
The Temporal Relation between Cardiomyopathy and LBBB and Response to Cardiac Resynchronization Therapy:Case Series and Literature Review
2020-03-25 11:02SanshuaiChangMDYiHePhDHuiWangMSFeiGuoMDQiangLvMDJunpingKangMDRongBaiMDXiaohuiLiuMDXinDuMDChangshengMaMDandProfJianzengDongMD
Sanshuai Chang,MD ,Yi He,PhD ,Hui Wang,MS ,Fei Guo,MD ,Qiang Lv,MD ,Junping Kang,MD ,Rong Bai,MD ,Xiaohui Liu,MD ,Xin Du,MD ,Changsheng Ma,MD andProf.Jianzeng Dong,MD
1 Department of Cardiology,Beijing AnZhen Hospital,Capital Medical University,National Clinical Research Centre for Cardiovascular Diseases,Beijing,China
2 Department of Radiology,Beijing AnZhen Hospital,Capital Medical University,National Clinical Research Centre for Cardiovascular Diseases,Beijing,China
Abstract
Keywords:left bundle branch block;cardiomyopathy;heart failure;cardiovascular magnetic resonance;cardiac resynchronization therapy
lntroduction
Cardiac resynchronization therapy (CR T) has been shown to improve left ventricular (L V) function,reduce heart failure hospitalizations,
REVlEW
and reduce mortality in selected heart failure (HF) patients with nonischemic cardiomyopathy (NICM) with left bundle branch block (LBBB) [1- 4].However,a major issue with CR T is that when patients are selected according to current guidelines,about 20-40% still do not benef t [5,6].Traditional predictors of CRT response,including echocardiographic assessment of dyssynchrony,have proved disappointing in multicenter studies [7].
Insights are needed into the pathogenesis of HF to accurately select CRT candidates [8].Previous studies suggested that LBBB is a reversible cause of NICM with HF.In a prospective study involving 29 patients with dilated cardiomyopathy and LBBB [9],LV dysfunction was completely reversed after CR T in a small but impor -tant subset (17%) of the patients,f rst giving rise to the new concept of LBBB-induced cardiomyopathy.Vaillant et al.[10] reported that HF may develop over a mean of 11.6 years of LBBB,and LBBB-induced cardiomyopathy was identif ed in 1.6% of 375 patients who received CR T.The results showed that improvement of L V structure and function can be achieved by CR T in those patients.
Although the concept of LBBB-induced cardiomyopathy was proposed,it is diff cult or impossible to determine definitively the causal relation between cardiomyopathy and LBBB only by clinical records.Consecutive clinical documents in many years are needed,especially in the asymptomatic period,which cannot be saved well by most HF patients.The association between HF pathogenesis and CR T response should be explained integrally,and practical criteria for selecting CR T candidates are needed.
Here our proposal is that the temporal relation between cardiomyopathy and LBBB could be a key factor for CRT response,and the chronological order can be identif ed by different contraction patterns in cardiovascular magnetic resonance (CMR),which could be a principal consideration for selecting candidates for CRT.We present two patients as evidence:one had LBBB-induced cardiomyopathy with specif c features in CMR and had good response to CR T;the other had cardiomyopathy-induced LBBB with dif ferent CMR characteristics and poor response to CRT.
Methods
All patients in Beijing Anzhen Hospital with HF and for whom CMR images were available were reviewed.Cardiomyopathy and LBBB were diagnosed in 1 17 patients,24 of whom received CR T.There were two patients who had a clear temporal relation between cardiomyopathy and LBBB.Ethics approval was obtained from the Human Research Ethics Committees of Beijing Anzhen Hospital,and informed consent was sought from individual patients for their agreement to participate in longterm follow-up.
lnclusion Criteria and Data Acquisition
LBBB was defined as follows:QRS duration 120 ms or greater,QS or rS in lead V1,broad (frequently notched or slurred) R waves in leads V5 and V6,absent Q waves in leads V5 and V6 [11].
NICM with HF was diagnosed by echocardiography according to the following criteria:LV ejection fraction (LVEF) of 40% or less,L V end-diastolic diameter (LVEDD) of 55 mm or greater,New York Heart Association (NYHA) functional class III or IV,no evidence of features or history suggesting coronary artery disease or a potential reversible cause of NICM,including alcoholic cardiomyopathy,thyrocardiomyopathy,myocarditis and tachycardiomyopathy were excluded.
