
Application of positive behavior management in patients after breast cancer surgery
2020-04-22 02:19YingJieHaoHuiBoSunHongWeiLiBingJieChenXiuLiChenLinMaYingLiLi
World Journal of Clinical Cases 2020年4期
Ying-Jie Hao,Hui-Bo Sun,Hong-Wei Li,Bing-Jie Chen,Xiu-Li Chen,Lin Ma,Ying-Li Li
Ying-Jie Hao,Hui-Bo Sun,Hong-Wei Li,Department of Breast Surgery,the Third Affiliated Hospital of Qiqihar Medical University,Qiqihar 161000,Heilongjiang Province,China
Bing-Jie Chen,Xiu-Li Chen,Lin Ma,Department of Nursing,the Third Affiliated Hospital of Qiqihar Medical University,Qiqihar 161000,Heilongjiang Province,China
Ying-Li Li,Department of Otolaryngology,the Third Affiliated Hospital of Qiqihar Medical University,Qiqihar 161000,Heilongjiang Province,China
Abstract
Key words:Breast cancer;Cognitive intervention;Degree of hope;Self-efficacy;Negative emotions;Quality of life
INTRODUCTION
Breast cancer is a common malignant cancer.The estimated survival time of patients is short,and the average survival time is only 5-19 mo[1].In recent years,with the popularization of physical examination in China,the detection rate of breast cancer has increased annually,which has caused concern to medical personnel.Breast cancer patients have an uncomfortable cognitive experience after knowing that they have a tumor,which has an adverse effect on their quality of life[2].Positive behavior management usually refers to the subjective judgment of the individual’s current behavioral organization and execution toward the intended goal,that is,the selfconfidence of the individual’s behavior management ability[3].The higher the patient’s awareness of the disease,the stronger their ability to manage positive behavior.If the patients can adopt autonomous behaviors in the subconsciousness,they may work harder on disease management[4].The positive behavior management model based on cognitive framework intervenes in behavior and emotions that affect patient cognition,and uses multidimensional nursing methods to reverse the patient’s past misconceptions,thereby achieving physical and mental comfort,and providing preconditions for the disease to return in a benign direction[5].In terms of improving patient cognitive reserve,traditional interventions only focus on oral health education,and do not guide patients to manage their own behavior,so the intervention is less effective,and patients’ behavior cannot achieve the expected results[6].
The aim of the present study was to introduce behavioral interventions to improvetraditional interventions in order to manage the patients’ psychological and behavioral aspects together,to ensure that patients are integrated and to improve their hope for treatment and self-management,and ultimately improve quality of life[7].The study started from the perspective of random intervention and validated the clinical effects achieved by the intervention through collecting data from observational projects.
MATERIALS AND METHODS
Patients
Eighty-four patients with breast cancer who underwent surgery in our hospital from August 2016 to December 2018 were included in the study.The patients were divided into an experimental group(n= 42)and control group(n= 42)by random number table grouping.
Inclusion criteria:(1)Patients were diagnosed with breast cancer for the first time,by pathological biopsy,and the diagnosis was based on the diagnostic criteria for breast cancer developed by the International Association for the Prevention of Cancer.(2)Patients had a clear sense of consciousness and had the ability to communicate with others,and could independently complete the evaluation of the scale and questionnaire.(3)Patients’ heart,kidney and brain and other substantial organs functioned well.(4)Patients’ case data were complete.(5)Patients were accompanied by at least one immediate family member.(6)Patients had an estimated survival time of > 6 mo.And(7)Patients understood the content of the study and gave signed informed consent.
Exclusion criteria:(1)Patients had poor communication levels or barriers to understanding.(2)Patients had a primary mental illness or a family mental illness.(3)Patients were unaware or had not been informed of their condition/diagnosis.(4)Patients had concomitant malignant tumors in other areas.(5)Patients had alcohol or drug dependence.And(6)Patients were resistant to the study.
The study was reviewed and approved by the hospital ethics committee.There was no significant difference in the basic data between the two groups of patients(P>0.05,Table 1).
