
Targeting molecular pathways for the treatment of inherited retinal degeneration
2020-03-25 10:22MeltemKutluerLiHuangValeriaMarigo
中国神经再生研究(英文版) 2020年10期
Meltem Kutluer, Li Huang, Valeria Marigo
Department of Life Sciences, University of Modena and Reggio Emilia, Modena, Italy
Funding: This work was supported by grants from the Telethon Foundation (GGP14180, GGP19113) and the European Union (LSHGCT-2005-512036 and transMed, MSCA-ITN-2017-765441) (all to VM).
Abstract Inherited retinal degeneration is a major cause of incurable blindness characterized by loss of retinal photoreceptor cells. Inherited retinal degeneration is characterized by high genetic and phenotypic heterogeneity with several genes mutated in patients affected by these genetic diseases. The high genetic heterogeneity of these diseases hampers the development of effective therapeutic interventions for the cure of a large cohort of patients. Common cell demise mechanisms can be envisioned as targets to treat patients regardless the specific mutation. One of these targets is the increase of intracellular calcium ions,that has been detected in several murine models of inherited retinal degeneration. Recently, neurotrophic factors that favor the efflux of calcium ions to concentrations below toxic levels have been identified as promising molecules that should be evaluated as new treatments for retinal degeneration. Here, we discuss therapeutic options for inherited retinal degeneration and we will focus on neuroprotective approaches, such as the neuroprotective activity of the Pigment epithelium-derived factor. The characterization of specific targets for neuroprotection opens new perspectives together with many questions that require deep analyses to take advantage of this knowledge and develop new therapeutic approaches. We believe that minimizing cell demise by neuroprotection may represent a promising treatment strategy for retinal degeneration.
Key Words: achromatopsia; calcium; calpains; calpastatin; congenital stationary night blindness; Leber’s congenital amaurosis; retinitis pigmentosa; stargardt disease
In troduction
Inherited retinal degeneration (IRD) is a group of diseases characterized by progressive loss of photoreceptor cells which affects vision and ultimately leads to complete blindness (Broadgate et al., 2017). The complexity of genetic variations in this group of diseases demands for gene-independent therapeutic strategies and requires a strong collaboration among ophthalmologists, geneticists and biotechnologists (Wubben et al., 2019). The pathophysiological events occurring at the subcellular and molecular levels in the degenerating photoreceptors have been partially characterized and represent possible targets for neuroprotective therapeutic strategies. Specifically, Ca2+overloads have been recently identified as harmful events at early stages of photoreceptor degeneration. Interestingly, increased intracellular Ca2+was detected in animal models caused by mutations in different genes, identifying high intracellular Ca2+as a common mechanism during the degeneration process(Power et al., 2019). A rationale for developing neuroprotective approaches can be the treatment with either calcium pump blockers or molecules able to boost calcium pumps favoring the extrusion of the ion from the photoreceptor cell (Frasson et al., 1999; Comitato et al., 2018). The topic of this review is the discussion of recent characterizations of the molecular events activated during photoreceptor degeneration and how these molecules can be targeted by neuroprotective approaches.
Search Strategy and Selection Criteria
The databases used to select the most relevant papers included in this article were: https://www.ncbi.nlm.nih.gov/pubmed and https://sph.uth.edu/retnet/. Keywords for searching (selection criteria): retinal degeneration, photoreceptors, rods, neuroprotection, gene therapy, cell replacement, optogenetics, retinal prosthesis, calcium, calpains,PEDF. We set dates of searching: 2000-2019.
Inherited Retinal Degeneration
IRD is a group of diseases that can lead to vision loss and eventually to blindness due, primarily, to photoreceptor cell death (Broadgate et al., 2017). The incidence of IRD is estimated 1:2000, thus being the most common cause for visual loss in the working population of the industrialized world (Cremers et al., 2018). The term IRD groups several diseases in which photoreceptors are affected and can be stationary, as for congenital stationary night blindness and achromatopsia, or progressive as in retinitis pigmentosa (RP),Leber’s congenital amaurosis (LCA) and Stargardt disease(Verbakel et al., 2018). IRD are genetically and clinically heterogeneous retinopathies. More than 100 different genes have been linked to the disease and each of them can bear different mutations (https://sph.uth.edu/retnet/). There is a great functional diversity in the types of genes that have been implicated in IRD and they can be eye specific (e.g., components of the visual transduction cascade or of the retinoid cycle, involved in outer segment renewal, photoreceptor specific structural proteins, transcription factors) or ubiquitously expressed (e.g., splicing factors, contributing to nucleotide metabolism) (Daiger et al., 2013). The genetic and functional multiplicity of the involved proteins might cause the activation of distinctive molecular mechanisms for the different forms of RP. However, the most recent findings suggest that some common mechanisms are associated to photoreceptor demise in the animal models for IRD analyzed so far (Marigo,2007).
