
Risk factors for postoperative sepsis in patients with gastrointestinal perforation
2020-04-22 02:19XinXuHaiChangDongZhengYaoYunZhaoZhao
World Journal of Clinical Cases 2020年4期
Xin Xu,Hai-Chang Dong,Zheng Yao,Yun-Zhao Zhao
Xin Xu,Zheng Yao,Yun-Zhao Zhao,Department of General Surgery,Jiangning Hospital,Nanjing 210002,Jiangsu Province,China
Hai-Chang Dong,Department of General Surgery,Huaihe Hospital,Kaifeng 475000,Henan Province,China
Abstract
Key words:Risk factor;Sepsis;Gastrointestinal perforation;Prevalence;Postoperative period
INTRODUCTION
Gastrointestinal perforation(GIP)is a common acute abdominal injury.It usually requires active rescue in the intensive care unit with an emergency laparotomy[1].The risk factors for GIP vary and include older age,diabetes,antecedent diverticulitis,glucocorticoid therapy,and use of nonsteroidal anti-inflammatory drugs[2-4].GIP is an indication for emergency surgery.Laparotomy and laparoscopic surgery are the most effective and important treatment methods[5,6]despite reports regarding therapeutic endoscopy and conservative treatment for GIP[7-9].
Previous studies have shown that GIP is the most common cause of sepsis in the intensive care unit[10,11].Wickelet al[12]reported that the incidence of postoperative sepsis was > 70% in patients with GIP,thus leading to severe peritonitis.Despite advances in intensive care and antibiotic treatment,the hospital mortality rate due to abdominal sepsis remains high,and the mortality due to a postoperative septic abdomen in patients with GIP can reach 50%[12-16].The definition of sepsis was revised in 2016(sepsis 3.0)to better reflect the prognosis and organ function damage rather than being defined as infection-induced systemic inflammatory response syndrome[17].Once sepsis occurs,the prognosis worsens,and few studies have focused on the risk factors for postoperative sepsis in patients with GIP.The present study was conducted to investigate these risk factors.
MATERIALS AND METHODS
Study design
This was a retrospective study performed at the Department of General Surgery in our treatment center.From January 2016 to December 2018,the medical records of patients with GIP who underwent emergency surgery were reviewed.Patients younger than 17 years or who did not undergo surgical treatment were excluded.Patients were divided into the postoperative sepsis group and the non-postoperative sepsis group.Clinical data for both groups were collected and compared,and the risk factors for postoperative sepsis were investigated.The institutional ethical committee of our hospital approved the study(No.2019110).All study participants provided informed written consent during treatment.The statistical methods used in this studywere reviewed by Doctor Ren from Henan University.
Data collection
Following admission,each patient underwent routine blood and biochemical tests.A computed tomography scan was also performed for a detailed diagnosis.After GIP was diagnosed,emergency surgery(either laparotomy or laparoscopic surgery)was performed.All patients received third-generation cephalosporins to treat the infection after admission.Data for each patient,including demographic characteristics(e.g.,age,sex,and body mass index),laboratory examination results at admission,perforation location,etiology(i.e.,trauma,malignant tumor,or benign ulcer),time interval from abdominal pain to surgery,perforation diameter,surgical procedure,and whether postoperative sepsis occurred were collected.In the present study,sepsis was defined as life-threatening organ dysfunction caused by a dysregulated host response to infection.For clinical operationalization,organ dysfunction was represented by an increase of ≥ 2 points on the Sepsis-related Organ Failure Assessment score[17].Sepsis was evaluated daily after surgery,until the patients were discharged.
Statistical analysis
All statistical analyses were performed using the SPSS,version 20.0 for Windows(IBM,Analytics,Armonk,NY,United States).A Kolmogorov-Smirnov test was performed to determine whether continuous variables conformed to a normal distribution,and then the Student’st-test(for normally distributed data)or the Mann-Whitney U test(for data that were not normally distributed)were performed.Fisher’s exact test was used to compare categorical variables.Multiple logistic regression analysis was performed to evaluate the risk factors for GIP.Odds ratios(ORs)are expressed with 95% confidence intervals(CIs).Kaplan-Meier estimates followed by a log-rank test were used to evaluate the prognoses between different groups.Pvalues< 0.05 were considered statistically significant.
RESULTS
Population and prevalence of postoperative sepsis
Two hundred twenty-six patients were admitted to our department due to GIP.Fourteen patients were excluded:Four were under 17 years old,and 10 did not undergo emergency surgery because of high surgical risk and/or disagreement with the patients and their family members.Two hundred twelve patients were finally enrolled in the study;161 were men,and 51 were women.The average age was 62.98± 15.65 years.Postoperative sepsis occurred in 48 cases.The prevalence of postoperative sepsis was 22.6%(95%CI:17.0%-28.3%).Twenty-eight patients(13.21%)died after emergency surgery.Table 1 shows the characteristics of the 212 patients.