Control group
The control group received traditional nursing interventions.Nurses carried out the following tasks:Provided knowledge of breast cancer occurrence,development,prognosis and outcome to the patients;answer the patients’ questions and calmed the patients’ emotions;informed the patients of each pertinent care and let the patients cooperate with the nursing care;introduced the patients to the attending physician,familiarized the patients with the ward environment,adjusted the temperature and humidity of the ward according to the patients’ comfort perception;and informed the patients about the pharmacological mechanism of any drugs and possible adverse reactions.
Experimental group
The patients in the experimental group received a positive behavior management model based on cognitive framework based on the traditional intervention of the control group.
Reshape the cognitive system
Mental health guidance strategies were used to guide patients to gradually adopt the correct cognitive approach,allowing patients to gain a new perspective to examine themselves and their surroundings.After determining the research objectives,an appropriate time and place were selected to let the patients express their inner feelings,letting them vent their inner anxiety and depression,and then improve their self-image.The patients were made aware of their family responsibilities and the medical costs of their treatment.We let the patients express any fears that may occur in future social activities,corrected any misconceptions that the patients may have had from a psychological perspective,and helped them cope with their disease with a positive state of mind.We helped the patients to accept follow-up treatment and reversed any negative lifestyle.At the end of the intervention,the patients were given paper and pen to record anything from the conversation.For patients who had difficulty writing,they were able to record their thoughts on a mobile phone.The intervention lasted for 20 min,and was conducted every day from 08:00 to 09:00 h,and once a day for 2 wk.
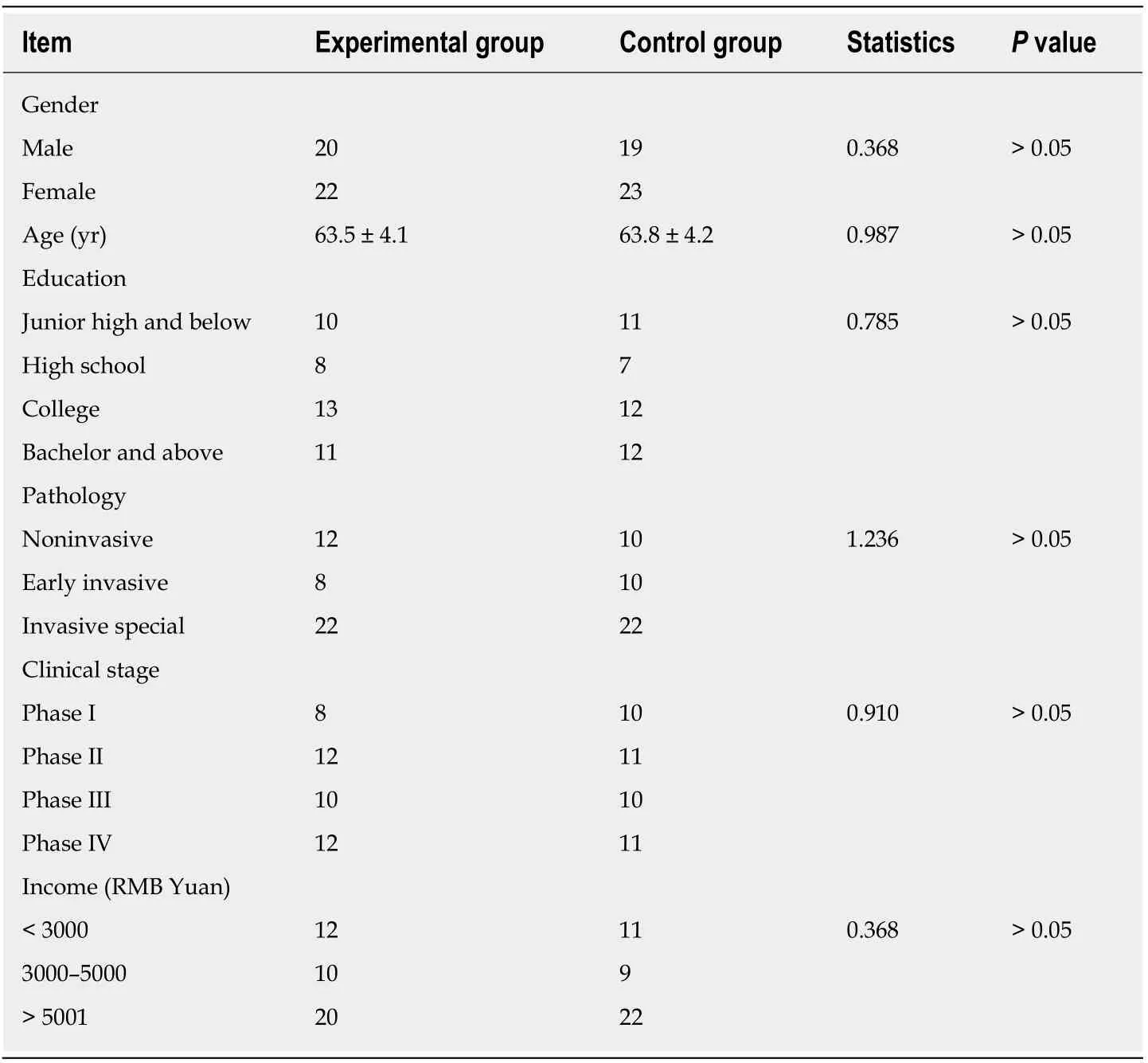
Table 1 Basic patient data
Health-related cognitive structure
Every day from 14:00 to 16:00 h,oral presentation,hand-drawn animation and video review were used alternatively according to the patients’ education level to teach them about the impact of social support,emotional status and coping behavior on physical and mental health status,in order to improve the patients’ response to disease,and encourage family members to participate in disease management.The time for the nurses’ involvement in the above three topics was restricted to 30 min,and the time spent on each topic was about 10 min.When the teaching was completed,the nurses asked the patients to objectively present the knowledge points in the form of mind map(picture combined with text),and the time was restricted to 30 min.After that,the nurse gave the patients a situational topic.You have many friends and family,how do they