
Left atrial appendage aneurysm:A case report
2020-04-09 08:07:24DmitryVladimirovichBelovVladimirIvanovichMoskalevDmitryVictorovichGarbuzenkoNikolayOlegovichArefyev
World Journal of Clinical Cases 2020年19期
Dmitry Vladimirovich Belov,Vladimir Ivanovich Moskalev,Dmitry Victorovich Garbuzenko,Nikolay Olegovich Arefyev
Dmitry Vladimirovich Belov,Department of Hospital Surgery,South Ural State Medical University,Chelyabinsk 454092,Russia
Dmitry Vladimirovich Belov,Vladimir Ivanovich Moskalev,Department of Hospital Surgery,Federal Center for Cardiovascular Surgery,Chelyabinsk 454033,Russia
Dmitry Victorovich Garbuzenko,Department of Faculty Surgery,South Ural State Medical University,Chelyabinsk 454092,Russia
Nikolay Olegovich Arefyev,Department of Pathological Anatomy and Forensic Medicine,South Ural State Medical University,Chelyabinsk 454092,Russia
Abstract BACKGROUND An aneurysm of the left atrial appendage is one of the rare but potentially hazardous heart defects.The risk of lethal complications grows with its size.To date,about 150 cases of this defect have been described in the literature.We present a case of left atrial appendage aneurysm with the deformation of the mitral valve and the left main coronary and circumflex artery,which required mitral valve annuloplasty and bifurcation stenting.CASE SUMMARY A 58-year-old man presented to our hospital complaining of shortness of breath,general weakness,dizziness during physical exertion,and fatigue.Based on the results of echocardiography,an aneurysm of the left atrium was suspected.A free-breathing real-time cine magnetic resonance imaging with electrocardiograph synchronization confirmed the diagnosis of left atrial appendage aneurysm.The patient underwent an aneurysmectomy via a median sternotomy with cardiopulmonary bypass.Intraoperative transesophageal echocardiography revealed relative mitral insufficiency that was corrected with an annuloplasty ring.Intraoperative coronary angiogram showed impaired blood flow in the left main coronary and circumflex artery and 60% stenosis.For this reason,bifurcation stenting was performed.The patient had an uneventful postoperative clinical course and was discharged from the hospital on the 10th day in a satisfactory condition.CONCLUSION Left atrial appendage aneurysm is a rare and dangerous heart pathology that requires surgery to prevent related complications.
Key Words:Atrial appendage;Aneurysm;Mitral valve insufficiency;Coronary stenosis;Catheter ablation;Case report
INTRODUCTION
Left atrial appendage aneurysm is one of the rare but potentially hazardous heart defects.The bigger it grows,the higher is the risk of lethal complications[1].The paper presents a case of left atrial appendage aneurysm that required a left atrial appendage resection and mitral valve annuloplasty.
The PubMed database,the Google Scholar retrieval system,and the reference lists from related articles were used to search for relevant publications.Articles corresponding to the aim of the review were selected for 1962 to 2019 using the keywords:“left atrial appendage aneurysm”,“left atrial appendage dilatation”,“pathogenesis”,“diagnosis”,“treatment”.The management of patients with left atrial appendage aneurysm was the inclusion criterion.
CASE PRESENTATION
Chief complaints
A 58-year old man was hospitalized to the Federal Center for Cardiovascular Surgery of the Russian Ministry of Health(Chelyabinsk)complaining of dyspnea,general weakness,dizziness during physical exertion,and fatigue.
History of present illness
Over the past five years,the patient experienced rare heart palpitations that have occurred and stopped on their own after a few minutes.Six months before hospitalization,shortness of breath,weakness,and post-exertion dizziness appeared.Heart rate increased to 120 per minute.The electrocardiogram taken in an outpatient clinic revealed an irregular form of atypical atrial flutter.Based on the results of echocardiography,an aneurysm of the left atrium was suspected.Warfarin was prescribed.The maintenance dose was 2.5 mg daily.
History of past illness
The patient had a free previous medical history.
Physical examination
On the patient’s visit to the Center for Cardiovascular Surgery,his vital signs were within normal limits.
Laboratory examinations
The Quick prothrombin activity was 27.9%(reference values were 70%-120%),INR was 2.52,and the prothrombin time was 45.6 s due to warfarin treatment.Other laboratory parameters of blood and urine analyses,blood biochemistry,and arterial blood gas were within normal limits.
