
Using Materialise's interactive medical image control system to reconstruct a model of a patient with rectal cancer and situs inversus totalis:A case report
2020-04-22 02:19TaoChenYuTaoQueYiHaoZhangFeiYuLongYiLiXinHuangYaNanWangYanFengHuJiangYuGuoXinLi
World Journal of Clinical Cases 2020年4期
Tao Chen,Yu-Tao Que,Yi-Hao Zhang,Fei-Yu Long,Yi Li,Xin Huang,Ya-Nan Wang,Yan-Feng Hu,Jiang Yu,Guo-Xin Li
Tao Chen,Yu-Tao Que,Yi-Hao Zhang,Fei-Yu Long,Xin Huang,Ya-Nan Wang,Yan-Feng Hu,Jiang Yu,Guo-Xin Li,Department of General Surgery,Nanfang Hospital,Southern Medical University,Guangzhou 510515,Guangdong Province,China
Yi Li,Department of Radiology,Nanfang Hospital,Southern Medical University,Guangzhou 510515,Guangdong Province,China
Abstract
Key words:Rectal neoplasm;Situs inversus totalis;Laparoscopy;Three-dimensional reconstruction;Case report
INTRODUCTION
Situs inversus totalis(SIT),also termed situs inversus viscerum,is a rare congenital anatomic abnormality of the human viscera with an incidence of 0.01% to 0.1% in the normal population.The whole internal organs of SIT patients,including the heart,lungs,septum transversum,liver,spleen,stomach,and intestines,are inverted by 180 degrees to present an approximately mirror image of the anatomy of a typical person.This condition is occasionally discovered unintentionally during check-up examinations.Although this condition does not affect normal health or longevity,the recognition of this anomaly is vital to treating many diseases,especially for patients who require surgical invention[1].
To get better acquainted with the aforementioned condition,Materialise's interactive medical image control system(Mimics,Materialise Co.,Leuven,Belgium),into which the Digital Imaging and Communications in Medicine computed tomography(CT)images are put,can be used to reconstruct the three-dimensional(3D)models of target organs.This technology can visually display and accurately locate the anatomical structure,which is conducive to the formulation and implementation of the surgical program.
Timeline
This case information is organized into a timeline presented in Table 1.
CASE PRESENTATION
Chief complaints
A 68-year-old Chinese Han woman with a clear medical history was admitted to our hospital because she reported intermittent bloody stool for approximately 6 mo that had become aggravated for nearly 11 d.
History of past illness
Proximately 6 mo ago,it was found that there was bright red blood at the end of the stool with no obvious incentive for defecation.There was no chills,high fever,nausea,vomiting,abdominal pain,or diarrhea.
Personal and family history
The patient’s family history was unremarkable.

Table 1 Timeline
Physical examination upon admission
Digital rectal examination revealed that a mass was about 5 cm above the anal verge and the tip of the glove was stained with blood.A palpable encircling mass was found in the lower rectum,10-13 cm above the anal verge,on colonoscopy(Figure 1).Part of the mass was sent for biopsy and pathology confirmed the presence of moderately differentiated adenocarcinoma from a biopsy specimen(Figure 2).Chest posterioranterior radiograph(Figure 3)and electrocardiographic examination showed dextrocardia.
Laboratory examinations
The occult blood test was positive.Plasma D-dimer level was 0.81 mg/L fibrinogen equivalent unit,and potassium ion concentration in serum was 3.48 mmol/L.
Imaging examinations
Abdominopelvic contrast-enhanced CT scans revealed that a soft tissue mass,approximately 4.5 cm from the lower rectum to the anus,was irregularly infiltrated into the serous membrane.The mass was seen to protrude into the lumen,with metastatic lymph nodes detected around.CT further revealed the complete transposition of the abdominal viscera,indicating SIT(Figure 4).Magnetic resonance imaging(MRI)scans(3.0T)revealed that a soft tissue mass,approximately 70 mm from the lower rectum to the anus,was irregularly thickened(Figure 5)and was seen to protrude into the lumen.
FINAL DIAGNOSIS
Malignant rectal tumor(cT3aN2Mx),ascending colon polyp,and SIT with no absolute contraindication.