provide you with social support? What changes have occurred in your emotional state after receiving social support? Can you talk more about what kind of behavior you will adopt when dealing with the disease? These situational topics served as patients’ homework.The nurses asked the patients to think before going to sleep,and then answer the above three questions by mobile phone recording.From 07:00 to 08:00 h in the next morning,the nurses checked the patients’ responses and gave them encouragement to strengthen their self-confidence and courage to overcome the disease.The intervention time was limited to 90 min and took place once a day for 2 wk.
Physical and mental relaxation cognitive intervention
During the rest time each day(12:30 to 13:00 h),the patients were instructed to take a comfortable supine position,close their eyes,relax their body and mind.The intervention time was restricted to 15 min.Then,the patients were allowed to listen to some soothing music to relieve their anxiety and depression.During listening to the music,the nurses slowly told the patients about breast cancer,each sentence separated by 5 s,until all the health education content was finished.The intervention time was restricted to 10 min,and the intervention was performed once a day for 2 wk.
Family members’ participation in cognitive management
From 20:00 to 21:00 h,the nursed treated the patients and their immediate family as a common intervention group.The nurse used the relevant knowledge of the patient as the specific situation,and allowed the patients and their family to participate in roleplaying of the real situation.The specific situation involved the following:What kind of cooperative behavior should patients and their families jointly adopt during the perioperative period of breast cancer? The nurses used a mobile phone to record the role playing.The situation was limited to 30 min.The nurses recorded the strong points and deficiencies of the patients and their families,and then commented on both aspects,thus enhancing the awareness and understanding of the relevant cognitive content.The intervention time was restricted to 30 min,and the intervention was performed once a day for 2 wk.
Evaluation indicators
Self-efficacy:The self-efficacy of the two groups of patients before and 1 wk after the intervention was assessed using the General Self-Efficacy Scale(GSES).GSES was developed in 1994 by Professor Ralf Schwarzer,a renowned clinical and health psychologist at the Free University of Berlin,Germany.The scale involves 10 items,with a 4-level scale(1-4 points)with a total score of 10-40 points.The higher the score,the higher the self-efficacy.If the score is between 1 and 10,it means that the patient’s self-confidence is low;if the score is 11-20,self-confidence is relatively low;if the score is 21-30,self-confidence is higher;if the score is 31-40 points,selfconfidence is very high.The scale had a Cronbach’s α of 0.813,structural reliability of 0.793,and retest validity of 0.815.
