
Pancreatic cancer with ovarian metastases: A case report and review of the literature
2020-04-07 08:49ShunDaWangLiangZhuHuanWenWuMengHuaDaiYuPeiZhao
World Journal of Clinical Cases 2020年21期
Shun-Da Wang, Liang Zhu, Huan-Wen Wu, Meng-Hua Dai, Yu-Pei Zhao
Shun-Da Wang, Meng-Hua Dai, Yu-Pei Zhao, Department of General Surgery, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing 100730, China
Liang Zhu, Department of Radiology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing 100730, China
Huan-Wen Wu, Department of Pathology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing 100730, China
Abstract BACKGROUND Pancreatic cancer with ovarian metastases is rare and easily misdiagnosed. Most patients are first diagnosed with ovarian cancer. We report a rare case of ovarian metastases secondary to pancreatic adenocarcinoma. We also review the literature to analyze the clinical characteristics of, diagnostic methods for, and perioperative management strategies for this rare malignancy.CASE SUMMARY A 48-year-old woman with an abdominal mass presented to our hospital.Computed tomography revealed lesions in the pancreas and lower abdomen.Radiological examination and histological investigation of biopsy specimens revealed either an ovarian metastasis from a pancreatic neoplasm or two primary tumors, with metastasis strongly suspected. The patient simultaneously underwent distal pancreatectomy plus splenectomy by a general surgeon and salpingo-oophorectomy with hysterectomy by a gynecologist. Histological examination of the surgical specimen revealed a pancreatic adenocarcinoma(intermediate differentiation, mucinous) and a metastatic mucinous adenocarcinoma in the ovary.CONCLUSION For this rare tumor, surgical resection is the most effective treatment, and the final diagnosis depends on tumor pathology.
Key Words: Pancreas; Ovary; Pancreatic cancer; Ovarian cancer; Metastasis; Case report
INTRODUCTION
Pancreatic cancer (PC) is the fourth leading cause of cancer-related death and has a dismal prognosis. Approximately 20% of patients who present with local disease may show long-term survival, and only radical operation can be an optimal treatment to improve the prognosis[1]. PC tends to metastasize through the lymphoid system to organs such as the lung, liver, bone, and spleen[2]. However, PC with ovarian metastases is rare. PC that has metastasized to the ovaries is found in 4%-6% of patients during autopsy, but it is rarely diagnosed clinically[3-5]. Patients with an ovarian metastasis generally have no distinguishing clinical symptoms or signs[6-8].Since PC is easy to misdiagnose in clinical practice, the accuracy of clinical diagnoses,reasonable therapeutic methods, perioperative management, and overall survival in those with PC are unclear. Herein, we report a case of PC with ovarian metastases and review previously reported cases.
CASE PRESENTATION
Chief complaints
A 48-year-old woman was admitted to our hospital because of a palpable mass in the lower abdomen.
History of present illness
She denied the presence of abdominal pain, abdominal distention, diarrhea, or dyspepsia without weight loss. Her appetite was not affected.
History of past illness
She denied any history of hypertension, coronary heart disease, diabetes, or coronary heart disease. She reported no history of smoking, alcohol intake, or a hereditary disorder.
Physical examination
Abdominal examination showed that her abdomen was diffusely soft, with no distention or tenderness. No other positive sign was observed.
Laboratory examinations
Upon admission, her routine blood test results and blood biochemical parameters were normal. Her serum carbohydrate antigen (CA) 19-9 level was 251 U/mL, and her serum CA125 level was 412 U/mL. The levels of other tumor markers, including CA242, carcinoembryonic antigen (CEA), alpha-fetoprotein (AFP), and CA724, were within the normal ranges.
Imaging examinations
Abdominal enhanced computed tomography (CT) revealed a low-density lesion measuring 5.9 cm × 4.6 cm with a poorly defined margin and an irregular contour in the tail of the pancreas. The lesion was hypo-enhanced in the pancreatic parenchyma phase, with progressive delayed enhancement; this possibly indicated a pancreatic tumor (Figure 1). Additionally, a cystic-solid mass measuring 15.1 cm × 12.0 cm in the right ovary and a cystic mass measuring 5.7 cm × 4.3 cm in the left ovary were detected in the pelvic cavity. Both masses were thin-walled and had multiple enhancing septa. There was no evidence of liver or peritoneal metastases (Figure 2).