While the mutations behind many of the disease types are known, only one treatment based on gene therapy for theRPE65gene is available for Leber’s congenital amaurosis,and some other gene therapy treatments are developing for mutations in specific genes (Trapani and Auricchio, 2019).Nevertheless, development of gene therapy strategies for each mutated gene or, even, for specific mutations in one gene is not feasible and requires such highly personalized therapy approaches, that only few patients may benefit from every single new treatment that will be generated. Otherwise, recent studies characterized cell death mechanisms in several models of IRD, either caused by dominant or recessive mutations, and found some events that play key roles in all the analysed retinas, such as increases of cyclic guanosine monophosphate (cGMP) and high levels of intracellular calcium ions (Power et al., 2019). Based on this evidence,development of new treatments targeting the characterized common molecular mechanisms leading to photoreceptor cell death may benefit a larger cohort of patients (Marigo,2007).
In IRD, the causative mutations frequently affect rods but degeneration of diseased rods leads to a secondary loss of cones, even if cones are genetically unaffected (Campochiaro and Mir, 2018). There are several evidences that preservation of rods, although not functional, can save sight, because vision in humans is mainly mediated by cones (Sahel and Léveillard, 2018; Vighi et al., 2018). The purpose of neuroprotection is, indeed, based on preservation of rod photoreceptor cells and consequently cones to save vision.
Therapeutic Prospects for Retinal Degeneration
The slow progression of the disease allows a wide time window for treatments but different stages of the disease may be more appropriate to be targeted by different therapeutic approaches (Figure 1). At early stages of the disease, when the retinal structure and histology are still not fully degenerated and photoreceptor cells are present, gene therapy and neuroprotection are the most appropriate approaches(Pardue and Allen, 2018). In fact, a successful gene therapy based on AAV2 delivery was recently approved for patients bearing mutations in theRPE65gene and was applied to patients that, based on optical coherent tomography analysis,showed a preserved photoreceptor cell layer (Trapani and Auricchio, 2019). When most of photoreceptors are lost, cell replacement is an option. Transplantation of photoreceptors in patients is not in clinical trials yet, but several studies evaluated photoreceptor transplantation in wild type or IRD mutant mice (Jayakody et al., 2015). Seminal studies showed that post-mitotic photoreceptor precursor cells or mature photoreceptors can integrate in the degenerating retina of murine models of IRD, express photoreceptor markers, are light sensitive and improve function (MacLaren et al., 2006;Lakowski et al., 2010; Gust and Reh, 2011). The challenges of these studies are to obtain long-term survival of transplanted cells and sufficient integrated cells for improved functionality. Endogenous sources of photoreceptors are the ciliary epithelium and Müller glia cells (Tropepe et al., 2000;Giannelli et al., 2011), and recent studies provided evidences that the regenerative ability of Müller glia cell may represent a new therapeutic approach for retinal degeneration (Langhe and Pearson, 2019). While several protocols have been developed to differentiate rod-like cells from embryonic stem cells (Osakada et al., 2008; Lamba et al., 2009), induced pluripotent stem cells (Osakada et al., 2009; Lamba et al., 2010;Tucker et al., 2014) and adult retinal stem cells (Coles et al.,2004; Giordano et al., 2007; Demontis et al., 2012), none of these differentiation protocols can, at the moment, provide cells in number and integration capacity appropriate for an efficient transplantation of photoreceptors (Marigo and Casarosa, 2014; Gasparini et al., 2019). Differently, transplantation ofin vitrodifferentiated retinal pigment epithelium is at a much more advanced stage and in clinical trials,as differentiated human embryonic stem cells-derived retinal pigment epithelium cells have been transplanted in patients with age-related macular degeneration and Stargardt disease(Bertolotti et al., 2014; Schwartz et al., 2015). An autologous transplant of retinal pigment epithelium derived from induced pluripotent stem cells was performed in a patient with age-related macular degeneration (Mandai et al., 2017). One year after surgery, the transplant demonstrated to be safe but with no improved visual acuity. Perception of light can also be restored by optogenetic approaches in advanced stages of degeneration (Fortuny and Flannery, 2018). Optogenetics is a biotechnological approach to allow light perception by a light-sensitive protein ectopically expressed in retinal cells that are not photoreceptors. The idea behind optogenetics is that, provided the complete loss of the light-sensitive photoreceptors in IRD, new light-sensitive cells can be generated by misexpression of proteins, that can be membrane integral ion channels, i.e., channelrhodopsin and halorhodopsin,or retinal G-protein coupled receptor, like opsins, that can change membrane potential upon light stimuli (Ostrovsky and Kirpichnikov, 2019). The low light sensitivity of channelrhodopsin and halorhodopsin was recently overcome by the finding that cone opsin can activate a G-protein-coupled inward-rectifier potassium channel and transduce the signal(Berry et al., 2019). The delivery of the genes encoding for optogenetic tools was based on viral delivery, like in gene therapy, in animal models of IRD. The targets of the optogenetic gene therapy are second-order neurons, such as bipolar cells, or retinal ganglion cells, third-order neurons, because IRD leads to loss of photoreceptors but the rest of the retina can be preserved for long time (Stefanov et al., 2019).