Emergency surgical procedures
Table 2 shows the emergency surgical procedures.Of the 212 enrolled patients,169 underwent perforation repair:Seventy one of those underwent laparoscopic gastrointestinal repair,and 98 underwent standard surgical repair.Of the remaining 43 patients,11 underwent repair + ostomy(colonic repair + enterostomy),6 underwent resection and anastomosis,12 underwent resection + ostomy,and 14 underwent subtotal gastrectomy + gastrojejunostomy due to gastric malignant perforation.
Risk factors for postoperative sepsis in patients with GIP
Patients were divided into either the postoperative sepsis group(n= 48)or the nonpostoperative sepsis group(n= 164).Following univariate analysis(Table 1),16 factors differed between the two groups:Age,temperature,heart rate,mean arterial pressure,ascites incidence,serum creatinine,white blood cell counts,C-reactive protein,colonic perforation,gastric perforation,time interval from abdominal pain to emergency surgery,preoperative American Society of Anesthesiologists score,incidence of malignant tumor-related perforation,perforation diameter,perforation repair,and digestive tract reconstruction.
Multiple logistic regression analysis confirmed that the time interval from abdominal pain to emergency surgery(OR = 1.021,95%CI:1.005-1.038,P= 0.006),colonic perforation(OR = 2.761,CI:1.821-14.776,P= 0.007),perforation diameter(OR= 1.062,95%CI:1.007-1.121,P= 0.027),and incidence of malignant tumor-related perforation(OR = 5.384,95%CI:1.762-32.844,P= 0.021)were associated with postoperative sepsis(Table 3).
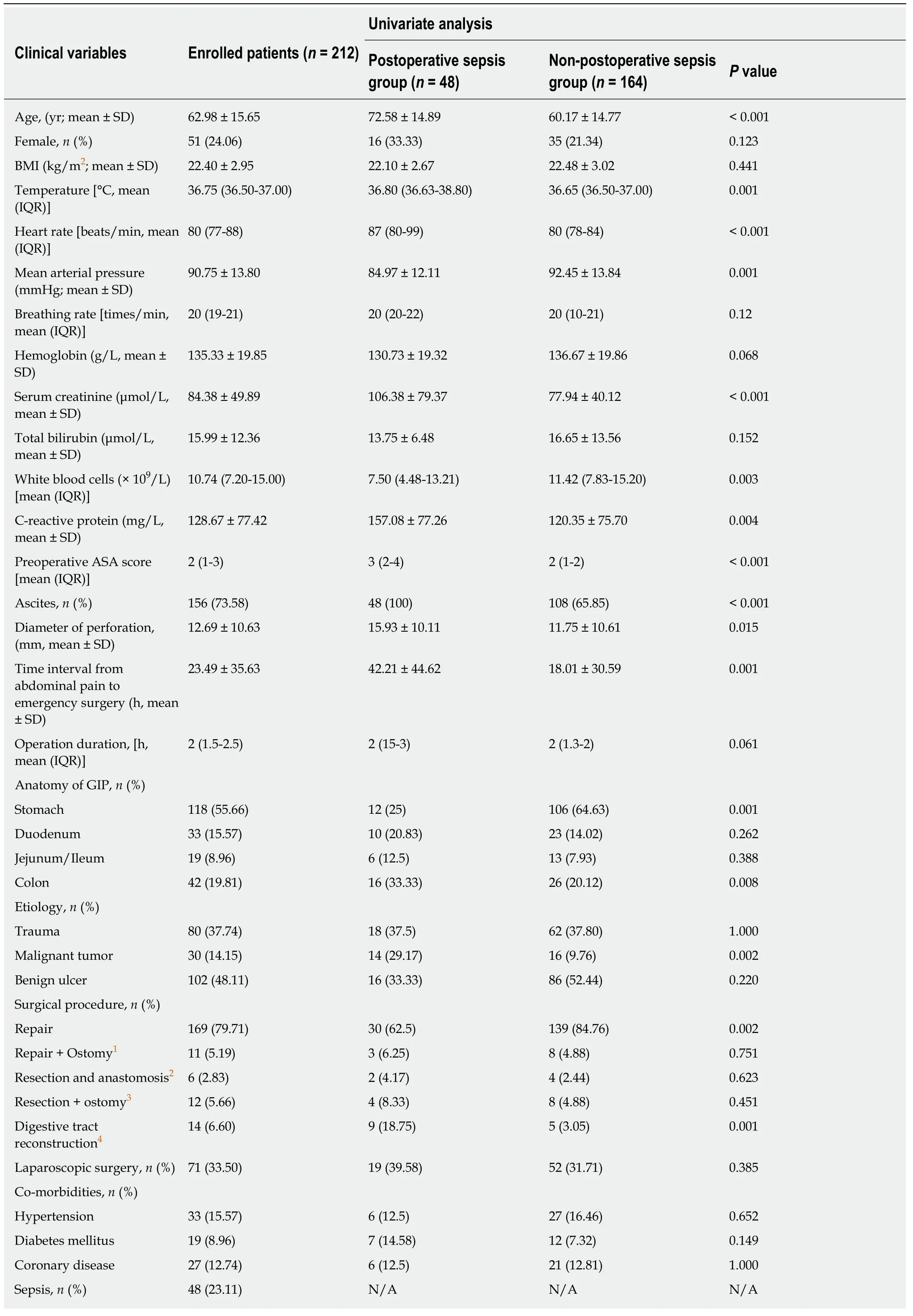
Table 1 The characteristics of the 212 patients with gastrointestinal perforation and univariate analysis for postoperative sepsis
Prognosis of patients with postoperative sepsis
The time interval from emergency surgery to sepsis was 1 d(range,1-2 d).Twentyfour patients(50%)died in the postoperative sepsis group,whereas only 4 died(2.44%)in the non-postoperative sepsis group(Table 4).Mortality was higher in the postoperative sepsis group than in the non-postoperative sepsis group(Figure 1;P<0.001).Length of stay in survivors was longer in the postoperative sepsis group than in the non-postoperative sepsis group(20.96 ± 4.97 dvs11.69 ± 2.8 d;P< 0.001).
DISCUSSION
GIP is a common but fatal acute abdominal injury.The primary method for treating GIP is emergency surgery[8,9].Prior studies showed that the incidence of sepsis due to GIP reached 20%-73%[12,14-16],and mortality due to GIP-induced sepsis was 30%-50%[12,14-16].In the present study,the incidence of sepsis was 22.6%,and the mortality due to sepsis was 50%.Although a new definition of sepsis has been introduced,mortality was not significantly increased,possibly because of the differences between participants in our study and those in previous studies.