Diagnostic work-up
The initial diagnosis was uncertain, but the focus was on pancreatic or ovarian cancer.Therefore, she underwent fine-needle biopsy of lesions after a consultation of doctors.Endoscopic ultrasound-guided fine needle (22 gauge) biopsies of the lesion in the pancreatic tail revealed that there was an infiltrative heterogenic glandular growth in the fibrous tissue. And the ultrasound-guided biopsy of the ovary indicated the mass was likely to be metastatic. Immunohistochemistry showed the following findings:CK20 (+), CK7 (+), CDX2 (-), ER (-), and PR (-). The multidisciplinary team considered this pancreatic tumor to be possibly resectable or borderline resectable with ovarian metastases.
FINAL DIAGNOSIS
A provisional diagnosis of PC with ovarian metastases was made.
TREATMENT
The patient underwent surgeries performed by doctors from the Department of General Surgery and Gynecology. She underwent distal pancreatectomy plus splenectomy as well as salpingo-oophorectomy with hysterectomy. In addition, the appendix and omentum were removed. During the surgery, a mass measuring 4 cm ×3.5 cm was observed in the tail of the pancreas and the hilum of the spleen (Figure 3).It had invaded the spleen parenchyma. Immunohistochemical examination of the pancreatic tumor revealed the following results: CEA (-), CK20 (+), CK7 (+), p53 (-),CA125 (+), and CDX (+). Postoperative pathology revealed the pancreatic mass to be a pancreatic adenocarcinoma (intermediate