In case degeneration reaches a terminal stage with complete photoreceptor loss, implant of a retinal prosthesis needs to be evaluated (Bloch et al., 2019). Advances in retinal prostheses increased in the last decades thanks to improved microelectronics, biomaterials and retinal surgery methodologies. Retinal prostheses can be recorded in two major groups: epiretinal prostheses and subretinal prostheses. Epiretinal prostheses are implanted on the vitreal side of the retina to stimulate retinal ganglion cells, the neurons that form the optic nerve and connect the eye to the brain.Clinical trials with hundreds of patients enrolled for the Argus II Retinal Prosthesis System (Second Sight Medical Products Inc., Sylmar, CA, USA), approved by the Food and Drug Administration in 2013, demonstrated statistically improved quality of life and functional vision tasks (Dagnelie et al., 2017; Duncan et al., 2017). Subretinal prostheses are implanted on the side of photoreceptor cells with the aim of stimulating the retinal interneurons and possibly benefit from retinal signal amplification. Clinical trials with the Alpha IMS by Retinal Implant AG (Reutlingen, Germany) reported safety and improvements in quality of life and object recognition (Kitiratschky et al., 2015).
These new biotechnological approaches are attracting a lot of attention for patients with no residual photoreceptors leftand thus at a stage of complete blindness.
Patients at early stages of the disease and still presenting photoreceptor cells can aspire to a treatment to delay degeneration. Pharmacological approaches are mostly based on neuroprotection aimed at slowing the progression of the disease by interfering with inflammation or oxidative stress or apoptosis (Dias et al., 2018). The purpose of neuroprotection is the survival and maintenance of neurons and, in the case of IRD, of photoreceptors. The neuroprotective treatment is suitable for the slow degenerative progress characterizing IRD, however, at the moment, no pharmacological therapy demonstrated enough efficacy to restore vision. Some neuroprotective approaches have been attempted by injection of stem cells. Exogenous sources of stem cells are non-retinal stem cells such as mesenchymal stem cells, derived from adipose tissue, bone marrow or dental pulp. Recent studies showed that injections of these types of cells have neuroprotective effects without any replacement of photoreceptors in the murine retina (Mead et al., 2015). Genetically modified bone marrow mesenchymal stromal cells overexpressing brain derived neurotrophic factor, injected in the rd6 IRD mouse model, could effectively rescue the damaged retina by neuroprotective means (Lejkowska et al., 2019). Some clinical trials are now undergoing based on injections of autologous mesenchymal stem cells in IRD patients (Labrador-Velandia et al., 2016). We should keep in mind that the therapeutic possibilities of mesenchymal stem cells can be unpredictable because these cells are often derived from patients for autologous transplants and their ability to secrete neuroprotective molecules will vary from one individual to the other.