The patients ’ baseline characteristics,including age,sex,and history of coronary artery disease,hypertension,and diabetes,were collected.The onsets of LBBB,cardiomyopathy,and HF were retrospectively ascertained by review of medical records including ECG and echocardiography recordings.
CMR Analysis
All CMR scans were performed before CRT at admission.The patients were scanned with a 3.0-T magnetic resonance scanner (Verio,Siemens Healthcare,Germany).All analyses were performed with CVI42 (version 5.3,Circle Cardiovascular Imaging).A customized software program was used for semiautomated analysis of LV strain.LV endocardial and epicardial borders were manually traced in end- diastolic short-axis cine views and contractile strain plots for each LV segment were automatically generated.
For CMR modalities,the left ventricle was divided into 17 segments according to the American Heart Association LV segmentation model.LV wall thickness at the end of systole and the end of diastole,LV septal-to-lateral thickness ratio,and LV wall thickening were obtained at the midventricular level.The presence of abnormal late gadolinium enhancement in the LV myocardium was visually detected and was also quantitated by CVI42.In addition,the circumferential strain,representing myocar -dial shortening/stretching in the short-axis plane,was assessed.Regional stretching is expressed as a positive value and shortening is expressed as a negative value.From these data,peak strain,time to peak strain,strain rate,and peak shortening delay (the delay of the f rst peak circumferential strain between the septal wall segment and the lateral wall segment) were calculated [12].
ln-Hospital Management
The patients continued to have NYHA functional class III or IV HF with LVEF less than 40% despite optimal medical treatment,so CR T was recommended for these symptomatic HF patients in sinus rhythm with a QRS duration of 150 ms or greater and LBBB (class I,level A) [6].After consent had been obtained,CRT devices were implanted transvenously.The LV lead was implanted in the lateral or the posterolateral region of the left ventricle,ideally in the midventricular region rather than the basal or apical region.The implantation of a bipolar L V lead was recommended to enable all four LV pacing conf gurations so as to avoid phrenic nerve stimulation and/or to maximize the LV pacing threshold in the final lead position.Systematic efforts were made to obtain the narrowest biventricular paced QRS complex during the implantation procedure and initial programming.
Follow-up and Outcome Assessment
All patients received optimal medical treatment after CRT and were followed up by face-to-face inter -views in outpatient clinics.At each follow-up visit,echocardiography was used to examine the changes in LVEDD and LVEF.The patients ’ symptoms were also evaluated and were graded according to NYHA functional class.CRT response criteria were defined as at least a 15% reduction in LVEDD,a 5% absolute increase in L VEF,and change to at least one NYHA class lower on the basis of prior studies that assessed response to CRT [13,14].
在现代社会中,大多数城市居民已经远离自然环境。所以,在进行工程设计时,应该让人们充分参与到实际的设计过程中,通过树叶摆动、花开花落等四季的变化让人们能够更加关怀环境,并积极参与到生态公园的设计工作中。
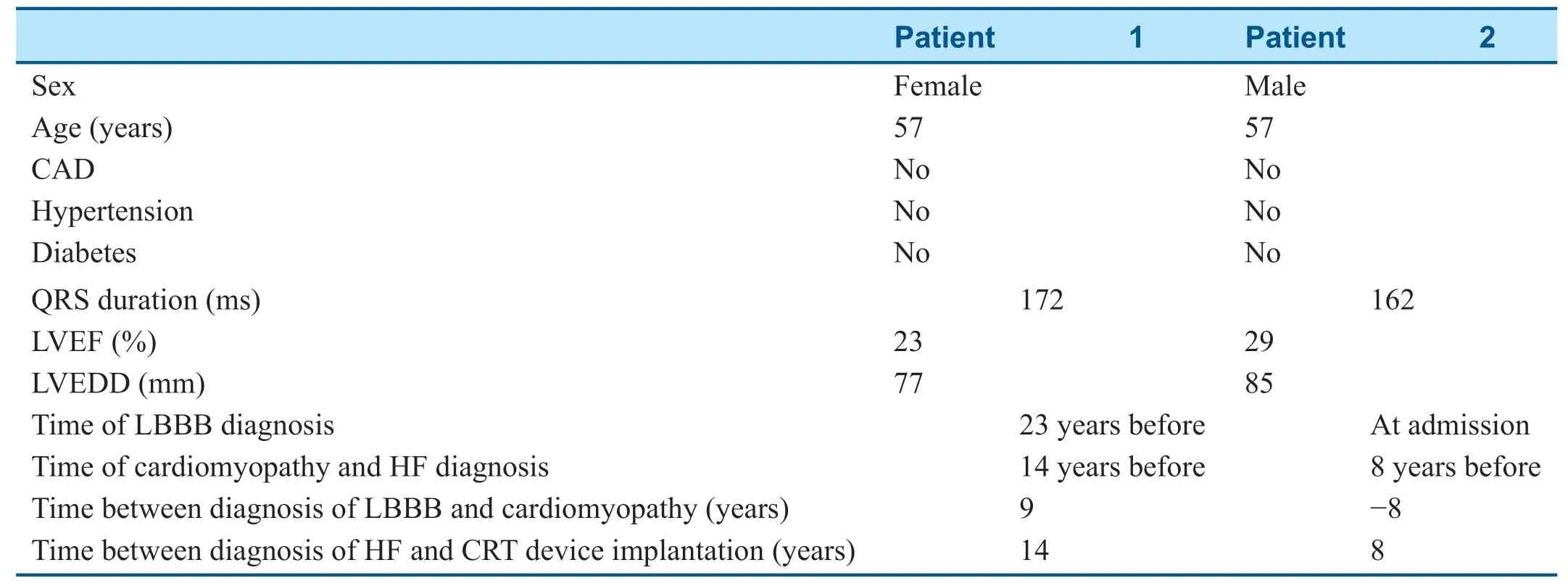
Table1 Main Clinical and Echocardiographic Characteristics of Individual Patients at the Baseline.