differentiation, mucinous), and the ovarian masses were correspondingly diagnosed as metastases from the pancreatic mucinous adenocarcinoma. The metastatic cystic-solid mass in the ovary was found to contain many mucinous cysts and a solid component that was gray-pink in color and gel like in consistency (Figure 3). The immunohistochemical characteristics of the ovarian tumor were as follows: CDX2 (-), CK20 (+), CK7 (+), CEA (+), EMA (+), ER (-), PR (-),p53 (-), and CA125 (-) (Figure 4).
OUTCOME AND FOLLOW-UP
She had an uneventful recovery after surgery, and her postoperative hospital stay was 13 d long. Postoperative chemotherapy was advised; however, the patient’s intestinal function was significantly inhibited after chemotherapy, and she did not receive any subsequent chemotherapy. Ultimately, the patient died after 3.5 mo of follow-up.
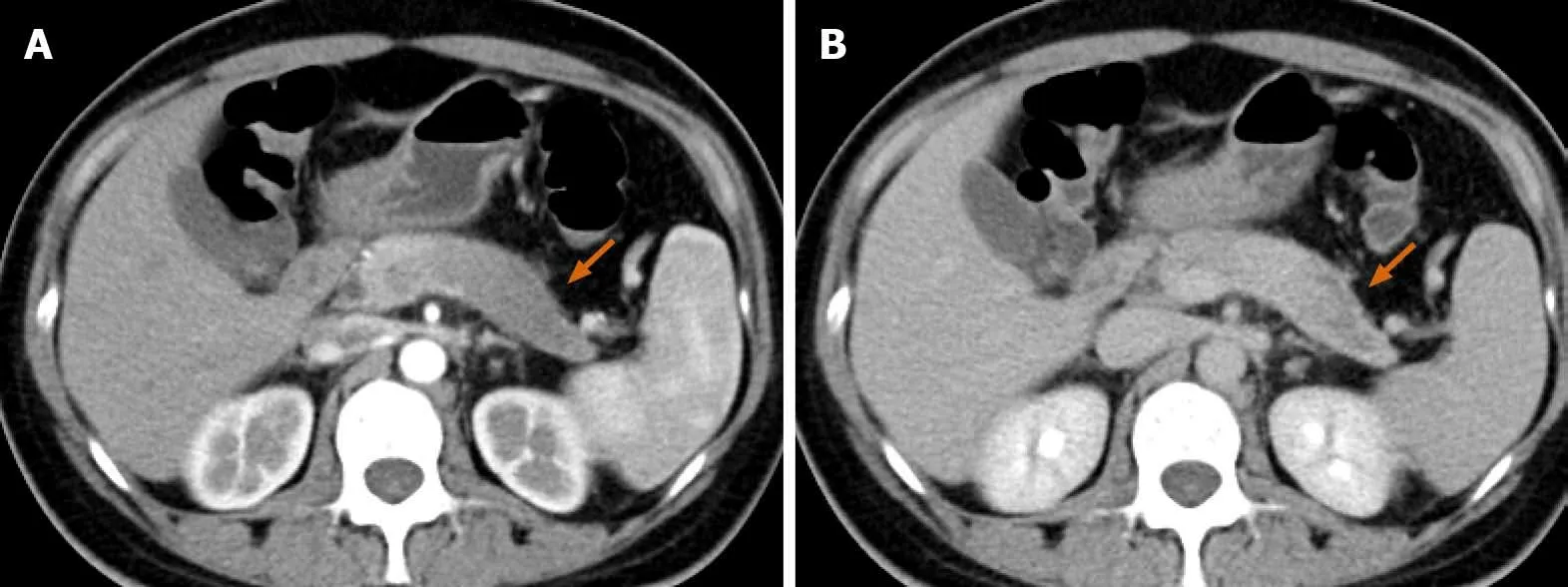
Figure 1 Change in the contour of the pancreatic body and tail, with the effacement of lobules. A: The lesion is hypo-enhanced in the pancreatic parenchyma phase (orange arrow), with progressive delayed enhancement; B: Internal necrosis is seen in the delayed phase.
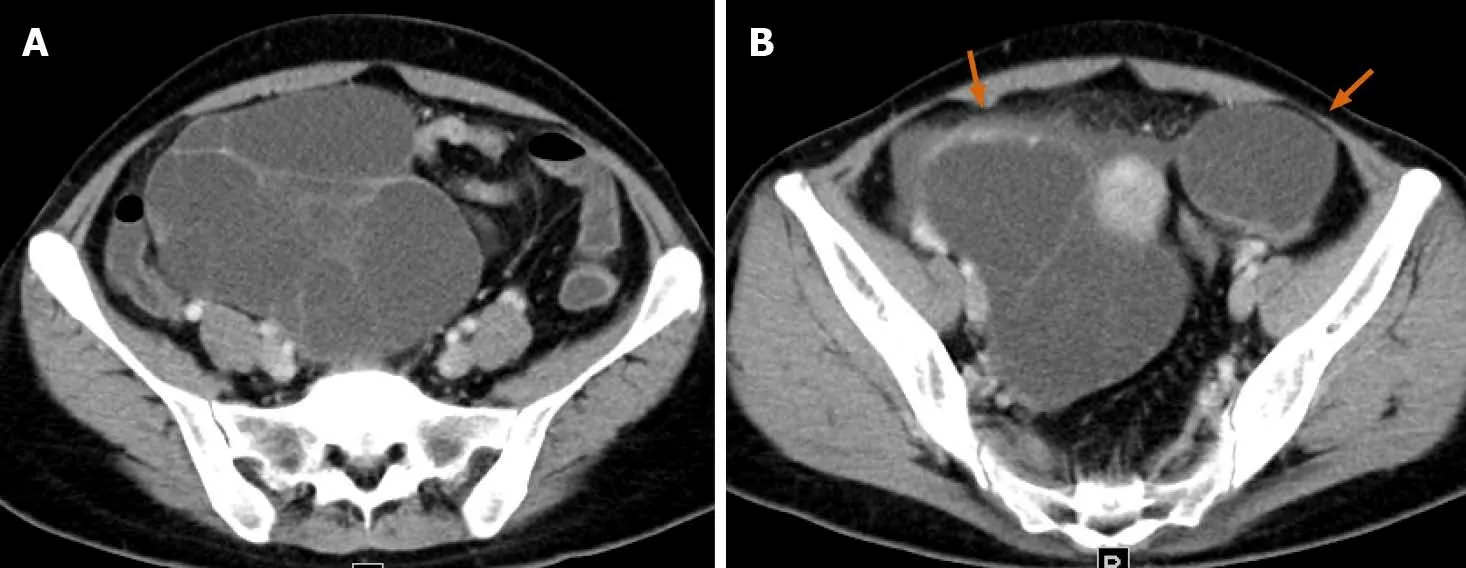
Figure 2 Bilateral cystic masses in the pelvis alongside the uterus. The masses measure 15.1 cm × 12.0 cm and 5.7 cm × 4.3 cm (A and B,respectively). Both are thin-walled with multiple enhancing septa (orange arrow). There is no evidence of liver or peritoneal metastases.
