
One disease,many faces-typical and atypical presentations of SARS-CoV-2 infection-related COVID-19 disease
2020-04-08 02:55CyriacAbbyPhilipsNarainMohanRizwanAhamedSandeepKumbarSasidharanRajeshTomGeorgeMeeraMohananPhilipAugustine
World Journal of Clinical Cases 2020年18期
Cyriac Abby Philips,Narain Mohan,Rizwan Ahamed,Sandeep Kumbar,Sasidharan Rajesh,Tom George,Meera Mohanan,Philip Augustine
Cyriac Abby Philips,Narain Mohan,The Liver Unit and Monarch,Cochin Gastroenterology Group,Ernakulam Medical Center,Cochin 682025,Kerala,India
Rizwan Ahamed,Sandeep Kumbar,Philip Augustine,Gastroenterology and Advanced GI Endoscopy,Cochin Gastroenterology Group,Ernakulam Medical Center,Cochin 682025,Kerala,India
Sasidharan Rajesh,Tom George,Division of Hepatobiliary Interventional Radiology,Cochin Gastroenterology Group,Ernakulam Medical Center,Cochin 682025,Kerala,India
Meera Mohanan,Anesthesia and Critical Care,Cochin Gastroenterology Group,Ernakulam Medical Center,Cochin 682025,Kerala,India
Abstract Since the appearance of the novel coronavirus(severe acute respiratory syndrome-coronavirus-2)and related coronavirus disease 2019(COVID-19)in China in December 2019,a very high number of small and large patient series have been published in literature from around the world.Even though the classical presentation of COVID-19 is one with respiratory symptoms with or without pneumonia that can be self-limiting or evolve into severe respiratory distress syndrome with multiple organ failure,and secondary bacterial sepsis,a large body of evidence suggests a plethora of other types of clinical presentation.In this exhaustive review,we reviewed all of the published literature on COVID-19 to identify different types of clinical presentations affecting various organ systems,to provide an in-depth analysis that may prove useful for clinicians and health-workers on the frontline,battling the severe pandemic.
Key Words:Adult respiratory distress syndrome;Sepsis;COVID-19;SARS-CoV-2;World Health Organization;Centers for disease control
INTRODUCTION
In December 2019,health authorities in Wuhan,the capital of central China’s Hubei province,reported cases of “pneumonia of unknown origin”.The etiological agent was identified as a novel coronavirus(nCoV)by the Chinese Center for Disease Control on January 7,2020.The novel coronavirus was named severe acute respiratory syndromecoronavirus-2(SARS-CoV-2)by the International Committee on Taxonomy of Viruses because its clinical presentation was similar to that of the SARS virus of 2003.In February 2020,the World Health Organization(WHO)renamed the disease as coronavirus disease 2019(COVID-19),an acronym of coronavirus disease 2019.In the early weeks of March 2020,the WHO declared COVID-19 a pandemic[1,2].At the time of this manuscript preparation,a total of 2422278 cases and 165924 deaths due to COVID-19 were reported worldwide(data extracted on 20/4/2020 from www.worldometers.info/coronavirus/).The nCoV belongs to the Nidovirales order and is a single-stranded virus with a crown-like appearance due to its spiked glycoprotein envelope.The sub-family Orthocoronavirinae comprises four genera namely the α-coronavirus,β-coronavirus,δ-coronavirus and γ-coronavirus.βcoronaviruses are divided into five lineages.The A-lineage of β-coronaviruses and αcoronaviruses cause self-limiting upper respiratory tract infections,while the B-lineage(currently designated Sarbecovirus)is associated with SARS and COVID-19 pandemics.The C-lineage was responsible for the middle-east respiratory syndrome(MERS)(camel flu,caused by the MERS-CoV)of 2012.To date,including the novel SARS-CoV-2,seven coronaviruses have been identified to cause infections in humans[1-3].The nCoV is sensitive to heat and ultraviolet radiation,inactivated by lipid solvents such as chloroform and ether,and is resistant to chlorhexidine.A plausible explanation for the origin of SARS-CoV-2 is either natural selection in an animal host before the zoonotic transfer or natural selection in humans following the zoonotic transfer.Even though the first cases of COVID-19 were linked to the Huanan market in Wuhan and epidemiologists contemplate that an animal source of spread was likely present at this location this theory remains unproven.The nCoV is very similar to the bat SARS-CoV-like virus,and the likelihood of bats being reservoirs of the current pandemic is high.It was shown that the RaTG13 genome sequence isolated fromRhinolophus affinisbat species was approximately 96% identical to the SARS-CoV-2 genome.Nonetheless,the receptor-binding domain of the SARS-CoV-like virus spike protein in the bat species demonstrated divergence,which made is less efficient in binding to the human angiotensin-converting enzyme-2(ACE-2)receptor[2-4].The mechanism of nCoV infection includes requisite binding of the virus to the membranebound form of ACE-2 receptors and internalization of the complex within the host cell.In humans,the tissues that express ACE-2 receptors include that of the lung,heart,kidney,brain,and the gut.Amid discrepancy with purely bat-related mutational selection and transmission,researchers discovered genomic and evolutionary evidence on the occurrence of a SARS-CoV-2-like coronavirus in dead Malayan pangolins(called Pangolin-CoV).The discovered sequences were 91.02% and 90.55% identical to SARS-CoV-2 and Bat-CoV RaTG13,respectively,at the whole genome level.Furthermore,six key amino acid residues of the receptor-binding domain protein,involved in the interaction with human ACE-2 receptors were fully consistent between Pangolin-CoV and SARS-CoV-2.Nonetheless,four amino acid mutations were found in the bat RaTG13 genome sequence,implicating pangolins as possible natural reservoirs and intermediate mammalian hosts of the nCoV.Hence,an interplay between natural selection or mutations between bat and pangolin reservoirs and the subsequent transfer to humans may plausibly explain the emergence of the COVID-19 virus[3-6].In a population genetic analysis of 103 SARS-CoV-2 genomes,two prevalent evolutionary types of SARS-CoV-2-the L type(approximately 70%)and the S type(30%)were identified.The strains in L type,thought to be derived from the S type(a milder ancestral form),were considered evolutionarily more aggressive and contagious.Nonetheless,this study and its findings came under severe scrutiny for the lackadaisical methodology and conclusions made based on “statistical artifacts”.Experts have cautioned against the portrayal of the two-strain COVID-19 virus theory[7,8].It is believed,pending further confirmatory evidence,that human intervention might have caused severe selective pressure on the L type.Aggressive control of such host environments and activities could result in a selective increment in the S type,leading to a less aggressive disease course in subsequent infections.This could explain the phenomenon of variable death rates noted in some heavily infected populations[9](Figure 1).