Results
Baseline Characteristics
The baseline characteristics of the patients are detailed in Table1.In patient 1,LBBB had been diagnosed 23 years before,at which time echocar -diography showed her LVEDD was 49 mm and her LVEF was 61%;cardiomyopathy with HF appeared 9 years later (seemingly induced by LBBB).In patient 2,cardiomyopathy and HF had been diagnosed 8 years before.His L VEF was 40% and his LVEDD was 70 mm.The ECG then showed a normal QRS duration of 100 ms,and LBBB was present at the latest admission.ECGs at different stages are shown in Figure1.
CMR Measurements
CMR measurements of the two patients before CRT device implantation are shown in Table2 and Figure2.The LV wall thickness at the end of systole and the wall thickening rate were higher in patient 1,and the ratio of septal-to-lateral thickness was much lower.In addition,the peak circumferential strain for patient 1 was comparatively higher in the lateral and septal walls,and the peak circumferential straindelay between the lateral wall and the septal wall was longer for patient 1.Distinctively dif ferent LV deformation patterns in the two patients were seen from CMR tissue tracking (Figure3).
Outcomes
During follow-up,the echocardiographic and NYHA classes of the two patients were assessed.Patient 1 demonstrated a good response to CR T;in contrast,patient 2 had no response to CRT (Table3).
Discussion
The cases we report here support the concept that patients with LBBB-induced cardiomyopathy will have a positive response to CRT,while patients with cardiomyopathy-induced LBBB will have a poorer response to CRT.Moreover,distinctively dif ferent cardiac contractility and L V deformation patterns can be recognized by CMR tissue tracking in those two patients.CMR findings are helpful to elucidate the underlying temporal relation between LBBB and cardiomyopathy,to select candidates for CR T,and to predict the prognosis.
It has been suggested that LBBB induces myocardial remodeling that includes asymmetric hypertrophy,f ber disarray,increased myocardial catecholamine concentrations,and altered perfusion distribution,thus contributing to L V dilatation and dysfunction [15].Meanwhile,increased wall stress,a longer conduction pathway,molecular/cellular changes,and flbrosis in HF patients may impair the conductive tissue,which conversely aggravate asynchronous electrical activation [16].As a result,the conduction disturbance and the cardiac remodeling seen in HF patients with NICM and LBBB interact to produce a vicious cycle [17].
Mechanisms of LBBB-lnduced Cardiomyopathy
With LBBB,the LV motion shows signif cant delay and is uncoordinated,with paradoxical septal motion,LV remodeling,and hemodynamic deterioration [18].The anomalous contraction inducesredistribution of cardiac mass,the early-activated regions becoming signif cantly thinner because of the low wall stress than the late activated regions,which are contracting against a higher wall stress,which results in the disuse atrophy of the LV septum and relative hypertrophy of the lateral wall [19] and leads to chronic L V dilatation (Figure4).If the L V activation sequence is corrected by CRT,the mechanical dyssynchrony and cardiac remodeling can be reversed and patients will have a good or even “ super” response to CRT (Figure5).