Imaging examinations
A free-breathing real-time cine magnetic resonance imaging(MRI)with electrocardiograph synchronization did not reveal any defects in the leaves of the pericardium and extrapericardial protrusions of the heart cavities.A giant aneurysm of the left atrial appendage(123 mm × 90 mm × 70 mm in size)had uneven and clear contours,thin walls,and turbulent blood flow in the cavity.The aneurysm had a wide communication with the cavity of the left atrium.The neck of the aneurysm was 51 mm × 55 mm in size.The cavity of the aneurysm had no pathological formations,there were no blood clots.The aneurysmically dilated left atrial appendage was adjacent to the trunk and left branch of the pulmonary artery,to the upper and lower left pulmonary veins,and to the left atrioventricular sulcus.The lower contour of the aneurysm reached the diaphragmatic surface of the pericardium.The left atrium was of normal size(Figure 1).Preoperative coronary angiography showed the absence of coronary artery stenosis.
FINAL DIAGNOSIS
The final diagnosis of the presented case is left atrial appendage aneurysm.
TREATMENT
The operative approach wasviaa median sternotomy with cardiopulmonary bypass.Along the lateral wall of the left atrium,in the projection of the left atrial appendage,there was a pulsating,spherical,and irregularly shaped aneurysm of 10 cm × 8 cm in size.It was not adjacent to the pericardium and involved the posterior wall,reaching the left pulmonary veins ostia.
The intraoperative transesophageal echocardiography showed that the aneurysmal cavity was divided by a short septum and had free communication with the left atrial cavity.Relative mitral insufficiency requiring correction was also revealed.
The mitral valve was accessed through the right contour of the left atrium.The aneurysm of the left atrium was opened from the outside,and its base was resected.The wall of the aneurysm was thin,flabby,and without any blood clots.
In the area of the circumflex artery,the left ventricle was significantly deformed and had an indentation of 3.0 cm × 2.0 cm in size.The lower edge of the resected aneurysm was located near the fibrous annulus of the mitral valve,in the area of anterolateral commissure(A1 and P1 segments).The flaps of the mitral valve and chords were not damaged.Mitral valve annuloplasty was performed by using a PROFILE 3D®680R annuloplasty ring(Medtronic,United States).Considering that the defect,which formed after excision of the aneurysm,was close to the fibrous annulus and the circumflex artery,we decided to suture it from the inside.In the area of the fibrous annulus,the suture was fixed to the outer layer of the annuloplasty ring(Figure 2).Intraoperative transesophageal echocardiography showed grade 0–1 mitral regurgitation and insignificant mitral regurgitant volume.
Considering the anatomical location of the aneurysm and the absence of visualization of the circumflex artery,we performed coronary angiography.Signs of impaired blood flow in the left main coronary and circumflex artery and 60% stenosis were found.Bifurcation stenting was performed.
A histological examination of the resected left atrial appendage revealed a 1 mm thin wall of the left atrium with hypertrophied cardiomyocytes with dystrophic changes and vacuolated cytoplasm,and slight fibrosis of the endo- and epicardium(Figure 3).

Figure 1 Magnetic resonance imaging.A white arrow shows a sharply dilated cavity of the left atrial appendage.