GENERAL CONSIDERATIONS IN COVID-19
The average incubation period of SARS-CoV-2 is between 2 to 7 d,extending up to 24 d in some studies.The major route of human to human transmission is through respiratory droplets,and COVID-19 patients,including asymptomatic cases,remain the largest source for the spread of infection[10].The basic reproduction number or R0,which is the expected number of cases directly generated by one case in a population where all individuals are susceptible to infection in the absence of prior infection and active or passive immunization for SARS-CoV-2 is 2.2.Transmission of the virus from contaminated articles has been described,and the possibility of faecal-oral transmission exists.The latter is contemplated given detection of the SARS-CoV-2 nucleic acid in faeces and urine of infected patients[11,12].Caution regarding the possibility of transmission of the virus through conjunctival secretions and tears was put forth by certain authors but simultaneously refuted by others pending further confirmation in well-controlled large cohort studies[13].Approximately 95% of patients develop symptoms within 12.5 d of contact while others remain asymptomatic,but continue to transmit the virus and could ultimately develop symptoms after a longer duration after initial exposure[1,3,14,15].Most affected individuals are middle-aged(49 to 59 years)males,more than half of whom have an underlying chronic comorbid condition such as diabetes mellitus,systemic hypertension,chronic kidney disease,malignancy,or chronic lung disease.The case fatality rate of COVID-19 in patients with comorbid illnesses was demonstrated to be higher.The disease spectrum ranges from an asymptomatic carrier to severe respiratory failure leading to multiple organ dysfunction.However,a multitude of clinical presentations has been described.Common symptoms include fever,loss of appetite,nausea,myalgia,and arthralgia.Some authors have divided COVID-19 clinically into mild,moderate,severe,and critical stages.In the moderate stage,symptoms and signs of respiratory involvement predominate,worsening to respiratory failure in severe COVID and full-blown acute respiratory distress syndrome(ARDS)requiring mechanical ventilation and multiple organ failure requiring additional salvage support with a high likelihood of death in the critical stage[16,17].Two phases of immune responses decide the outcome of patients with COVID-19[16-18].Early in the disease,during incubation and the mild symptomatic stage,adaptive immune responses predominate.In hosts with good general health and favourable genetic predisposition(HLA status that remains undefined in SARS-CoV-2),antiviral immunity through adaptive responses promotes early recovery.In overwhelming viral replication,when adaptive immunity fails,tissue destruction in organ systems expressing ACE-2 receptors occurs.This tissue damage results in innate immunity-mediated inflammation arbitrated by macrophages and granulocytes,largely concentrated in the cardiopulmonary system that leads to life-threatening events.This cytokine release syndrome and associated poor prognosis are notable in COVID-19 patients with severe lymphocytopenia,manifested by high interleukin-6 levels.A drastic reduction in the numbers of CD4+ and CD8+ T cells and natural killer cells;a lower percentage of circulating functional monocytes,eosinophils,and basophils along with neutrophilia and an increase in neutrophil to lymphocyte ratio is seen in the innate immunity-mediated inflammatory stage of COVID-19.In patients who become refractory to aggressive medical and supportive care,upregulation of markers of immune cell exhaustion(for example,the NKG2A,on cytotoxic lymphocytes)has been demonstrated[19-21].Indeed,it has been proposed that the use of extracorporeal membrane oxygenation(ECMO)in patients with severe lymphocytopenia in the immune exhaustion phase could be deleterious since ECMO itself has been associated with a reduction in the circulating lymphocyte population[22].The diagnosis of COVID-19 requires serology confirmation,along with classic symptoms and signs.Serology can be performed on nasopharyngeal swabs or blood samples.An enzyme-linked immunosorbent assay(ELISA)or immunochromatography(card test)could be utilized.The ELISA,based on the Rp3 nucleoprotein detection of immunoglobulin M(active infection)or G(prior infection),has higher sensitivity than the card test.The latter has a more rapid turnover,but both have 100% specificity.Additionally,ELISA has high false-positive rates due to the cross-reactivity to viral nucleocapsid of other SARS viruses in the presence of shared sequence homology.Hence,ELISA specific to SARS-CoV-2 virus should ideally be towards S-protein,which is the transmembrane glycoprotein spike.The gold standard for the COVID-19 confirmatory test is the reverse-transcriptase polymerase chain reaction(RT-PCR)which has a sensitivity of approximately 90% on day one to three of infection,80% on day 4 to 6 and < 50% after two weeks of the onset of symptoms.The best sample for a good viral load yield is the bronchoalveolar lavage fluid,but getting results may take a few days compared to a few hours of turn-around-time of serologybased tests.It was shown that pharyngeal virus shedding was very high during the first week of symptoms,peaking at 7.11 × 108viral RNA copies per throat swab on the fourth day[5,23].COVID-19 can present with non-specific and sometimes surprising symptoms and signs,and hence epidemiological factors such as exposure and close contact history remain the most important tools for detection.In the following sections,we review all typical and atypical presentations of COVID-19 that are useful for clinicians caring for patients on the pandemic battle frontline.