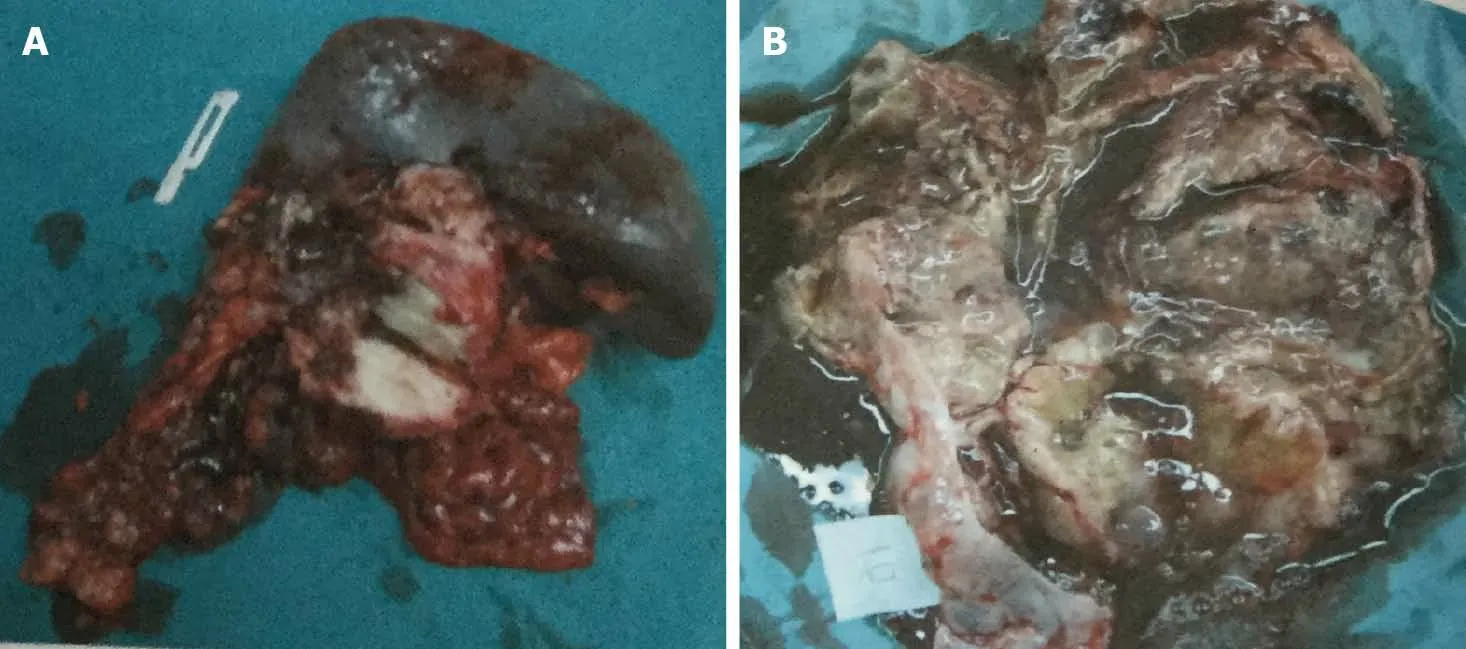
Figure 3 Specimens of the ovarian mass and distal pancreas with spleen. A: An ovarian metastatic mass with a cystic-solid profile contains many mucinous cysts; B: A pale solid mass sized 4 cm × 3.5 cm is seen at the tail of the pancreas.