Neuroprotection is, otherwise, often achieved by the delivery of small molecules at specific concentrations either locally in the eye or systemically (Sieving et al., 2006; Perusek and Maeda, 2013; Scholl et al., 2015; Vighi et al., 2018).This requires prolonged administration of the drug and one treatment is usually not definitive. Therefore, appropriate delivery systems, necessary to allow the drug to reach the neural retina, need to be developed based on the chemical characteristics of the different neuroprotective molecules(Himawan et al., 2019). The promising aspects of neuroprotective approaches are based on the fact that neuroprotection is not driven by a specific mutation in one gene but aims at targeting common cell stress pathways for the treatment of a broad spectrum of patients in a mutation-independent modality. This therapeutic approach allows also combined therapies and is less dependent on the stage of the disease because it will target cells that, at the specific moment of the treatments, are facing molecular and metabolic changes associated to cell death. Production of promising neuroprotective drugs requires a deep knowledge of the physiological and metabolic changes as well as molecular pathways activated in photoreceptor cells during the degenerative process.
Cell Death Mechanisms in Rod Photoreceptor Cells
The definition of whether different genetic lesions trigger similar cell death mechanisms and the identification of the crucial players during the degenerative process are strategic matters to be addressed for the development of new treatments for this genetically heterogeneous but phenotypically similar group of diseases.
The role of apoptotic pathways engaging executioner caspases during photoreceptor degeneration has been quite controversial. Caspase 3 and caspase 7, both executioner of apoptosis, were found activated in transgenic rats and mice with a mutation in the Rhodopsin (Rho) gene (Liu et al.,1999; Gorbatyuk et al., 2010; Comitato et al., 2019b). Several data, otherwise, on different models of the disease indicated that a caspase-independent mechanism is triggered during retinal degeneration (Donovan and Cotter, 2002; Doonan et al., 2003; Comitato et al., 2019b). The limited impact of caspase 3 in IRD was confirmed by taking advantage of caspase 3-deficient mice, in which knock-out of caspase 3 provided only transient photoreceptor protection (Zeiss et al., 2004). Supporting this hypothesis werein vivotreatments with a pan-caspase inhibitor, such as Z-VAD-FMK, that offered very limited neuroprotection in murine models of IRD (Sanges et al., 2006; Comitato et al., 2019b). The focus on caspases was based on the fact that BCL2-associated X protein (BAX) had been found activated in the degenerating retinas of animal models of IRD. Our studies extensively evaluated BAX activation in at least three models of RP, therd1mouse bearing a recessive mutation in thePde6bgene,theRhoknock-out mouse and a transgenic mouse expressing the P23H mutation in RHO, and demonstrated that its function is mainly related to the efflux of the apoptosis inducing factor (AIF) from mitochondria and not to caspase activation (Comitato et al., 2014). These and other studies suggested that executioner caspases may be activated but they are not critical in mediating retinal degenerationin vivo. Based on these evidences the use of the term “apoptosis”for photoreceptor cell death in IRD is, thus, considered not appropriate and scientists in the field prefer to refer to photoreceptor cell death or photoreceptor degeneration for these events (Power et al., 2019).
Accumulating evidences from our and other laboratories implied that mitochondria and the endoplasmic reticulum(ER) are major points of integration of cell death signals.These two organelles contribute to tides and ebbs in calcium ions leading to unbalance of Ca2+fluxes triggering cell demise. Intracellular Ca2+levels are strictly regulated because they can affect neuronal survival (Yamashima and Oikawa,2009). Several studies on models for photoreceptor cells death reported that the molecular pathways following calcium overload differ from classical caspase mediated apoptosis and engage calpains (Paquet-Durand et al., 2006, 2019;Sanges et al., 2006; Comitato et al., 2019b; Figure 2).
Calpains are cysteine proteases sensitive to intracellular calcium and are activated by increases in intracellular [Ca2+].Inactive calpains are heterodimers, composed of an 80 kDa proteolytic subunit and a 28 kDa regulatory subunit (Ravulapalli et al., 2009). In the ER the heterodimer is associated with an endogenous calpain inhibitor called calpastatin.Calpastatin release and Ca2+stimulated dissociation of the regulatory subunit lead to the activation of the calpain enzymes (Hood et al., 2004). Activation of calpains has been associated to cell death in IRD (Marigo, 2007; Paquet-Durand et al., 2019). Calpains do not directly cause chromatin condensation but they are proteases with a broad spectrum of substrates such as cytoskeleton components, AIF and BAX (Goll et al., 2003; Comitato et al., 2014) (Figure 2). AIF is a flavoprotein localized in the mitochondrial intermembrane space. Upon proper cell death stimuli, AIF exits the mitochondrion through BAX-formed pores and translocates to the nucleus where induces chromatin fragmentation (Arnoult et al., 2003; Comitato et al., 2014). Cleavage and release of AIF from mitochondria are regulated by calpain 1 and can occur in the absence of cytochrome c release, an event that otherwise induces apoptosis (Polster et al., 2005; Ozaki et al.,2009). In several neuronal degeneration models, including retinal degeneration, activation of AIF and its translocation to the nucleus had been observed (Cande et al., 2002;Sanges et al., 2006; Cao et al., 2007; Mizukoshi et al., 2010;Rosenbaum et al., 2010; Comitato et al., 2016, 2019b). The activated form of AIF recruits Cyclophilin A for chromatin fragmentation that culminates in cell death (Arnoult et al.,2003; Cande et al., 2004).