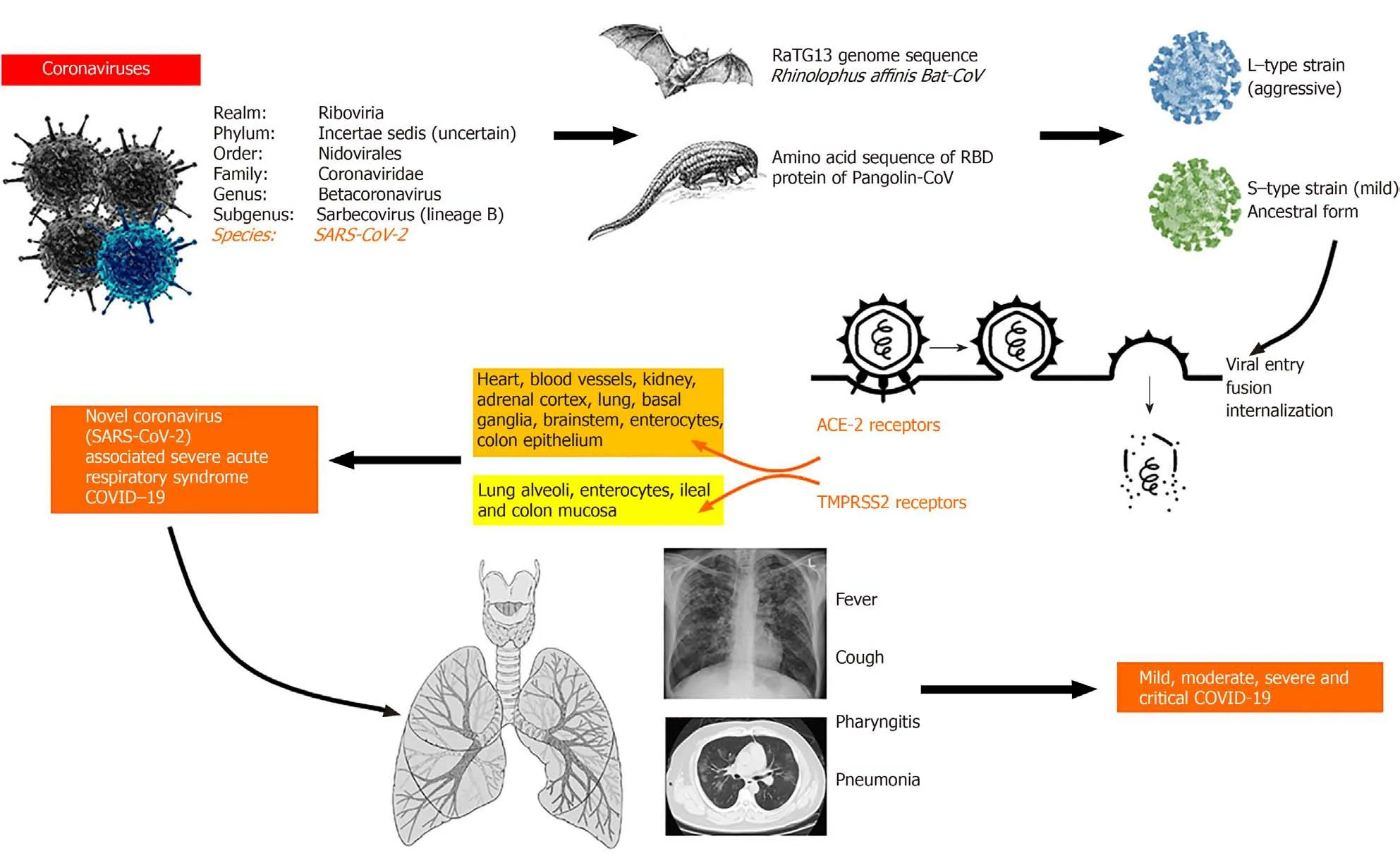
Figure 1 General considerations with regards to novel coronavirus 2019 disease.The novel coronavirus(severe acute respiratory syndrome coronavirus-2)belongs to the beta coronavirus genus and has been shown to have shared genomic sequences with bat and pangolin coronaviruses.Different strains have been controversially proposed that differ in virulence,and viral entry has been demonstrated to occur through two important receptors,namely,the angiotensinconverting enzyme-2 and the transmembrane protease serine 2 receptors present on multiple organ systems that showcase multisystem involvement and variable disease presentations.Common and typical symptoms include fever,cough and breathlessness or difficulty in breathing and can be mild,moderate,severe,or critical in its disease course[1-4,7].COVID-19:Coronavirus disease 2019;SARS-CoV-2:Severe acute respiratory syndrome-coronavirus-2;ACE-2:Angiotensin-converting enzyme-2;TMPRSS2:Transmembrane protease serine 2.