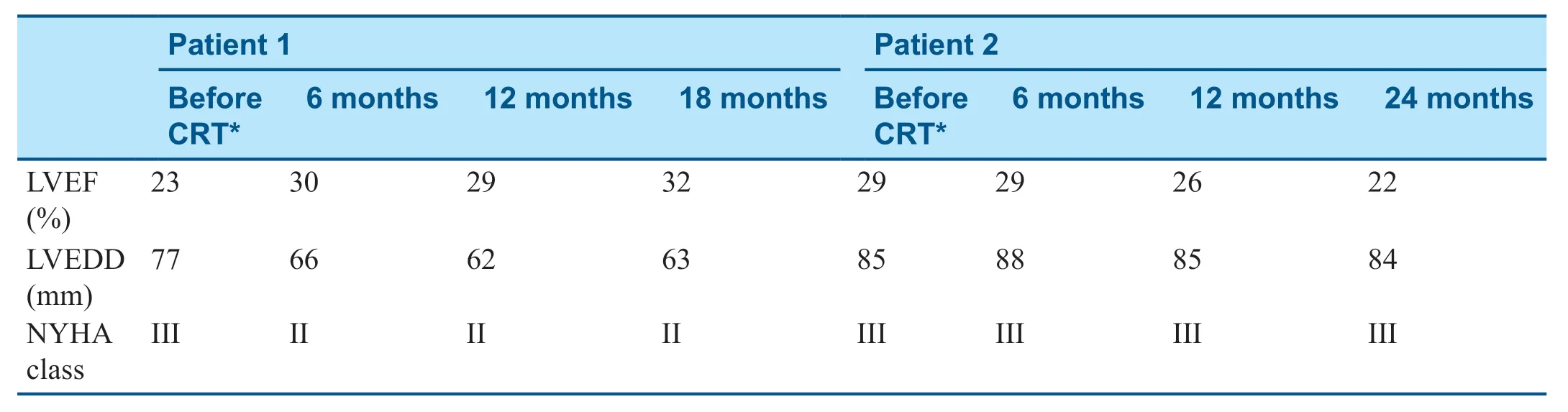
Table3 Echocardiographic and Clinical Parameters for Cardiac Resynchronization Therapy (CRT) Response for the Two Patients at each Follow-Up Visit.
Mechanisms of Dilated Cardiomyopathy- lnduced LBBB
However,in patients with preexisting cardiomyopathy,HF develops f rst and subsequently evolves with conduction disturbances.It is assumed that the underlying disease process,which induces not only LV dilation and LVEF reduction,may also be associated with myocardial flbrosis,and cellular uncoupling is likely to produce LBBB [17,20].In patients with cardiomyopathy-induced LBBB,the LV dysfunction is due to myocardial degeneration and flbrosis rather than asynchronous electrical activation (Figure4).Even though the activation sequence can be corrected by CR T,there is diffuse akinesia in the left ventricle,and the L V function cannot be restored;therefore,it is likely such patients will not respond to CRT.Besides,as all the cardiomyocytes,including the conduction system,are af fected by degeneration,the ECG in those patients may not have the typical LBBB morphology.
Assessment of the LV Contraction Patterns in HF Patients with LBBB
To clarify whether L V dysfunction is caused by myocardial akinesia (underlying cardiomyopathy) or is secondary to asynchronous electrical activation (LBBB),CMR circumferential strain was applied to assess the L V contraction pattern [21].Patient 1 exhibited an initial negative strain in the septal segment ref ecting presystolic contraction,followed by a positive strain ref ecting stretching and dyskinesis of the septum,while the compliant lateral wall was f rstly inappropriately stretched (positive strain) during septal contraction and the peak systolic circumferential strain (negative strain) occurred later (Figure2).The hemodynamic deterioration appears to be due to the paradoxical systolic septal motion and loss of the interventricular septal contribution to ejection fraction,indicative of a primary electrical abnor -mality.Therefore,the correction of the ventricular activation sequence by CRT improved both LV function and LV structure in this patient.However,patient 2 showed no dyskinesis but reduced amplitude of septal strain,with attenuated thickness of the myocardial wall and little wall thickening during systole.The results suggest that L V dysfunction was potentially related to electromechanical uncoupling from cardiomyopathy instead of specif c conduction system disease,and as expected the patient had no response to CRT.