DISCUSSION
PC with ovarian metastases has seldom been reported. To investigate this rare disease,we systematically searched the literature databases up till 2020. The keywords used were “Pancreatic carcinoma/cancer/adenocarcinoma,” “ovarian carcinoma/cancer,”“ovarian metastasis,” and “ovary.” In addition, the reference list of each paper was also analyzed. The inclusion criteria were any form of publication focusing on PC with ovarian metastases and a sufficient description of clinicopathological characteristics.Studies published in languages other than English, those with duplicate data from the same patient, and those for which the full text was unavailable were excluded.
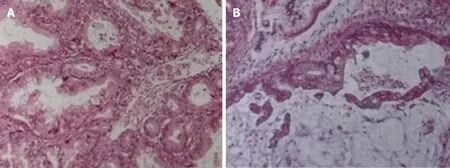
Figure 4 Histopathological analysis of the resected tumors. A: Pancreatic tumor; B: Ovarian mass.
The systematic search yielded five studies comprising 31 patients[4,9-12]. The patient in our article was the 32ndreported case. Our case report was the only one that reported the complete pathology and immunohistochemistry results for both the pancreatic and ovarian lesions. The characteristics of all cases are summarized in Table 1. The summary and analysis of the clinicopathological characteristics from these cases should provide a comprehensive description for surgeons and gynecologists.
Metastatic ovarian cancers secondary to gastrointestinal cancer are called Krukenberg tumors; an ovarian metastasis from PC presenting as a Krukenberg tumor is rare[7,13]. Ovarian tumors usually dominate the clinical presentation[3]. Ovarian metastases commonly originate from malignant tumors of the stomach, breast,colorectum, appendix, and cervix. However, metastases from PC to the ovaries are rare[3,10,14-16]. PC as the primary cancer accounted for an estimated 7% of cases of nongenital ovarian metastasis[4,7]. Among these cases, patient age ranged from 24 to 83 years. The major complaints were abdominal pain and abdominal masses. In some case reports, there was a lack of description of symptoms. We deduced that some of the abnormalities might have been discovered incidentally during physical examinations.
PCs that initially present as ovarian metastases are very difficult to diagnose. In many cases, patients were diagnosed with ovarian neoplasms with lower abdominal symptoms, which would distract from an accurate examination by doctors. Twentyone patients in our review were classified to have an ovarian tumor at the initial presentation. Only five patients were diagnosed with a primary pancreatic mass at the initial hospital admission. In almost 50% of cases, PC and ovarian metastases were found simultaneously. Many patients were first admitted into the gynecology department, were prepared to undergo a gynecological operation, and were then diagnosed with primary PC during the preoperative examination or intraoperative exploration. Currently, the combination between gynecology and general Surgery departments is important. Surgery should be contemplated only after multidisciplinary discussion.
Clinically, doctors might tend to pay attention only to pancreatic neoplasms or ovarian lesions. Without enhanced CT of the whole abdomen and pelvis, this tendency can often lead to misdiagnosis. Positron-emission tomography-CT remains the best method for identifying metastatic lesions, but it is expensive and not included in routine examinations. Currently, serum biomarkers are highly valuable. CA 19-9 is commonly used to identify PC. Unfortunately, most of the published reports lacked data on biomarkers. Another effective diagnostic method is endoscopic ultrasonography, which was applied to clinical practice three decades ago[17]. And endoscopic ultrasonography plus fine-needle aspiration was introduced to distinguish primary from metastatic tumors although with a suboptimal accuracy[18]. In our case,the ultrasound-guided biopsy exerted an important role in pre-operative diagnosis.Nowadays, the value of endoscopic ultrasonography for the differential diagnosis of various pancreatic lesions (malignant, low-grade malignant, and benign) has been widely depicted[18-21].