PRESENTATIONS OF COVID-19
The respiratory system
Patients with COVID-19 typically present with pharyngitis(sore throat)and dry cough along with the prodrome.Respiratory involvement can be in the form of mild upper tract symptoms and signs in the absence of pneumonia,mild pneumonia,severe pneumonia necessitating high dependency care or critical illness pneumonia requiring ventilatory support that can progress to multiple organ failure with or without superadded bacterial sepsis[24,25].Patients with mild disease have only fever and associated prodrome without respiratory symptoms even though chest signs could still be present.In moderate COVID-19 pneumonia,respiratory symptoms and signs accompany early radiological features.Progression to severe pneumonia is underscored by the occurrence of respiratory distress with a respiratory rate above 30/min,peripheral capillary oxygen saturation(SpO2)< 93% at rest,the ratio of arterial oxygen partial pressure(PaO2in mmHg)to fractional inspired oxygen(FiO2)≤300 mmHg and rapid radiological disease progression(> 50% from admission).In patients who have all of the above features along with respiratory failure needing mechanical ventilation,shock,or extrapulmonary organ failure,critical COVID-19 is diagnosed[17,18,26,27].Pneumonia in COVID-19 patients with pre-existing chronic lung disease and smokers can be catastrophic,leading to severe cardiopulmonary dysfunction and a high mortality rate.Patients can also be COVID-19 positive with detectable viral nucleic acids on RT-PCR assay but without symptoms.On the other hand,radiological changes in PCR-negative SARS-CoV-2 in the presence of virusspecific immunoglobulins G and M have been described.A small proportion of COVID-19 patients can also present with silent hypoxemia.These patients do not present with overt clinical symptoms but can develop symptoms necessitating urgent mechanical ventilation on follow-up.In this regard,some authors advise blanket oxygen saturation screening at presentation in suspected or confirmed COVID-19 cases to facilitate diagnosis and prognosis,respectively[28,29].High resolution computed tomography(CT)of the chest plays a vital role in early disease detection and evaluation.The typical findings on CT include peripherally,and sub-pleural distributed multifocal ground-glass opacities(GGOs)with patchy consolidation with a predilection for involvement of the posterior part and lower lobes of the lungs.Some patients develop bilateral multifocal consolidation that represents “crazy-pavement”appearance that,along with pleural effusion,when extensive,can demonstrate “white drowned lung”.Patients rarely present with isolated consolidation,air-bronchogram sign,reverse “halo-sign”,vascular enlargement sign,or fine reticulations on highresolution CT.According to current literature,the most common radiological presentations include GGOs,followed by GGOs with consolidation and isolated consolidation.Findings that differentiate COVID-19 pneumonia from other viral causes of pneumonia include a predominance of peripheral findings,GGOs,and,when present,reticulations with vasodilatation.Nonetheless,RT-PCR must be performed for confirmation of coronavirus pneumonia.The classical findings on chest CT imaging can also occur in asymptomatic patients.Nevertheless,cavitary lesions,calcifications,and lymphadenopathy are strikingly absent in COVID-19 lung disease[30-32].Xuet al[33]described the lung pathology in a patient who died of severe COVID-19 pneumonia.The pathological features resembled SARS and MERS infection revealing diffuse alveolar damage with cellular fibromyxoid exudates,pneumocyte desquamation,and hyaline membrane formation.The pulmonary inflammation was predominantly interstitial and dominated by lymphocytes and multinucleated syncytial cells within the intra-alveolar spaces[33].Apart from the typical lung symptoms and signs,Wanget al[34]described a PCR positive COVID-19 patient who developed spontaneous pneumomediastinum with subcutaneous emphysema that resolved uneventfully after aggressive medical management[34].