Dysregulation of different photoreceptor factors may cause calcium overloads leading to calpain activation. Recessive mutations in thePde6bgene in therd1mouse model cause lack of PDE6 enzyme activity. PDE6 is a key enzyme in the phototransduction cascade. PDE6 hydrolyses cGMP in response to light and rhodopsin (RHO) activation. Impaired PDE6 activity causes elevated levels of cGMP (Farber and Lolley, 1974; Vighi et al., 2018). The correlation of elevated intracellular cGMP and photoreceptor cell death is quite well documented and appears to underlie photoreceptor cell demise caused by mutations in several genes linked to IRD(Power et al., 2019). In healthy photoreceptors, cGMP binds and keep open the cGMP-gated channels, channels regulating entrance of cations and, among them, Ca2+. Excessive cGMP, thus, results in elevated intracellular calcium (Sanges et al., 2006). Increased cGMP, on the other hand, can also activate cGMP-dependent protein kinase enzymes that trigger cell death mechanisms (Paquet-Durand et al., 2009; Vighi et al., 2018; Figure 2).
Mutations that cause misfolding of the RHO protein have been also associated with increased intracellular Ca2+in rod photoreceptors (Shinde et al., 2016; Comitato et al., 2019b).Dominant mutations in RHO account for 20-25% of the dominant forms of RP and most of these mutations lead to misfolding of the protein and retention in the ER (Behnen et al., 2018). Dominant mutations in RHO have been studied for several years and numerous murine models are available as transgenic or knock-in mice. Activation of ER resident sensors, such as IRE (inositol-requiring enzyme 1),ATF6 (activating transcription factor-6) and PERK (protein kinase R-like ER protein kinase) have been reported but the functions of these sensors in the unfolded protein response to activate protective mechanisms or in ER-stress leading to cell death are still not completely defined in degenerating photoreceptors (Lin et al., 2007; Kunte et al., 2012; Chiang et al., 2015; Athanasiou et al., 2017; Comitato et al., 2018).In transgenic mice, in which expression of mutant RHO is combined with RHO protein overexpression, ER-stress sensors linked to apoptosis are activated (Gorbatyuk et al.,2010; Kunte et al., 2012; Comitato et al., 2016). Differently,in RHO recessive mutations, as in the knock-out mouse of theRhogene, no ER-stress could be revealed but high [Ca2+]was reported (Comitato et al., 2016). Interestingly, in murine models of IRD with an equal gene dosage of wild type and mutant proline 23 to histidine (P23H)Rho, such as in the P23H knock-in mouse (RhoP23H/+), activation of the ER resident sensors, i.e. phosphorylated IRE1 and PERK, could be detected but this activation appeared to be related to ER-associated protein degradation and unfolded protein response and not to cell death (Chiang et al., 2015; Comitato et al.,2019b). Specifically, we defined that activation of PERK leads to phosphorylation of the nuclear factor erythroid 2-related factor 2 transcription factor, which is a mediator of the antioxidant response and possibly a protective mechanism during photoreceptor degeneration (Comitato et al., 2019b).On this line of evidences, inhibition of the PERK pathway revealed to be detrimental, suggesting that PERK sustains unfolded protein response and is a compensatory response in the degenerating retina (Athanasiou et al., 2017; Comitato et al., 2019b). These data are relevant for the studies on IRD because theRhoP23H/+knock-in mouse models the degenerative progression of photoreceptors similarly to what found in RP patients bearing the P23H mutation in RHO, i.e., with a slow degeneration starting from the ventral side of the retina(Sakami et al., 2011).
Altogether the studies suggest common mechanisms of cell demise in dominant and recessive forms of RP caused by mutations in thePDE6BandRHOgenes. In murine models of these types of RP intracellular increase of calcium ions and activation of calpains have been pinpointed as key players triggering photoreceptor degeneration.