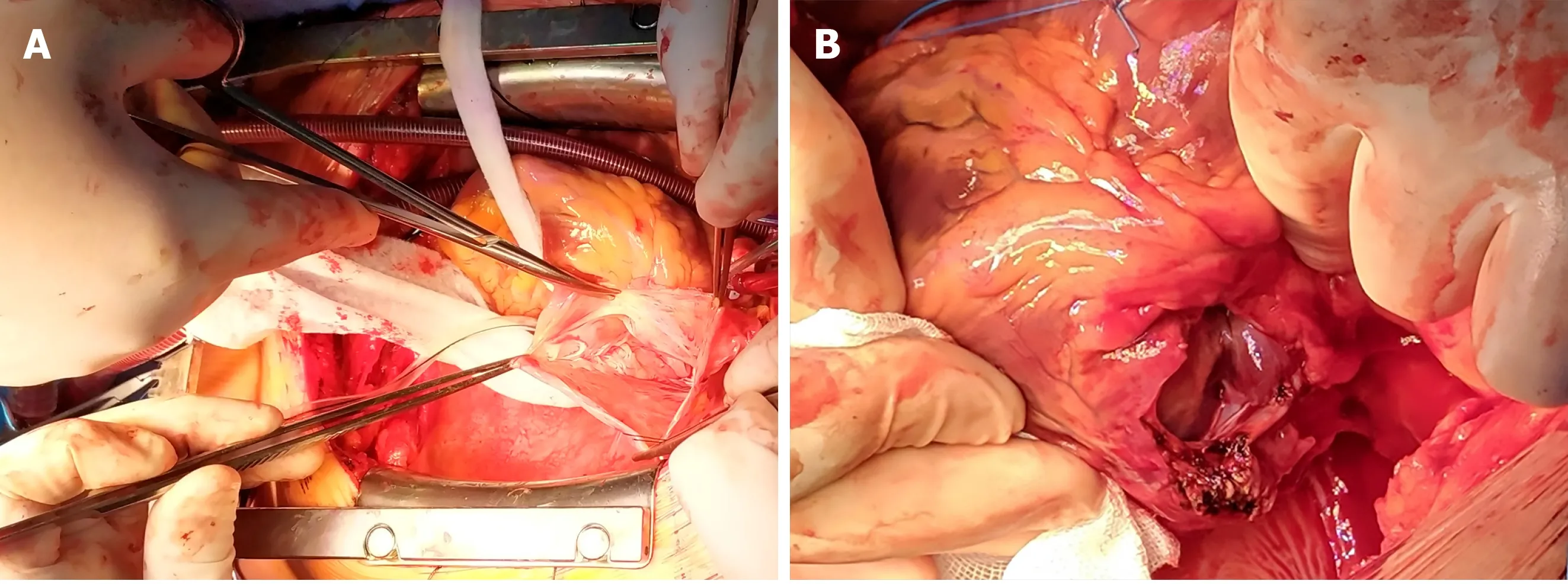
Figure 2 Aneurysmectomy.A:The aneurysm of the left atrial appendage is opened;B:The aneurysm of the left atrial appendage is excised and sutured from the inside.
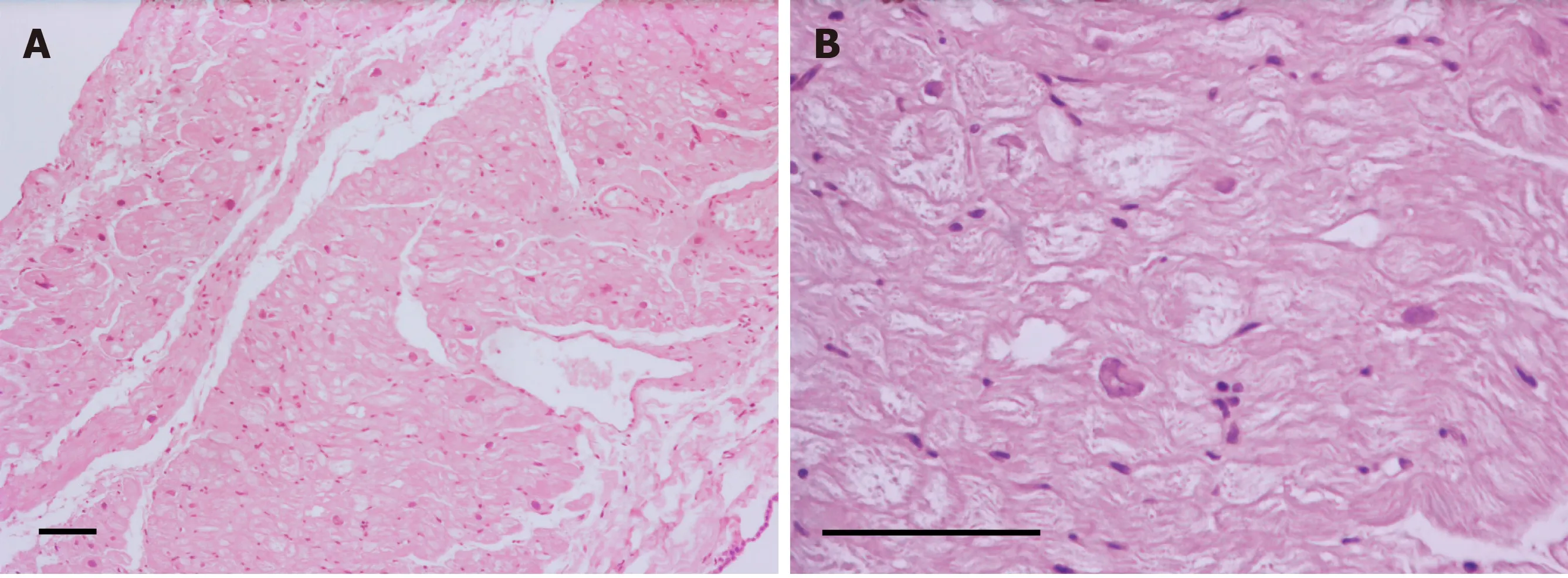
Figure 3 Hematoxylin and eosin staining of the resected left atrial appendage aneurysm.A:The wall of the aneurysm is thin,with slight fibrosis of the endo- and epicardium(scale bar 100 µm,100 × magnification);B:Hypertrophied cardiomyocytes with dystrophic changes and vacuolated cytoplasm(scale bar 100 µm,400 × magnification).