The cardiovascular system
In COVID-19,ARDS can secondarily lead to a wide range of arrhythmias,shock,and heart failure.Nonetheless,primary cardiac involvement in COVID-19 has been described recently[35].A report from Italy described the case of an otherwise healthy 53-year-old woman with PCR positive COVID-19 who presented with fever and cough.She was diagnosed with acute myopericarditis with systolic dysfunction that was confirmed on cardiac magnetic resonance(MR)imaging in the absence of respiratory involvement[36].The patient was hypotensive,and electrocardiography(ECG)showed diffuse ST-segment elevation,had increased high-sensitivity troponin T and NT-pro-BNP(N-terminal pro-brain natriuretic peptide)along with biventricular edema on MR imaging.Even though the patient improved symptomatically,the outcome was not reported.Chinese authors from Chengdu described a COVID-19 patient with fulminant myocarditis associated with pneumonia,pleural effusion,and ECG features suggestive of acute myocardial infarction.Early initiation of systemic corticosteroids along with intravenous immunoglobulins resulted in complete recovery[37].Two COVID-19 patients with ECG features of S1T3Q3 pattern with reversible nearly complete atrioventricular block and ST-segment elevation associated with multifocal ventricular tachycardia,respectively,were described by Heet al[38].While the former patient improved and was discharged to home,the second patient died in hospital.The authors proposed ACE-2 receptor-related signaling,hypoxemia,and the presence of severe systemic inflammation as important factors associated with ECG involvement in their COVID-19 patients.Sustained ventricular tachycardia or ventricular fibrillation was reported in 6% of patients at hospitalization in a study by Guoet al[39].Changet al[40]described a 49-year-old man who presented with syncope after a day of fever.At admission,an ST-segment elevation myocardial infarction was contemplated,but echocardiogram and coronary angiogram were normal.Serial ECGs were suggestive of type 2 Brugada pattern,and,in the presence of related clinical symptoms,the patient underwent coronary care unit management leading to complete recovery[40].Large series on COVID-19 patients have demonstrated evidence of acute myocardial injury(increased high-sensitive cardiac troponin I above the 99thpercentile upper reference limit),shock and non-specific and classical arrhythmias in the presence of severe lung disease,the majority of whom required intensive care management and poor clinical outcome.A patient with COVID-19 primarily presenting with cardiogenic shock due to acute cardiac injury requiring mechanical ventilation and venous-arterial ECMO who eventually died of secondary bacterial pneumonia was described by Tavazziet al[41].This was the first reported case of COVID-19 causing direct cardiac injury,underscored by the fact that endomyocardial biopsy showed low grade interstitial and endocardial inflammation along with CD68-positive macrophages and SARS-CoV-2 particles in the absence of myocyte necrosis.Ischemic and non-ischemic myocardial injury in COVID-19 was significantly associated with fatal outcomes especially in those with underlying cardiovascular disease associated with severe cardiac dysfunction and life-threatening arrhythmias and sudden death during the severe or the resolving phase of infection,in which persistent severe systemic inflammation has been proposed as the potential adverse mechanism[42].
The gastrointestinal system
Gastrointestinal symptoms are common in COVID-19(ranging from 3% to 20%)and include loss of appetite,nausea,vomiting,abdominal pain,and diarrhoea(very rarely bloody stools reported in 4% of patients in the series by Wanet al[43]),along with respiratory symptoms.Nonetheless,a group of COVID-19 patients can present with isolated diarrhoea.The SARS-CoV-2 can be detected in the faeces in about 50% of infected subjects in the absence of a clear correlation between digestive symptoms and detection of the virus in stool.Han and colleagues described a unique sub-group of COVID-19 patients with mild or no respiratory disease and lower disease severity presenting with gastrointestinal symptoms.These patients had a higher likelihood of detection of viral RNA in their faeces with longer duration for viral clearance.The onset of respiratory symptoms and fever lagged behind digestive symptoms and,in some patients,never occurred[44].Pan and colleagues showed that 18.6% of patients with COVID-19 presented with a gastrointestinal-specific symptom,including diarrhoea,vomiting,or abdominal pain,with a long time from onset to admission and diagnosis compared to those without digestive symptoms.With increasing disease severity,the gastrointestinal symptoms and signs worsened,and such patients had elevated liver enzymes,monocytopenia,and more coagulation abnormalities[45].ACE-2 receptors were highly expressed in the proximal and distal enterocytes of the small intestine.Successful viral entry depends not only on the presence of this receptor but also on the transmembrane protease serine 2(TMPRSS2)receptor,which is critical for the fusion of viral and cellular membranes.The ACE-2 and TMPRSS2 are co-expressed in the lung alveolar type 2 cells and upper esophageal epithelial lining as well as ileum and colon mucosa[46,47].Pautratet al[48]described a patient with SARS-CoV-2 infection,presenting as an appendicular syndrome(appendicitis on clinical examination without radiological evidence).However,even though the CT chest was suggestive of COVID-19,reports of RT-PCR confirmation was not reported by the authors.In patients with COVID-19,gastrointestinal symptoms are not uncommon,and CT imaging of the chest followed by RT-PCR confirmation from nasopharyngeal swabs is mandatory in the current pandemic setting.