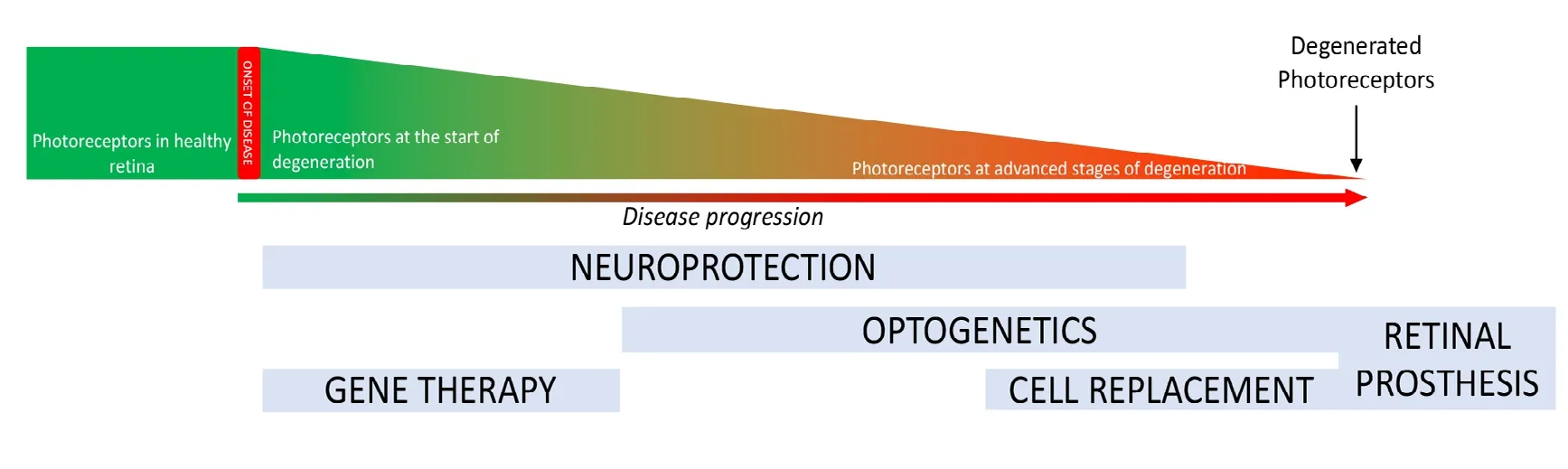
Figure 1 Stages of photoreceptor degeneration and applicable therapies.Degeneration is represented in a graph showing the reduction in photoreceptors cells during degeneration. Below we report the time windows of different therapeutic options. Gene therapy is appropriate for early stages of photoreceptor degeneration and neuroprotective strategies can treat ongoing photoreceptor cell degeneration. Both these treatments act on endogenous photoreceptors. Cell replacement, optogenetics and retinal prosthesis are strategies to treat patients at advanced/late stages of degeneration.
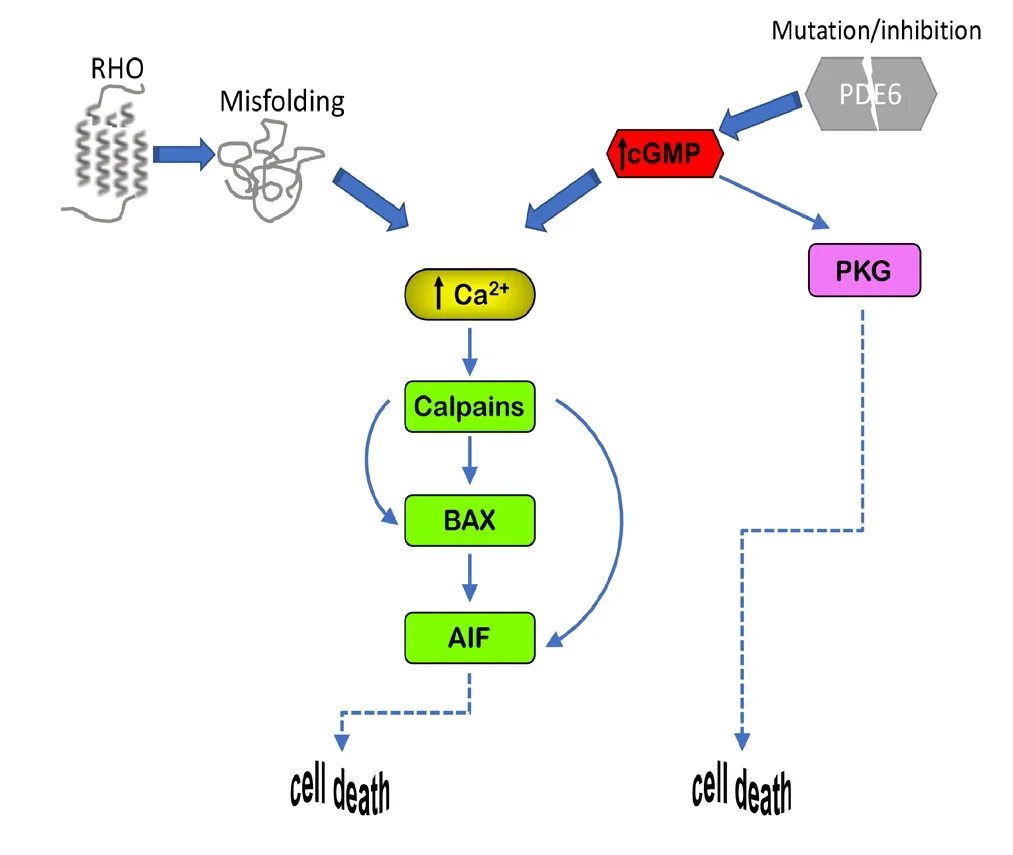
Figure 2 Cell death mechanisms.
Targeting Cell Death Mechanisms for Neuroprotection of Degenerating Photoreceptors
Several studies demonstrated that targeting calpains can be a promising therapeutic neuroprotective option for the degenerating retina. We showed that, in therd1mouse model with a recessive mutation in thePde6bgene, calpain 1 appears to play a major role in the activation of the cell death pathway leading to AIF nuclear translocation (Comitato et al., 2014). Several calpain inhibitors have been tested in this mouse model of IRD and many of them showed neuroprotective effect in short-term delivery (Paquet-Durand et al., 2006, 2010; Sanges et al., 2006). However, some calpain inhibitors, such as CX295 and SJA6017, demonstrated to be toxic when the retina was exposed for a prolong time period to the inhibiting compounds (Paquet-Durand et al., 2010).In healthy tissue, calpain 1 and calpain 2 are maintained in an inactive state by binding to calpastatin, a highly specific endogenous inhibitor (Hood et al., 2004). A peptide