Degree of hope:The Herth Hope Scale was used to assess the degree of hope of the two groups of patients before and 1 wk after the intervention.The Herth Hope Scale was compiled in 1992 by American scholar Herth based on Dufauft’s concept of hope.The scale involves 12 items,including three dimensions(4 items in each dimension),which are “positive attitudes towards the present and the future”,“practicing positive actions” and “keeping close relationships with others”.The scale is given a four-level score(1-4 points),with a total of 4-16 points for each dimension.The higher the score,the higher the level of hope that the disease will be cured.The scale had a Cronbach’s α of 0.806,structural reliability of 0.804,and retest validity of 0.811.
Negative emotions:The negative emotions of the two groups of patients before and 1 wk after the intervention were evaluated using the Self-Rating Anxiety Scale(SAS)and Self-Rating Depression Scale(SDS)compiled by Zung in 1978.Evaluation criteria for the two scales were:Score 50-59,mild anxiety/depression;score 60-69,moderate anxiety/depression;score > 70,severe anxiety/depression.The Cronbach’s α of the SAS scale was 0.817,structural reliability was 0.796,and retest validity was 0.803;Cronbach’s α of the SDS scale was 0.832,structural reliability was 0.799,and retest validity was 0.814.
Quality of life:The quality of life of the two groups of patients before and 1 wk after the intervention was assessed using a breast cancer patient-specific scale.The scale was developed by the European Quality of Life Collaboration in 2000 and is based on the Cancer Core Scale EORTCQLQ-30.The scale includes five dimensions,each of which has a score of 0-100.The higher the score,the higher the quality of life.The scale had a Cronbach’s α of 0.817,structural reliability of 0.792,and retest validity of 0.804.
Statistical analysis
The data were analyzed using SPSS version 22.0 software.The variables data were analyzed by paired-samplest-test;the attributes data were analyzed byχ2test;and the ranked data were analyzed by Wilcoxon rank sum test.P< 0.05 indicated that the difference was statistically significant.
RESULTS
Comparison of self-efficacy between the two groups before and after intervention
The self-efficacy of the experimental group was significantly higher than that of the control group(P< 0.05,Table 2).
Comparison of the degree of hope before and after intervention in the two groups of patients
The hope level of the experimental group was significantly higher than that of the control group(P< 0.05,Table 3).
Comparison of negative emotional scores before and after intervention in the two groups of patients

Table 2 Self-efficacy before and after intervention in the two groups of patients(cases)
The SAS and SDS scores of the experimental group were significantly lower than those of the control group(P< 0.05,Table 4).
Comparison of quality of life between the two groups before and after intervention
After the intervention,the quality of life scores of the experimental group were significantly higher than those of the control group(P< 0.05,Table 5 and Table 6).
DISCUSSION
Self-efficacy has some influence on the behavior of breast cancer patients,and urges individuals to consciously choose either a positive or negative lifestyle,and has a decisive influence on the duration of the two possible lifestyles[8-10].The stronger the self-efficacy of a breast cancer patient,the stronger they are in making an effort,and the more they can adhere to positive behaviors[11-13].When an individual encounters difficulties,some patients may have doubts about their response to the difficulties and diseases,so they may relax their efforts or face them in a lazy manner.However,for breast cancer patients with strong self-efficacy,they will face challenges through greater efforts[14-16].Cancer is a negative event and a major test for patients.Therefore,using multidimensional interventions to improve patients’ self-efficacy has important practical value for their prognosis[17,18].According to the self-efficacy theory of psychology,the individual’s self-efficacy is related to the power of the model,the experience of past success and failure,the level of inner positive emotion arousal,and speech comfort[19,20].