The hepatobiliary system
The primary and direct involvement of the liver in COVID-19 has not yet been convincingly reported.The related signs of liver involvement mainly stem from secondary damage due to the disease or its treatment,and there is no clear proof that the virus causes hepatocyte damage[49].A wide range of liver test abnormalities has been identified in patients with COVID-19 and most commonly involve a rise in alanine transaminase and aspartate transaminase.These liver test abnormalities have been identified in approximately 10% to 50% of patients,depending on the study series.Hyperbilirubinaemia and an increase in prothrombin time were notable in patients with severe disease and possibly represented advanced disease associated with multiple organ failure,sepsis,drug-induced liver injury due to experimental antivirals and antibiotics and severe refractory hypoxia.Acute liver failure has not been described in SARS-CoV-2 infection[50,51].Liver histopathology of COVID-19,as describedviapost autopsy and minimally invasive post mortem biopsies,was characterized by microvesicular steatosis and non-specific lobular and portal inflammation,which could have been treatment-related,associated with the underlying comorbid condition or concomitant sepsis[52-54].In a group of patients described from the Wuhan epicenter,one patient with severe COVID-19 was found to have severe hepatitis with a maximum elevation of serum alanine transaminase of 7590 U/L,which could have been secondary to hypoxic liver injury due to critical illness.Even though the virus entry ACE-2 receptors are highly upregulated in the liver,direct organ damage due to viral replication and tissue destruction has not been demonstrated.In this regard,the hepatic involvement of COVID-19 is probably secondary to multiple organ dysfunction associated with disease progression or treatments utilized,such as the use of lopinavir and ritonavir or high dose hydroxychloroquine,or the presence of underlying chronic liver disease.Authors have suggested that COVID-19-induced hepatic damage is only a “clinical distraction”,and focus needs to be maintained on managing the patient as a whole and not based on single organ systems[55-57].Wanderet al[58]described a 59-year-old COVID-19 patient with underlying human immunodeficiency virus infection,metabolic syndrome,and Grave’s disease,primarily presenting with acute non-icteric hepatitis.The patient recovered uneventfully in the hospital[58].Huanget al[59]reported the fatal outcome of a liver transplant recipient after SARS-CoV-2 infection in whom multiple organ failure progressed rapidly.Nonetheless,primary liver involvement was not reported in this case.Clinicians caring for COVID-19 patients must evaluate liver tests at admission and closely monitor those with deteriorating liver functions,as the latter may be the harbinger of progressive respiratory disease,the beginning of multiple organ failure or an associated drug-induced liver injury.
The central nervous system
Neurological involvement among patients with COVID-19 has been reported in multiple series worldwide.Almost all of the patients were critically ill,and the symptoms and signs included confusion,diffuse corticospinal tract involvement(exaggerated tendon reflexes,clonus,and extensor plantar responses),presence of dysexecutive syndrome with inattention,disorientation,and unorganized movements.Focal signs were notably absent in these patients,and MR imaging revealed enhancement of leptomeningeal spaces,bilateral frontotemporal hypoperfusion and acute ischemic stroke features with focal hyperintensity on diffusion-weighted images.Cerebrospinal fluid analysis was non-contributory and RT-PCR for viral RNA was negative in cerebrospinal fluid samples[60,61].Neuropsychiatric manifestations evidenced by altered behaviour,dissociated and contextually flawed speech responses and psychosis have been reported in COVID-19 patients[62].Other non-specific features include headache,altered level of consciousness and dizziness that are related to the severity of systemic illness,while specific features reported were loss of sense of smell or taste,myopathy,ataxia,stroke,and convulsions.
Furthermore,a plethora of severe neurological manifestations has been described with COVID-19 critical illness,most of which are partly related to the underlying chronic comorbid condition such as cerebrovascular events-ischemic or haemorrhagic stroke,hypoxic encephalopathy and drug-induced neurotoxicity[63-66].Viral infiltration of the brain stem in patients with COVID-19 was demonstrated by Liet al[67].The first case of SARS-CoV-2 infection and associated Guillan-Barre syndrome was reported by Zhaoet al[68].In this patient,the respiratory symptoms and signs along with fever occurred at a later stage during hospitalization.Contacts of the patient also tested positive for COVID-19.Recovery was complete with the use of supportive care and intravenous immunoglobulin.A similar case was reported from Iran in which a 65-year-old male presented with rapidly progressive acute bilateral symmetric quadriparesis.He tested positive for COVID-19,and further imaging revealed bilateral GGOs and consolidation.Immunoglobulin therapy improved the patient’s outcome[69].A probable case of meningitis associated with the novel coronavirus infection was reported from Japan.The patient presented with convulsions followed by loss of consciousness.However,the authors were unable to confirm viral RNA detection on nasopharyngeal swab tests,and brain MR imaging revealed mesial temporal lobe and hippocampus hyperintensities.Serology for other viruses was non-contributory,and hence COVID-19 was made as a diagnosis of exclusion[70].A similar case of intracerebral haemorrhage in a COVID-19 patient was also reported but could have been more of an association with critical illness rather than direct causation[71].Other neurological presentations of COVID-19 reported include Miller-Fisher syndrome,polyneuritis cranialis,and acute onset encephalopathy[72,73].In summary,COVID-19 may present with meningoencephalitis features,loss of smell and taste(described in the next section),and acute inflammatory demyelinating polyneuropathy is a subgroup of patients.Other manifestations are likely to be associated with severe disease and may not be due to direct viral effect.
Oto-rhinological and ophthalmic presentations
The American Academy of Otolaryngology and the British Association of Otorhinolaryngology recommended that anosmia with or without dysgeusia be added to the list of primary screening symptoms for COVID-19 given the frequent association of these among patients reported from epicenters[74].Eliezeret al[75]described a woman in her 40 s,with COVID-19,who presented with bilateral obstructive inflammation of olfactory clefts on MR imaging,which severely impaired olfactory function[75].Olfactory dysfunction has been recognized in patients with severe disease and selfidentified by patients after a prolonged latency period.Clinicians practicing in COVID-19 red zones must be aware that acute onset loss of smell and taste in the presence of a patent nasal airway should raise a high degree of suspicion for SARSCoV-2 testing.Classic nasal cavity symptoms such as rhinorrhoea,itchy erythematous nasal cavity,and nasal congestion associated with common viral respiratory disease seldom occur in COVID-19.Hypogeusia and hyposmia in patients without prior ear,nose,or throat disorders are strong pointers toward the clinical diagnosis of COVID-19.The explanation for smell and taste dysfunction in COVID-19 is believed to be the direct virus damaging effects on gustatory receptors and olfactory mucosa.Olfactory and taste dysfunction can occur during the early or late course of the disease,and can also be the only presenting symptom that could portend severe disease in those with a prolonged disease course[76-79].Acute otitis media with otalgia and tinnitus as the sole presentation of COVID-19 in a 35-year-old woman was reported from Turkey.Audiometry revealed conductive hearing loss with a type-b appearance on tympanometry and bilateral GGOs on chest imaging[80].
