations for cardiac resynchronization therapy in the 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure are mainly for symptomatic patients with a QRS duration >130 ms,a LBBB QRS morphology,and an LVEF ≤ 35% despite optimal medical therapy[10].A cardiac resynchronization therapy-defibrillator was implanted for several reasons.First,our patient had a LBBB QRS morphology in the sinus rhythm and a progressive increase of the QRS duration that reached 126 ms in two years.Second,our patient complained of breathlessness,tiredness,and reduced exercise tolerance,which are typical symptoms of heart failure,and the patient had NYHA class II cardiac status.Third,the results of an ultrasound cardiogram revealed left ventricular dyssynchrony.Due to the pathological characteristics of scleroderma,it can cause myocardial fibrosis,coronary microvascular damage,and paralysis,which can eventually lead to aggravation of heart failure.
The patient was not a candidate for cardiac ablation because ventricular tachycardia was not induced.Furthermore,the results of the ECG indicated that ventricular tachycardia originated from the right ventricular apex.Due to the poor hemodynamic tolerance and very high heart rate usually reached during tachycardia,successful ablation is uncommon in cases of tachycardia.Thus,the patient was treated by cardiac resynchronization therapy after consultation with members of her family.
Although cardiac resynchronization therapy is not generally recommended for patients with a QRS duration < 130 ms,a LBBB QRS morphology,and an LVEF >35%,our patient showed improvement of symptoms and quality of life at the 3-mo follow-up,indicating that the therapy has a potential application in patients with systemic sclerosis complicated by ventricular tachycardia.Further studies are needed to evaluate the long-term complications and treatment outcomes.
CONCLUSION
In conclusion,we report the first case of systemic sclerosis complicated by ventricular tachycardia successfully treated with a cardiac resynchronization therapy defibrillator.Further studies are needed to explore the application of this therapy.

Figure 3 Electrocardiogram.

Figure 4 Echocardiogram.
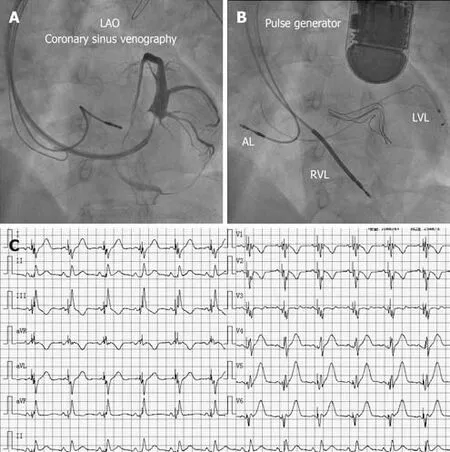
Figure 5 Coronary sinus venography and electrocardiogram.
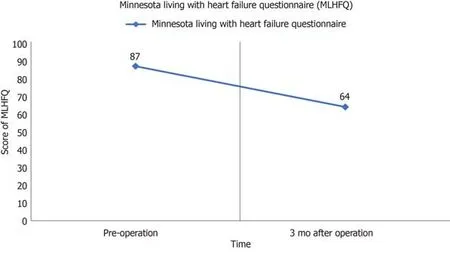
Figure 6 Minnesota living with heart failure questionnaire.
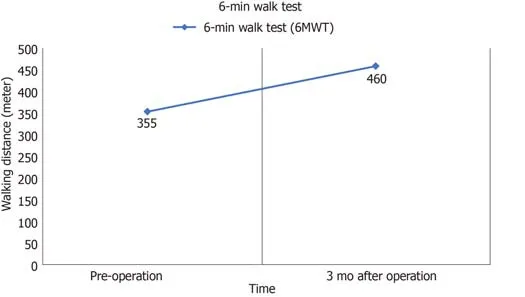
Figure 7 6-min walk test.
 World Journal of Clinical Cases2020年5期
World Journal of Clinical Cases2020年5期
- World Journal of Clinical Cases的其它文章
- Gut microbiota and nutrient interactions with skin in psoriasis: A comprehensive review of animal and human studies
- Microbiota-gut-brain axis and its affect inflammatory bowel disease:Pathophysiological concepts and insights for clinicians
- Distal esophageal spasm: Update on diagnosis and management in the era of high-resolution manometry
- Clinical course of percutaneous cholecystostomies: A crosssectional study
- Clinical characteristics and 28-d outcomes of bacterial infections in patients with hepatitis B virus-related acute-on-chronic liver failure
- Application of hybrid operating rooms for treating spinal dural arteriovenous fistula