The present study included 161 men and 51 women with GIP,with a male/female ratio of approximately 3:1.The male/female ratio was also high in other studies of GIP[16,18].Recent research on peptic ulcer perforation found an even higher male/female ratio of 10:1[14].Sivaramet al[14]found that being female was a risk factor for mortality in patients with peptic ulcer perforations.However,Sivaram’s research was focused on upper gastrointestinal ulcer perforations.Our study included jejunal/ileal and colonic perforations as well as trauma and tumor-related perforations;this may have caused the difference in the male/female ratio.
In our study,colonic perforation was associated with postoperative sepsis.The colon contains more bacteria;thus,these patients will absorb more toxins[19,20],resulting in a higher risk for postoperative complications,which has been demonstrated in many studies.The time interval from abdominal pain to emergency surgery was a risk factor for postoperative sepsis in our study.A longer interval may have caused more intestinal fluid to spill and be absorbed into the blood,possibly leading to postoperative sepsis.The occurrence of sepsis would lead to high mortality[14,15].Some studies found that a delay of more than 24 h is associated with mortality and morbidity due to GIP[15,21],thus illustrating the importance of the time interval from abdominal pain to emergency surgery.Perforation diameter is also associated with prognosis.Sivaramet al[14]revealed that perforation diameters > 1.0 cm led to poor outcomes.Taşet al[21]reported that patients with perforation diameters> 0.5 cm were at high risk for postoperative morbidity.Our research showed that the perforation diameter may be associated with postoperative sepsis,which was consistent with previous studies.
The present study also revealed that malignant tumor-related perforations may be associated with postoperative sepsis.The edges of malignant gastrointestinal ulcers are more irregular or asymmetric;folds appear more disrupted and “moth-eaten”near the crater edge and/or are clubbed or fused and more crisp or tough than benign ulcers[22].Consequently,malignant tumor-related perforations are more difficult to treat than benign ulcer-related perforations[22].In our study,30 patients had malignancy-related perforations.The operation duration was longer for patients with malignancy-related tumor perforations(3 h[3,4]vs2 h[1,2];P< 0.001).In addition,no patients with malignant tumor-related perforations underwent repair procedures.The surgical procedures included digestive tract reconstruction(gastrectomy +gastrojejunostomy,n= 14),gastrectomy(n= 4 patients with malignant gastric tumors),and resection + ostomy(n= 12 patients,9 with a partial colectomy +colostomy and 3 with a partial colectomy and anastomosis + enterostomy).Studies of damage control[23]have shown that complex surgical procedures can lead to poor prognoses.In summary,patients with malignant tumor-related perforations are more likely to experience postoperative sepsis with higher mortality rates.