Cheemaet al[81]reported a healthy young woman with COVID-19 presenting with right-sided keratoconjunctivitis and mild respiratory symptoms in the absence of fever.The conjunctival swab of the affected eye was positive for the SARS-CoV-2 virus[81].An update issued by the American Academy of Ophthalmology discussed conjunctivitis as a presenting symptom of COVID-19 in affected patients,and large series on 1099 COVID-19 patients described conjunctival congestion as an associated symptom in 0.8%[82].In the study by Wuet al[83],31.6% of COVID-19 patients had ocular manifestations in the form of conjunctivitis with conjunctival hyperemia,chemosis,epiphora,or excessive secretions.Univariate analysis of patients with ocular manifestations demonstrated a higher likelihood of leucocytosis,raised procalcitonin,C-reactive protein level and lactate dehydrogenase compared to those without eye symptoms.Nonetheless,Seahet al[84]showed that the risk of SARS-CoV-2 transmission through tears was probably low.Guoet al[85]also described the reduced potential of SARS-CoV-2 transmission through conjunctival secretions as detectable viral load in the conjunctival sac of affected patients was very low in the absence of strong evidence for local site replication[85].In COVID-19,the eye symptoms and signs are rare associations and even rarer index or presenting manifestations of the disease.
Venous thromboembolism in COVID-19
Mounting evidence from multiple countries suggests that SARS-CoV-2 infection has the potential to promote hypercoagulability at the local and systemic levels,even leading to instances of stroke in young persons.In severe progressive disease,this coagulation profile switches to one of disseminated intravascular coagulation,a harbinger of death.A middle-aged woman with COVID-19 who presented with severe pulmonary embolism with a clot in the patent foramen ovale was reported from France.Emergency embolectomy and extracorporeal life support failed to save the patient.Retrospective CT evaluation revealed multiple GGOs in both lungs[86].In the absence of other classical respiratory or gastrointestinal symptoms,acute presentations linked to the thrombogenic state could be a presentation of COVID-19.An underlying thrombophilic state,with frequent pulmonary embolisms,was reported among SARS patients at necropsy[87].Caseyet al[88]described a 42-year-old man with COVID-19,who presented with acute shortness of breath,severe chest pain,and hemoptysis.CT angiography of the chest showed bilateral segmental pulmonary emboli with areas of consolidation of the right lower lobe.Anticoagulation and oxygen therapy improved symptoms,and patients were eventually discharged to home[88].In severe COVID-19,it is presumed that local disseminated intravascular coagulation expressed in the lungs leads to activation of pulmonary thrombosis in the presence or absence of pneumonia followed by fibrinolysis activation and severe systemic inflammatory state[89].Dolhnikoffet al[90]performed ultrasound-based minimally invasive autopsies on sample tissues from several organs in patients dying of COVID-19.They identified exudative and proliferative diffuse alveolar damage associated with epithelial viral cytopathic effects involving the alveoli and small airway epithelium along with lymphocytic infiltration.Multiple areas of fibrinous thrombi in small pulmonary arterioles in damaged and preserved lung areas were notable in 80% of patients.This was associated with endothelial tumefaction associated with the packing of pulmonary megakaryocytes within pulmonary capillaries[90].Wanget al[91]found that patients at high risk of venous thromboembolism were older,required intensive unit admission,mechanical ventilation and had abnormal liver tests associated with higher levels of Creactive protein.Zhanget al[92]reported three patients with COVID-19 in whom the disease course was complicated with coagulopathy and secondary antiphospholipid antibodies associated with a critical illness.In one patient,peripheral ischemia of upper limb digits and bilateral cerebral infarcts in multiple vascular territories evolved,complicating recovery.Similar to Ebola,cytomegalovirus,and the SARS virus,SARS-CoV-2 has the potential to induce severe thrombotic phenomena at the local sites and systemic circulation.Identifying COVID-19 patients at high risk of thromboembolism is important for the initiation of prophylactic support that could prevent sudden clinical deterioration[93,94].