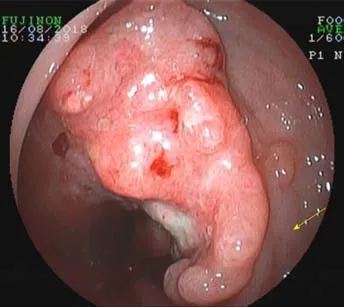
Figure 1 A palpable encircling mass was found in the lower rectum on colonoscopy(yellow arrow).
TREATMENT
No absolute surgical contraindication was found in the preoperative examinations.Before surgery,we imported the Digital Imaging and Communications in Medicine CT images into Mimics.According to the characteristic CT value range of each organ,we carried out thresholding,masking,segmentation,and boundary dressing to restore each anatomical structure,then a 3D virtual model was generated.Combined with CT images,a furthermore profound understanding of lesion and the surrounding structures of the patient was available(Figure 6).Laparoscope-assisted radical resection of rectal cancer(Figure 7)with distal ileostomy was performed successfully under general anesthesia.Postoperative pathological examination suggested differentiated colorectal adenocarcinoma invading into the full wall of the bowel.No cancer residues were found in the incised edge of either side,and the circumferential edge was 1 mm away from the tumor.The lymph nodes(LN1,LN2,and LN3)showed no metastasis of the tumor tissue(0/16,0/8,and 0/6).The postoperative condition of the patient was generally good without obvious discomfort(Figure 7).Adjuvant chemotherapy with the XELOX regimen(oxaliplatin 150 mg,D1+ Xeloda 1.0 g,Bid,D1-14)was initiated 1 mo after the operation.Assisted acidinhibiting and stomach-protecting medicine and injection of recombinant human granulocyte stimulating factor to enhance immunity were administered.
OUTCOME AND FOLLOW-UP
The patient recovered well after surgery,and her physical condition remains stable.
Mimics reconstruction
Traditionally,surgeons have used ultrasound,CT,or MRI scans to visualize and simulate the anatomy of a patient for reference.The quality of the surgical procedure depends on the surgeon's own clinical experience.Moreover,the application and promotion of laparoscopic gastrointestinal surgery are limited due to the complex structure of the peritoneal vessels and multiple anatomical variations caused by lymph node dissection.For the sake of solving the problems above,Mimics 20.0(from Materialise NV)was used to reconstruct a 3D model of abdominal organs and blood vessels of the patient through the delineation and segmentation of tissues and organs and to provide an objective basis for surgeons to design and optimize the surgical scheme.Liet al[2]provided that 3D models can better help doctors be familiar with anatomical information,develop personalized surgery plans,and reduce the learning time of young doctors on special anatomical structures.
DISCUSSION
Review of the literature
Until 2001,Bilimoriaet al[3]from the United States counted only 14 patients worldwide with all internal organs reversed complicated with malignant tumors,and none of thepatients had reported rectal cancer.So far,only three cases of rectal cancer complicated with SIT in the whole chest and abdomen have been reported in the literature;this report highlights the fourth case,as shown in Table 2.
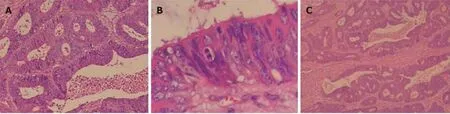
Figure 2 Pathological results.
SIT is a rare anomaly in which the abdominal and thoracic cavity structures are located opposite to their usual positions and has an incidence of 1/10000-50000 persons[4].This anomaly is not a premalignant condition.Most SIT patients can continue to live a normal life,but some may develop severe lung disease(bronchiectasis,unilateral lung defect),cardiovascular system abnormalities(ventricular septum,intra-atrial defects),and digestive system abnormalities(duodenal stenosis,atresia).The etiologic nature of this anomaly is not known.Some authors believe that this condition is related to familial genetic factors.However,other authors believe that changes in chromosome structure or number,unusual nucleotide arrangements,or mutations in DNA molecules can be the underlying cause of developmental abnormalities in embryos[7].Some experts believe that in the 4th week of embryonic development,if the intestinal loop is reversed clockwise with the supratentorial artery as the axis,or if the intestinal loop is not translocated after returning from the umbilical cord,retroversion of the abdominal situs inversus will occur[3].
Fabricius first reported cases of SIT in 1600,and the first case of SIT in China was reported by Peking Union Medical College Hospital in 1928.Due to the low incidence of SIT,patients with this abnormality and malignancy are very rare.Only nine SIT patients with laparoscopic surgery were reported[8].