The primary tumor was mostly located in the body and tail of the pancreas (20 cases in our review). The metastatic path of PC to the ovary is similar to that for the Krukenberg tumor[22]and is closely correlated with lymphatic metastasis. For infiltrative tumors in the body or tail of the pancreas, cells enter the lymphatic refluxsystem of the retroperitoneum. These cancer cells can cause mechanical blockage of the lower abdominal lymphatic vessels, resulting in retrograde lymphatic flow. The cancer cells can migrate to the pelvic lymph nodes, resulting in ovarian metastases[23]. In addition, tumors invading the pancreatic capsule could also fall into the pelvic cavity.Furthermore, PCs metastasizing to the ovaries often lead to bilateral ovarian metastases; microscopic examination sometimes reveals cancer emboli in lymphatic vessels[23-26].

Table 1 Clinical features of pancreatic cancer with ovarian metastasis (32 cases)

NG: Not given.
The optimal treatment for PC with ovarian metastases is complete resection of lesions. Even with unresectable PC, resection of the ovarian metastasis is still necessary since it can effectively relieve the clinical symptoms. After palliative resection of the ovarian metastasis, some patients can achieve a relatively satisfying chemotherapeutic effect[9]. Among the 32 patients, 20 underwent salpingooophorectomy and 6 underwent hysterectomy. However, only five patients had the opportunity to undergo pancreatectomy. It is unclear whether resection of the primary lesion can prolong survival; currently, no reliable indicators are available, and thus,this requires further investigation. In addition, only 14 patients received chemotherapy. Postoperative chemotherapy is generally considered to improve prognosis. However, the prognosis could not be predicted in most cases. Our patient died 3.5 mo after the operation; thus far, only four patients have survived for > 2 years,as reported by Marcoet al[11]and Falchooket al[9].
Most of the cases involved ductal adenocarcinoma, and eight cases involved mucinous adenocarcinoma, which is partially similar to the finding reported by Petruet al[27]. Patients were misdiagnosed with primary ovarian mucinous carcinomas by many pathologists, because PC can produce large metastatic, multicystic, ovarian tumors that appear similar to primary ovarian mucinous neoplasms[3]. Ovarian metastases are characterized by multiple cysts containing mucoid material and an external surface lobulated with small gray to yellow nodules. Usually, less than 3% of primary ovarian carcinomas are mucinous, and most of those are unilateral and present as stage I disease at diagnosis.
Our review also shows that 20 cases involved bilateral ovarian metastases. If the ovarian lesion is of the mucinous type, this may suggest that it originates from a nonovarian primary tumor[28,29]. In addition to morphological features, immunohistochemical staining may help distinguish primary ovarian cancers and metastatic ovarian tumors[22,30-33]. Many pancreatic and ovarian carcinomas are positive for CK7 and show variable expression of CK20[34,35]. It was also reported that the combination of MUC5ac positivity/WT-1 negativity was seen in PC, whereas the combination of MUC5ac negativity/WT-1 positivity was seen in ovarian carcinoma[36]. However, no immunohistochemical marker alone can be used to specifically differentiate primary ovarian neoplasms from metastatic ovarian mucinous neoplasms; no reliable diagnostic criteria have yet been established. With the advances in the fields of genomics and proteomics, we hope that the molecular profiling of PC and ovarian metastases can reveal the underlying molecular mechanisms and identify reliable diagnostic biomarkers.
CONCLUSION
In clinical practice, PCs with ovarian metastases are rare and difficult to diagnose;surgical opportunities tend to be missed in these patients. They are easily misdiagnosed as primary ovarian carcinomas. The resection of any metastases from PC is strongly recommended.
 World Journal of Clinical Cases2020年21期
World Journal of Clinical Cases2020年21期
- World Journal of Clinical Cases的其它文章
- Strategies and challenges in the treatment of chronic venous leg ulcers
- Peripheral nerve tumors of the hand: Clinical features, diagnosis,and treatment
- Treatment strategies for gastric cancer during the COVID-19 pandemic
- Oncological impact of different distal ureter managements during radical nephroureterectomy for primary upper urinary tract urothelial carcinoma
- Clinical characteristics and survival of patients with normal-sized ovarian carcinoma syndrome: Retrospective analysis of a single institution 10-year experiment
- Assessment of load-sharing thoracolumbar injury: A modified scoring system