Dermatological presentations
In a cohort of COVID-19 patients in Lombardy,Italy,20.4% were found to develop cutaneous manifestations not related to drug use or other treatment interventions.These included erythematous rash,widespread urticaria,and zoster-like vesicles.Trunk involvement was predominant,and itching seldom reported.The authors did not find any apparent correlation of dermatological manifestations with the disease severity[95].In a report from Spain,a 32-year-old female with COVID-19 was found to develop an urticarial rash six days after the onset of respiratory symptoms.However,she had received hydroxychloroquine and azithromycin for four days before the onset of rash.The skin biopsy revealed a perivascular infiltrate of lymphocytes,some eosinophils,and upper dermal edema.The rash resolved in five days after antihistamine treatment[96].In a large cohort of patients from China,only two out of 1099 were found to have skin lesions[82].Similarly,another report from Spain described a young woman who presented at 14-d of COVID-19 diagnosis with pruritic,confluent erythematous-yellowish papules of both heels,which evolved into intense itchy erythematous plaques with thickening[97].A report from France described pruritic disseminated erythematous plaques(urticarial)of the face with acral involvement preceding classic respiratory symptoms in a COVID-19 patient[98].Bouazizet al[99]described vascular skin lesions in COVID-19 patients.These included violaceous macules with “porcelain-like” appearance,livedo reticularis-like cutaneous eruption,non-necrotic and necrotic purpura and chilblain-like lesions with or without Raynaud’s phenomenon as well as eruptive cherry angioma[99].Mahéet al[100]described an older woman who developed an erythematous rash of both antecubital fossae extending to the axillary folds and trunk after a period of loss of appetite and asthenia.Dermatology evaluation confirmed symmetrical drug-related intertriginous and flexural exanthema even though drug history was non-contributory.CT imaging of the chest showed bilateral GGOs,and RT-PCR for SARS-CoV-2 was positive.Complete resolution of symptoms occurred over three weeks[100].In summary,even though rare,a small sub-group of COVID-19 patients can present with cutaneous manifestations akin to viral exanthem or urticaria.Nonetheless,cutaneous manifestations due to drug intake should be carefully excluded.The presence of dermatological manifestations in COVID-19 does not relate to disease severity or to clinical outcomes.
Miscellaneous clinical presentations associated with COVID-19
Direct kidney involvement is very rare,and any renal dysfunction associated with COVID-19 relates to the severity and onset of critical illness.Acute kidney injury can occur as part of drug therapy,severe systemic inflammation,multiple organ failure associated with severe ARDS,secondary bacterial sepsis and cardiogenic shock[101].Larsenet al[102]described an African-American woman with stable chronic kidney disease who developed collapsing glomerulopathy after COVID-19.The patient presented with fever,cough,vomiting,and flank pain,which progressed to confusion along with advanced azotaemia and oliguria requiring mechanical ventilation and renal replacement therapy leading to complete recovery after a prolonged hospital stay.The SARS-CoV-2 nucleoprotein antigen was positive in a renal biopsy specimen,but in-situ hybridization analysis for the virus failed to show evidence of viral RNA in the kidney sample,suggesting the absence of direct renal involvement.In a previous series,post-mortem kidney biopsy in COVID-19 patients has typically demonstrated acute tubular injury without glomerulopathy[103].Other anecdotal clinical presentations of COVID-19 reported in the literature include a form of abdominal pain syndrome with severe testicular pain,vaso-occlusive crisis with acute chest syndrome in sicklecell disease,and possible immune thrombocytopenic purpura and leucoerythroblastic reactions[104-107].A hyperinflammatory systemic disease akin to Kawasaki disease including shock syndrome and macrophage activation among children with COVID-19,has been reported from multiple centers[108,109].A summary of the protean clinical manifestations of COVID-19 is shown in Figure 2.
CONCLUSION
The COVID-19 infection due to SARS-CoV-2 typically presents with acute onset respiratory symptoms with or without associated prodrome such as headache,lethargy,anorexia,diarrhoea,and arthralgia.Cardiovascular manifestations are usually related to underlying chronic comorbid conditions and the severity of infections.Nonetheless,rare presentations in the form of electrocardiographic abnormalities and myocarditis leading to cardiac failure require consideration.Gastrointestinal and hepatic manifestations are mostly therapy-related or associated with disease severity and critical illness.Anosmia and hypogeusia are typical and may occur without other classical features.Rare presentations include dermatological and thromboembolic phenomena as well as central and peripheral nervous system involvement,even though the latter is more common with multisystem involvement of COVID-19.
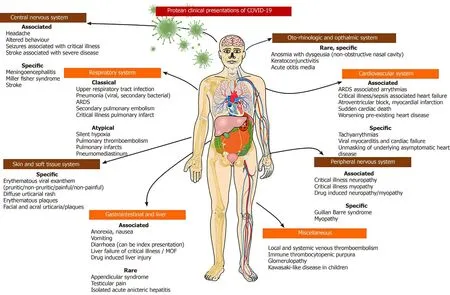
Figure 2 Summary of different clinical presentations and organ system involvement of coronavirus 2019 disease.Overall,multisystem involvement is due to the severity of the disease,but certain specific symptoms and signs can provide valuable clues towards a clinical diagnosis of coronavirus 2019 disease,which has to be confirmed on polymerase chain reaction studies from nasopharyngeal swabs.COVID-19:Coronavirus disease 2019.
 World Journal of Clinical Cases2020年18期
World Journal of Clinical Cases2020年18期
- World Journal of Clinical Cases的其它文章
- Special features of SARS-CoV-2 in daily practice
- Gastrointestinal insights during the COVID-19 epidemic
- From infections to autoimmunity:Diagnostic challenges in common variable immunodeficiency
- Application of artificial neural networks in detection and diagnosis of gastrointestinal and liver tumors
- Hepatic epithelioid hemangioendothelioma:Update on diagnosis and therapy
- Streptococcus agalactiae:Identification methods,antimicrobial susceptibility,and resistance genes in pregnant women