The positive behavior management model based on cognitive framework introduced in this study is a comprehensive management model,which aims to mobilize the inner positive power of patients from a multidimensional perspective,thus affecting their self-efficacy[21,22].First,through step-by-step health education and contextual play,breast cancer patients have a general awareness of the disease,thereby strengthening their self-care level and improving their self-confidence to overcome the disease[23,24].Furthermore,with the help of whole body muscle relaxation training,the patients release the negative effects on the body,thereby mobilizing their subconscious mind to counter the physical discomfort.In addition,self-care behavior is monitored in the form of study notes to improve cognitive level and intrinsic motivation on a realistic level.In addition,some breast cancer patients have negative emotions such as anxiety and depression because they are worried about their self-care outside the hospital[25].In this study,we used a physical and mental relaxation cognitive intervention to allow patients to memorize and digest relevant health knowledge while they were both physically and mentally relaxed,thus forming a virtuous circle[26].It has been reported[27]that when individuals are physically and mentally relaxed,they can promote synthesis and secretion of “happy hormones” such as dopamine,which enable individuals to make synaptic connections to new knowledge and strengthen the individuals’ memory of the corresponding knowledge.As the patients gradually reshape their knowledge about breast cancer,it can further strengthen the individuals’ hope for disease treatment,thus controlling their own behavior,which will help their condition to improve in a positive direction.Finally,the introduction of family members’ participatory cognitive management enables patients to obtain greater social support,which has a positive effect on individuals’ positive emotional experience.The results of our study also showed that the anxiety and depression scores of patients in the experimental group were lower than those in the control group,which indicates that maintaining a better sense of selfefficacy has a positive effect on the individuals’ positive emotional experience.In addition,family-based cognitive management is a concrete presentation of social support,which can in turn promote patients’ self-efficacy and thus achieve acontinuous cycle of positive effects[28].

Table 3 Level of hope before and after intervention in the two groups of patients(points)
Our study also compared the hope levels of the two groups of patients.The scores of “positive attitudes towards the present and the future”,“practicing positive actions” and “keeping close relationships with others” in the experimental group after intervention were higher than in the control group,indicating that the positive behavior management model based on cognitive framework may improve the level of hope.As patients become more aware of the disease,it can help them face and manage the disease with a positive attitude,and produce correct expectations for disease outcomes and prognosis[29].Interventions involving family members can also help patients gain emotional support.Since surgery will have a negative impact on the physiological and psychological state of breast cancer patients,it is more important to pay attention to the patients’ hope level in clinical practice and help them establish self-confidence to overcome the disease.As the level of hope and selfefficacy of patients improves,it can alleviate their anxiety and depression,so that they can face the diagnosis and treatment in a better physical and mental state,which helps to improve personal quality of life[30].In this study,the quality of life scores of the two groups were compared.The quality of life scores in the experimental group were higher than in the control group,which was consistent with the above analysis.
In conclusion,introduction of the positive behavior management model based on cognitive framework in patients with breast cancer surgery can enhance patients’ selfefficacy and improve their hopes for disease treatment,as well as relieve their anxiety and depression,which in turn may improve their quality of life.The positive behavior management model is worthy of further promotion in the clinic.
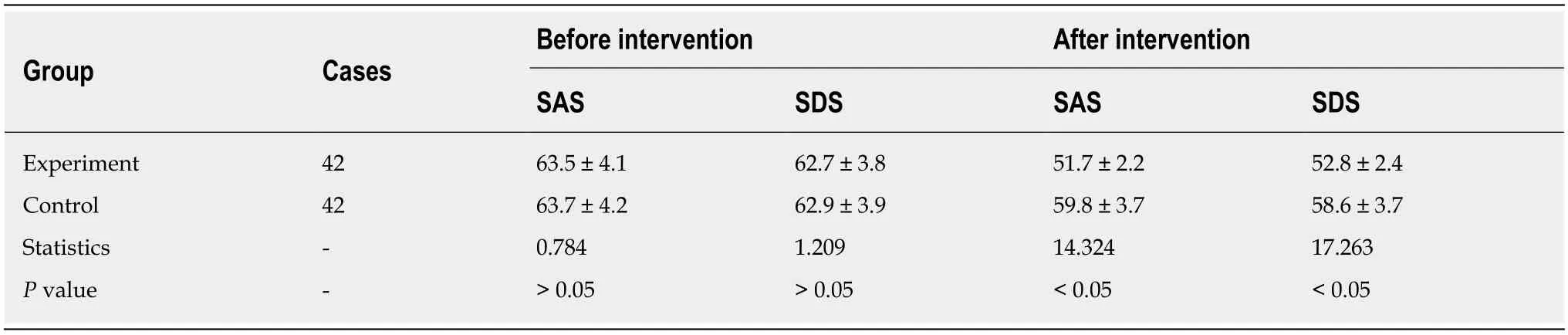
Table 4 Negative emotion scores before and after intervention in the two groups(points)

Table 5 Quality of life before intervention in the two groups of patients(cases)

Table 6 Quality of life after intervention in two groups of patients(cases)
ARTICLE HIGHLIGHTS
Research background
Although breast cancer surgery has a therapeutic effect,it has a greater psychological impact on patients,which is mainly reflected in the impact on patients' awareness of disease and selfefficacy.In order to better help patients improve their self-management effect,adopting a positive behavior management model based on cognitive architecture can effectively promote patients to cultivate a positive rehabilitation mentality,thereby promoting prognostic recovery.