OUTCOME AND FOLLOW-UP
The patient had an uneventful postoperative clinical course and was discharged from the hospital on the 10thd in a satisfactory condition.Sinus rhythm restored in the early postoperative period.Atrial flutter reappeared 2 mo after discharge from the hospital and required surgical intervention;so,radiofrequency catheter ablation of the cavotricuspid isthmus was performed.Transthoracic echocardiography performed 3 mo after discharge showed a left ventricular systolic pressure of 29 mmHg and an ejection fraction of 60%,grade 0-1 mitral regurgitation,and insignificant mitral regurgitant volume.The left atrium was 43 mm × 53 mm in size.
DISCUSSION
In 1938,Semans and Taussig reported an isolated expansion of the cavity of the left atrium in a 5-year-old girl[2].In 1962,Parmley described aneurysmal dilatation of the left atrium appendage in two children[3].The first child of 11 years old had supraventricular cardiac arrhythmia and two episodes of systemic embolism and underwent resection of the left atrial appendage and removal of the atrial septal defect at the Mayo Clinic.The second,7-year-old patient had an aneurysm of the left atrial appendage and a concomitant congenital anomaly of the left renal artery and left kidney causing arterial hypertension.In 1963,Williams published a report on an increase in the thin-walled appendage of the left atrium in a 27-year-old man[4].An attempt to clamp the appendage during surgery was accompanied by cardiac arrhythmia;therefore,appendage resection had to be abandoned.However,due to embolic complications that occurred two years later,the removal of the left atrial appendage with blood clots was performed.To date,about 150 cases of this defect have been described in the literature[5,6].
The defect has a congenital and acquired form.In the congenital form,the formation of the aneurysm occurs due to dysplasia of the scallop muscles and associated atrial muscle fibers[5].Poor contractile function leads to a gradual expansion and extension of the left atrial appendage as a result of increased internal pressure[7].
Foaleet al[8]proposed the following diagnostic criteria for the congenital form:(1)Origin from an otherwise normal atrial chamber;(2)Well-defined communication with the atrial cavity;(3)Location within the pericardium;and(4)Distortion of the left ventricle by an aneurysm.
At the same time,Williams divided congenital aneurysms of the left atrium into extra- and intrapericardial types[4].In the extrapericardial type,the left atrium or appendage is prolated through the pericardial defect and compressed in it,which leads to the aneurysmal expansion of the extrapericardial part.The intrapericardial type is due to the underdeveloped wall of the left atrium or its appendage[9].
The process of development of acquired aneurysms is the result of damage to the mitral valve or other conditions leading to an increase in pressure in the left atrium[10].At the same time,it is often difficult to differentiate the acquired and congenital forms,as in our case,since moderate changes of the mitral valve can be caused by the presence of the appendage aneurysm itself[11].
Clinical signs of the disease occur in the third decade of life[1].The most common manifestations are heart palpitations(43%),shortness of breath(22%),heart rhythm disturbances(15%),embolic disorders of cerebral circulation(11%),and chest pain and discomfort(7%)[12].
Heart rhythm disturbances occur as a result of structural remodeling of the left atrial appendage,leading to electrical dissociation of cardiomyocytes and local disturbances in conduction that favor the emergence and maintenance of arrhythmia[13].Left atrial appendage dilatation,atrial fibrillation,blood stasis,and thrombosis of the aneurysmal cavity are responsible for subsequent thromboembolic complications[5].