It has been recognized that LBBB in HF can consist of several dif ferent activation patterns [22,23],which are not apparent on the surface ECG.Using noncontact mapping,Fung et al.[24] found some patients had preserved left bundle activation despite LBBB on ECG,whereas others had either a conduction block during LV activation or homogeneous depolarization propagation within the left ventricle.The latest segment of activation was located in either the lateral or the posterior region.These variables appear to be related to the outcome with CRT.
Several imaging modalities were also advocated to assess the dif ferent LV contraction patterns in LBBB patients [25-28].In a two-dimensional LV longitudinal strain study by echocardiography speckle tracking,a typical LBBB strain pattern showed early contraction in the septal wall and prestretching of the opposing wall,followed by late contraction,which is highly predictive of response to CRT [25].Likewise,a U-shaped L V contraction pattern in patients with LBBB was identif ed by CMR cine imaging,which might be explained by there being a relatively thin anterior part of the septum,due to dyssynchrony-induced asymmetric atrophy [19].The rates of CR T response in those with a U-shaped pattern were signif cantly greater at 6 months [26- 28].By comparison,the other pattern was characterized by a short transseptal delay and homogeneous slow L V activation toward the lateral wall,which is associated with a poorer response to CRT [26-28].Nevertheless,the relation between the CMR features and the chronological order of LBBB and cardiomyopathy was not noted.
Study Limitations
Firstly,this is a small series of patients to illustrate the temporal relation between LBBB and cardiomyopathy and response to CR T,which is clearly inadequate to draw a statistically powerful conclusion.Secondly,as an inherent def ciency of the retrospective study design,more detailed clinical documents cannot be provided to determine the causality relation of LBBB and cardiomyopathy.In addition,because CMR is not feasible after CR T device implantation,L V circumferential strain could not be assessed and compared with the preimplantation value.Despite these disadvantages,it can be seen from the literature review that the theory we propose is reasonable and has real impor -tance for selecting CR T candidates.Lar ge-sample prospective studies are needed to address further issues.
Conclusion
The temporal relation between cardiomyopathy and LBBB could be a determinant for CR T response.CMR tissue tracking,which can reveal the temporal relation,may be a useful tool for predicting CR T response.The concept provided a reasonable explanation for the CR T response and has real impor -tance for selecting CRT candidates.However,only two patients with a clear temporal relation between cardiomyopathy and LBBB were identif ed in this study.Comprehensive records of patients ’ medical history and HF progression could be helpful in future studies addressing this issue,Lar ger prospective clinical trials are needed to study the prevalence of,time course of,and risk factors for LBBB-induced cardiomyopathy.
Public source of funding
Funding was provided by the Ministry of Science and Technology of the People ’ s Republic of China (grants 2016YFC1301000 and 2016YFC0900900).
Confl ict ofilnterest
The authors report no relationships that could be construed as a conf ict of interest.
猜你喜欢
导航定位学报(2022年5期)2022-10-13
建材发展导向(2022年12期)2022-08-19
建材发展导向(2022年10期)2022-07-28
体育科技文献通报(2022年3期)2022-05-23
中国典型病例大全(2022年7期)2022-04-22
建材发展导向(2022年3期)2022-04-19
房地产导刊(2022年4期)2022-04-19
少先队活动(2021年5期)2021-07-22
老区建设(2016年7期)2016-12-06
吉林体育学院学报(2015年4期)2015-02-28
 Cardiovascular Innovations and Applications2020年1期
Cardiovascular Innovations and Applications2020年1期
- Cardiovascular Innovations and Applications的其它文章
- Frailty and Anticoagulant Therapy in Patients Aged 65 Years or Older with Atrial Fibrillation
- lmpact of Postdilation on lntervention Success and Long-Term Major Adverse Cardiovascular Events (MACE) among Patients with Acute Coronary Syndromes
- A Giant Right Atrial Myxoma with Blood Supply from the Left and Right Coronary Arteries:Once in a Blue Moon
- Does Coronary Microvascular Spasm Exist? Objective Evidence from lntracoronary Doppler Flow Measurements During Acetylcholine Testing