Research motivation
The motivation of this study is to find a way to provide scientific and effective interventions to improve the overall rehabilitation effect of breast cancer patients,so as to promote the rapid recovery of patients and maintain their physical and mental health.The key issues to be addressed in this study are how to set up the corresponding interventions and how to determine that the interventions have the expected effect.Our article solves the above problems perfectly by formulating comprehensive intervention measures and developing objective evaluation indicators.In the future,more in-depth studies in this area should be conducted through cooperation with other medical institutions or by expanding the sample size and analyzing more detailed measurement indicators to obtain more representative conclusions.
Research objectives
The main objective of this study is to obtain the application effect data of the positive behavior management model based on cognitive architecture,and to verify its effectiveness and feasibility in clinical application.The goal that has been achieved is that the study has clearly identified that this intervention can strengthen the self-efficacy of breast cancer patients,increase their level of hope for disease treatment,and relieve their anxiety and depression,thereby improving the quality of life of individuals.This also points out the direction for future research,which can be studied in more depth or expansion,so as to achieve a wider coverage.
Research methods
The research method is mainly to implement different intervention measures for the two groups,focusing on the analysis of the role of the positive behavior management model based oncognitive architecture.The General Self-Efficacy Scale was used to evaluate self-efficacy,the Herth Hope Scale was used to evaluate hope level,the Self-rating Anxiety Scale and Self-rating Depressive Scale were used to evaluate negative emotions,and the breast cancer patient-specific scale was used to evaluate the quality of life.The characteristic and novelty of this research method lies in the fact that through the analysis of scales in different aspects,we statistically and comprehensively verify the effect of the intervention measures of the observation group,in order to provide clinical guidance.
Research results
The result of this study is that the effect and application value of the positive behavior management model based on cognitive architecture have been confirmed,thus pointing out specific directions for future interventions.The contribution of the study to its field is that it can help the clinical establishment of specific items,operational specifications and evaluation indicators of the positive behavior management model based on cognitive architecture.However,there are also some related problems,such as the need to further refine the research indicators and the evaluation schemes.
Research conclusions
The new findings of the study are the affirmation of the role and value of the positive behavior management model based on cognitive architecture,which has taken a solid step for future clinical applications.
Research perspectives
The lessons learned from this study are that continuing in-depth research and investigation can provide more substantial content for the positive behavior management model based on cognitive architecture,enrich its specific connotation,and thus make it more representative.Future research directions are mainly to expand disease adaptation,refine management models,and enrich survey methods.The best method for future research is to invite other medical institutions to conduct collaborative research,and conduct it more scientifically in the aspects of samples,indications,and so on.
ACKNOWLEDGEMENTS
We thank all medical staff who agreed to participate in this study.
World Journal of Clinical Cases2020年4期
- World Journal of Clinical Cases的其它文章
- Must pilots permanently quit flying career after treatment for colorectal cancer? - Medical waiver for Air Force pilots with colorectal cancer:Three case reports
- Prevalence and associated factors of suicide among hospitalized schizophrenic patients
- Lymphoepithelioma-like carcinoma of the upper urinary tract:A systematic review of case reports
- Extrapleural solitary fibrous tumor of the thyroid gland:A case report and review of literature
- Delayed right coronary ostial obstruction after J-valve deployment in transcatheter aortic valve implantation:A case report
- Diverticulum of the buccal mucosa:A case report