This report is the first case to use 3D reconstruction with Mimics to analyze the anatomical features of a patient with both SIT and rectal cancer.The anatomical descriptions from surgery confirmed that all of the mirrored anatomical features are consistent with the 3D modeling images displayed by the system before laparoscopic surgery.Nanfang Hospital of Southern Medical University has applied laparoscopic surgical navigation based on Mimics to some routine laparoscopic surgeries for stomach cancer.This procedure is designed to reduce the risk of bleeding and abdominal organ damage during surgery that arise from limited vision and unknown anatomical features before laparoscopic surgery.
Visceral inversion in SIT patients may also be accompanied by major vascular abnormalities,which will increase the operative time and the probability of complications[9-11].Therefore,careful preoperative anatomical evaluation is very important,especially for laparoscopic surgery[6].
SIT is a rare disease,but it begins to appear more frequently,and we ought to pay more attention to it.It is necessary to share and learn about the surgical experience with this disease.Based on the above case report,we would like to provide some advice for other clinicians:3D reconstruction of the imaging result with Mimics can help to enhance the surgeon’s understanding of patients with abdominal viscera and tumor lesions,and planning and evaluation for the operation in order to reduce the operation process of anatomic abnormalities caused by unpredictable risks.Meanwhile,we could get prepared to make preoperative psychological and equipment.Less operation time would improve the perioperative safety of the patients.In addition,the 3D model can be used to visually teach and guide the operation of an entire team,in the late,for young doctors learning about rare cases.As reusable and collectable digital data,it can also be shared online,providing more learning opportunities for surgeons in every region.
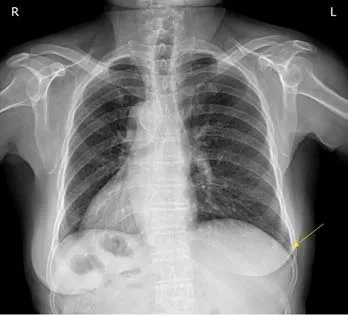
Figure 3 Chest X-ray image showing dextrocardia and a right subphrenic gastric bubble(yellow arrow).
CONCLUSION
Preoperative 3D reconstruction of the imaging results could help reduce the unknown risks during surgery caused by anatomical abnormalities and improve the perioperative safety for patients.

Table 2 List of situs inversus associated with rectal cancer
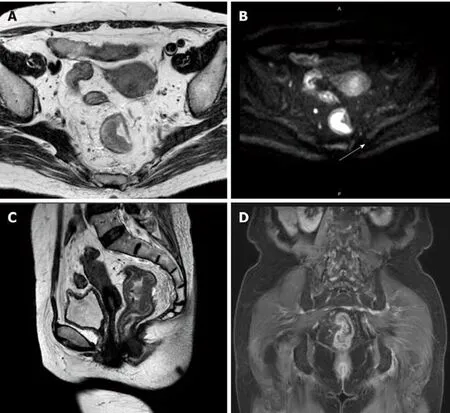
Figure 5 Pelvic magnetic resonance imaging.
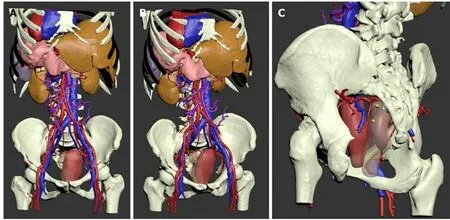
Figure 6 The three-dimensional model of abdominal organs and blood vessels of the patient.

Figure 7 Specimen.
ACKNOWLEDGEMENTS
We would like to appreciate those who devoted their efforts and time into this case,and also helpers who provided suggestions and support to us.
World Journal of Clinical Cases2020年4期
- World Journal of Clinical Cases的其它文章
- Extrapleural solitary fibrous tumor of the thyroid gland:A case report and review of literature
- Effectiveness of a microabrasion technique using 16% HCL with manual application on fluorotic teeth:A series of studies
- Prevalence and associated factors of suicide among hospitalized schizophrenic patients
- Lymphoepithelioma-like carcinoma of the upper urinary tract:A systematic review of case reports
- Delayed right coronary ostial obstruction after J-valve deployment in transcatheter aortic valve implantation:A case report
- Diverticulum of the buccal mucosa:A case report