大学生三观主要是指人生观、价值观以及世界观,在大学阶段大学生三观还未完全形成,对大学生进行思想政治教育主要目的是帮助大学生树立正确三观,而中国传统文化中涵盖的内容对大学生树立正确三观有积极影响。因此,在高校思想政治教育中融入中国传统文化有利于大学生树立三观。但目前我国仅有少部分高校将传统文化融入思想政治教育中,导致我国大部分大学生三观明显出现偏差,不利于其未来发展。
Our study had some limitations.First,because the study was retrospective,some selection bias existed.Second,procalcitonin was not analyzed,which might beregarded as an infection index.Third,the number of patients in the group with postoperative sepsis was very different from that in the non-postoperative sepsis group.In addition,the causes of the perforation would partially influence the surgical procedure,which may make some factors less prominent.Subgroup studies should be performed in the future.

Table 2 Emergency surgical procedures
In conclusion,the time interval from abdominal pain to emergency surgery,colonic perforation,perforation diameter,and malignant tumor-related perforation incidence were risk factors for postoperative sepsis in patients with GIP.

Table 3 Risk factors for postoperative sepsis in patients with gastrointestinal perforation

Table 4 Prognosis of patients
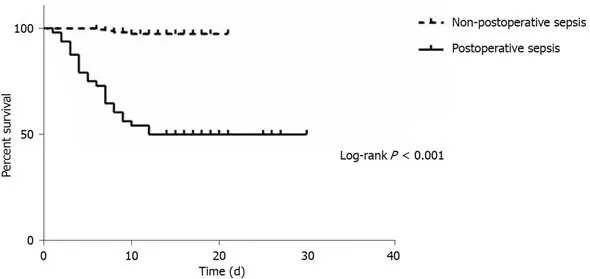
Figure 1 Kaplan-Meier estimates of survival between the postoperative sepsis group and the non-postoperative sepsis group.
ARTICLE HIGHLIGHTS
Research background
Gastrointestinal perforation(GIP)is a common acute abdominal injury.It usually requires activerescue in the intensive care unit with an emergency laparotomy.The definition of sepsis was revised in 2016(sepsis 3.0)to better reflect the prognosis and organ function damage rather than being defined as infection-induced systemic inflammatory response syndrome.Once sepsis occurs,the prognosis worsens,and few studies have focused on the risk factors for postoperative sepsis in patients with GIP.
Research motivation
In 2016,the definition of sepsis was revised.According to the revision,patients with postoperative sepsis would be at a higher risk for death.As a result,we thought an investigation of the risk factors for postoperative sepsis was very necessary.
Research objectives
This study aimed to investigate the risk factors for postoperative sepsis in patients with GIP.
Research methods
From January 2016 to December 2018,the medical records of patients with GIP,receiving emergency surgery,were retrospectively reviewed and analyzed.Risk factors for postoperative sepsis in patients with GIP were evaluated.
Research results
A total of 212 patients were eligible.The prevalence of postoperative sepsis was 22.6% [95%confidence interval(CI):17.0%-28.3%,n= 48].The time interval from abdominal pain to emergency surgery [odds ratio(OR)= 1.021,95%CI:1.005-1.038,P= 0.006],colonic perforation(OR = 2.761,CI:1.821-14.776,P= 0.007),diameter of perforation(OR = 1.062,95%CI:1.007-1.121,P= 0.027),and the incidence of malignant tumor-related perforation(OR = 5.384,95%CI:1.762-32.844,P= 0.021)were associated with postoperative sepsis.
Research conclusions
The time interval from abdominal pain to emergency surgery,colonic perforation,diameter of perforation,and the incidence of malignant tumor-related perforation were risk factors for postoperative sepsis in patients with GIP.
Research perspectives
A further study plans to include more subjects and the development of a prediction model for postoperative sepsis,in order to identify a truly accurate diagnostic method suitable for clinical use.
World Journal of Clinical Cases2020年4期
- World Journal of Clinical Cases的其它文章
- Must pilots permanently quit flying career after treatment for colorectal cancer? - Medical waiver for Air Force pilots with colorectal cancer:Three case reports
- Prevalence and associated factors of suicide among hospitalized schizophrenic patients
- Lymphoepithelioma-like carcinoma of the upper urinary tract:A systematic review of case reports
- Extrapleural solitary fibrous tumor of the thyroid gland:A case report and review of literature
- Delayed right coronary ostial obstruction after J-valve deployment in transcatheter aortic valve implantation:A case report
- Diverticulum of the buccal mucosa:A case report