derived from the natural inhibitor calpastatin was tested in the degenerating eyes and provided neuroprotection in recessive and dominant models of IRD after short and prolonged exposure timesin vitro, on retinal explants, andin vivoafter intravitreal injection (Paquet-Durand et al., 2010; Comitato et al., 2014, 2016). Neuroprotection byin vivoinjection in the eye of the calpastatin peptide gave variable results in different models of IRD, with effects ranging from 30% to 80% reduction of dying cells (Paquet-Durand et al., 2010;Comitato et al., 2014, 2019a). A possible explanation is the high specificity of calpastatin for two types of calpains, i.e.,calpain 1 and calpain 2. In case other calpains are activated,calpastatin cannot block them. In fact, while in the knock-in mouseRhoP23H/+we found 80% correlation of calpain activation with the cell death marker terminal deoxynucleotidyl transferase dUTP nick end labeling at the peak of degeneration, calpastatin peptide could reduce cell death only by 30%(Comitato et al., 2019a). We reasoned that other calpains,aside calpain 1 and calpain 2, might be activated during retinal degeneration caused by the P23H mutation in RHO and found that a different calpain inhibitor (PD150606), which can target the majority of calpain types, could protect the retina from cell death by 65%. The strong neuroprotective activity of PD150606 suggests that different calpains are activated in retinas bearing different mutations leading to IRD.Nevertheless, the common mechanism activated by changes in [Ca2+] appears to be shared by several models of the disease and, thus, lowering calcium ions should also be evaluated as new therapeutic avenue (Comitato et al., 2019b).