Despite the large size of the aneurysm,our patient did not have any of the following symptoms associated with compression of surrounding structures:(1)Compression of the left ventricle by the aneurysm may cause an increase in filling pressure and diastolic dysfunction,leading to the appearance of shortness of breath and heart failure[13,14];(2)Compression of the left anterior descending artery may manifest as angina pectoris[15];(3)A characteristic sign of irritation of the left phrenic nerve is hiccups[6];and(4)The aneurysm proximity to the respiratory tract may cause a dry,unproductive cough[16].
Cases of left atrial appendage aneurysm rupture with a lethal outcome have been described[9].
In most cases,the disease is detected by chance because of a non-specific clinical picture.A convexity at the contour of the left atrium determined on a chest X-ray requires differential diagnosis with a pericardial cyst and heart and mediastinal tumors[10,11].
Echocardiography is considered the main method for diagnosing left atrial appendage aneurysm and the presence of blood clots in it[1].While,due to the limited echo window,the transthoracic examination does not always make it possible to accurately establish the diagnosis,the transesophageal approach may provide a more detailed and clear visualization[10].
Computed tomography and MRI are useful in unclear cases.MRI has a high resolution,which makes it optimal in assessing the surrounding structures and cardiac abnormalities.However,MRI has certain disadvantages,such as the need for regular heart rhythm and patient’s exposure to nephrotoxic contrast agents.Cardiac computed tomography makes it possible to evaluate the anatomy of the coronary arteries,if there is a suspicion of their compression,but cannot provide functional data as accurately as echocardiography or MRI[10].
Surgical treatment is indicated for all patients to prevent the occurrence of atrial fibrillation,systemic embolism,or myocardial dysfunction[17,18].We performed a left atrial appendage aneurysm resectionviamedian sternotomy with cardiopulmonary bypass,which is considered the operation of choice,especially in patients with thrombosis of the aneurysmal cavity and the need for concomitant interventions[19].
Aneurysmectomy through left-sided lateral thoracotomy should be considered if isolated lesions of the left atrial appendage are present without significant violations of the heart anatomy[20].Endoscopic surgery is most suitable for patients with minor aneurysms in the absence of thrombosis[21].
The issue of performing a concomitant intervention to restore sinus rhythm remains debatable.Following the most recent 2017 guidelines from the Society of Thoracic Surgeons,surgical ablation for atrial fibrillation is recommended at the time of concomitant mitral operations to restore sinus rhythm(Class I,Level A)[22].However,removal of the aneurysm usually results in resolution of atrial arrhythmias with no need for additional surgery[23,24].Moreover,сoncomitant atrial fibrillation surgery increases the risk for requiring a permanent pacemaker[25].We decided to abandon concomitant surgery for atrial fibrillation to limit the overall risks of the operation.Also,there was a possibility that atrial flutter might disappear after resection of the aneurysm.Unfortunately,arrhythmia disappeared only temporarily and required radiofrequency catheter ablation 2 mo after discharge from the hospital.
Limitations
This is a case report and the conclusions are subject to the inherent bias associated with the retrospective design.Also,this study design does not allow us to establish a cause-effect relationship between atrial appendage aneurysm and mitral regurgitation,as well as to differentiate between congenital and acquired forms of the aneurysm.
CONCLUSION
Left atrial appendage aneurysm is a rare heart defect.Given the nonspecific clinical picture,the disease is diagnosed either by chance or during the examination of a patient when complications arise.Echocardiography helps to establish the diagnosis in most of the cases.However,MRI is necessary for a more detailed assessment of changes in the heart.Surgical treatment is indicated for all patients to prevent fatal disorders.In the case when the circumflex artery is not visualized,coronary angiography may help to avoid adverse events.Antiarrhythmic surgery can decrease the risk of thromboembolic complications and may be performed either at the time of concomitant left atrial appendage resection or as a stand-alone surgical procedure,depending on the clinical situation.
 World Journal of Clinical Cases2020年19期
World Journal of Clinical Cases2020年19期
- World Journal of Clinical Cases的其它文章
- Parathyroid adenoma combined with a rib tumor as the primary disease:A case report
- Displacement of peritoneal end of a shunt tube to pleural cavity:A case report
- Localized primary gastric amyloidosis:Three case reports
- Bochdalek hernia masquerading as severe acute pancreatitis during the third trimester of pregnancy:A case report
- Intravesically instilled gemcitabine-induced lung injury in a patient with invasive urothelial carcinoma:A case report
- Intraosseous venous malformation of the maxilla after enucleation of a hemophilic pseudotumor:A case report