In a recent study we confirmed the hypothesis that decreasing intracellular calcium can be neuroprotective in models of IRD. We and others showed that the pigment epithelium derived factor (PEDF) can preserve the degenerating retina of recessive and dominant models of IRD(Holekamp et al., 2002; Wang et al., 2013; Kenealey et al.,2015; Polato and Becerra, 2016; Comitato et al., 2018).Short-term treatments by intravitreal injection of human recombinant PEDF restrained cell death in the rd1 mutant retina by binding the PEDF receptor encoded by thePNPLA2gene (Kenealey et al., 2015) and a small peptide of 17 amino acids (17mer) was identified as the neurotrophic domain of the protein. PEDF or the 17mer were demonstrated to act by targeting the PMCA pumps at the plasma membrane of photoreceptors and, thus, by favoring calcium efflux with a consequent reduction of intracellular [Ca2+] below toxic levels (Comitato et al., 2018). Interestingly, the PEDF receptor is an integral membrane protein with a phospholipase A2 activity stimulating the release of the omega-3 fatty acid docosahexaenoic acid from phospholipids (Subramanian et al.,2013; Pham et al., 2017). Docosahexaenoic acid was proven in myocytes and cardiomyocytes to support PMCA pumps and to interfere L-type Ca2+channels counteracting calcium overload (Pepe et al., 1994; Mączewski et al., 2016). We, thus,propose that PEDF neuroprotective activity for degenerating photoreceptors acts by releasing intracellular docosahexaenoic acid, which increases PMCA pump activity to extrude calcium ions. The decrease of intracellular [Ca2+] induced by PEDF attenuate the cell death mechanism with lowered calpain activation and reduced mitochondrial BAX and nuclear translocation of AIF (Comitato et al., 2018). Altogether, the central cell death mechanism triggered by high intracellular[Ca2+] is diminished by PEDF. The open question that needs to be addressed is whether long-term exposure to PEDF can support photoreceptor survival or may have undesired side effects which will preclude the use of PEDF in therapy.
Perspectives and Conclusions
A limiting aspect in designing a cure for IRD is the high genetic heterogeneity found by molecular diagnosis in patients and the high percentage of isolated instances. General and common factors activated by mutations in different genes can be keystones for translational research. We identified activation of calpains, engaged by high intracellular Ca2+, as features shared by several murine models of IRD. In order to plan effective treatments to stop cell death during retinal degeneration we need specific studies aimed at defining whether high Ca2+and calpains activate all the downstream catastrophic events leading to cell death or whether they cooperate with other proteases. The identification and characterization of molecules acting on these events needs also to be complemented by the development of appropriate delivery systems for the retina (Himawan et al., 2019). In fact, the different chemico-physical properties of neuroprotective agents tested in mice by short-term delivery will require specific and differentiated delivery systems. A second challenge will be a specific delivery either to rod or to cone photoreceptors to avoid side effects, such as bioconjugated compounds, in case of synthetic molecules (Wadhawan et al., 2019) or viral pseudotypes and rod-specific promoters in case of gene therapy approaches (Auricchio et al., 2001; Mussolino et al.,2011). Treatments with neuroprotectants targeting cell death mechanisms can delay photoreceptor degeneration but may also be of interest for combined treatments. In fact, gene therapy for recessive forms of IRD is in the clinic but appears to be more effective in young individuals and thus on cells at an early stage of degeneration (Trapani and Auricchio, 2019).A healthier photoreceptor appears to be a better target for gene therapy. Neuroprotection could, thus, be envisaged as a treatment to prolong sight but also for combined therapies to enhance the effectiveness of gene therapy approaches. Similarly, we may expect that also cell transplantation may have more chance of integration in a retinal tissue with a limited stressed status and low inflammation.
Author contributions:MK, LH, VM wrote the manuscript and approved the final manuscript and submission.
Conflicts of interest:The authors declare no conflicts of interest.
Financial support:This work was supported by grants from the Telethon Foundation (GGP14180, GGP19113) and the European Union (LSHGCT-2005-512036 and transMed, MSCA-ITN-2017-765441) (all to VM).
Copyright license agreement:The Copyright License Agreement has been signed by all authors before publication.
Plagiarism check:Checked twice by iThenticate.
Peer review:Externally peer reviewed.
Open access statement:This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-Non-Commercial-ShareAlike 4.0 License, which allows others to remix, tweak,and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.

- 中国神经再生研究(英文版)的其它文章
- Transcriptional regulation of adult neural stem/progenitor cells: tales from the subventricular zone
- Green tea catechins inhibit microglial activation which prevents the development of neurological disorders
- Reversibility of visual field defects through induction of brain plasticity: vision restoration, recovery and rehabilitation using alternating current stimulation
- Role of activin receptor-like kinase 1 in vascular development and cerebrovascular diseases
- Effects of durotomy versus myelotomy in the repair of spinal cord injury
- Spinal genesis of Mayer waves