
Differences in brain-derived neurotrophic factor gene polymorphisms between acute ischemic stroke patients and healthy controls in the Han population of southwest China
2019-07-17 02:13JieZhouMengMengMaJingHuanFangLeiZhaoMuKeZhouJianGuoLiHe
中国神经再生研究(英文版) 2019年8期
Jie Zhou, Meng-Meng Ma, Jing-Huan Fang, Lei Zhao, Mu-Ke Zhou, Jian Guo, Li He
Department of Neurology, West China Hospital, Sichuan University, Chengdu, Sichuan Province, China
Abstract Single-nucleotide polymorphisms in the brain-derived neurotrophic factor gene may affect the secretion and function of brain-derived neurotrophic factor, thereby affecting the occurrence, severity and prognosis of ischemic stroke. This case-control study included 778 patients (475 males and 303 females, mean age of 64.0 ± 12.6 years) in the acute phase of ischemic stroke and 865 control subjects (438 males and 427 females, mean age of 51.7 ± 14.7 years) from the Department of Neurology, West China Hospital, Sichuan University, China between September 2011 and December 2014. The patients' severities of neurological deficits in the acute phase were assessed using the National Institutes of Health Stroke Scale immediately after admission to hospital. The ischemic stroke patients were divided into different subtypes according to the Trial of Org 10172 in Acute Stroke Treatment classification. Early prognosis was evaluated using the Modified Rankin Scale when the patients were discharged. Genomic DNA was extracted from peripheral blood of participants. Genotyping of rs7124442 and rs6265 was performed using Kompetitive Allele Specific polymerase chain reaction genotyping technology. Our results demonstrated that patients who carried the C allele of the rs7124442 locus had a lower risk of poor prognosis than the T allele carriers(odds ratio [OR] = 0.67; 95% confidence interval [CI]: 0.45-1.00; P = 0.048). The patients with the CC or TC genotype also exhibited lower risk than TT carriers (OR = 0.65; 95% CI: 0.42-1.00; P = 0.049). The AA genotype at the rs6265 locus was associated with the occurrence of ischemic stroke in patients with large-artery atherosclerosis (OR = 0.58; 95% CI: 0.37-0.90; P = 0.015). We found that the C allele (CC and TC genotypes) at the rs7124442 locus may be protective for the prognosis of ischemic stroke. The AA genotype at the rs6265 locus is likely a protective factor against the occurrence of ischemic stroke in patients with large-artery atherosclerosis. The study protocol was approved by the Ethics Committee of West China Hospital of Sichuan University, China (approval ID number 2008[4]) on July 25, 2008.
Key Words: nerve regeneration; ischemic stroke; brain-derived neurotrophic factor; single-nucleotide polymorphism; risk; stroke severity;prognosis; rs6265; rs7124442; neural regeneration
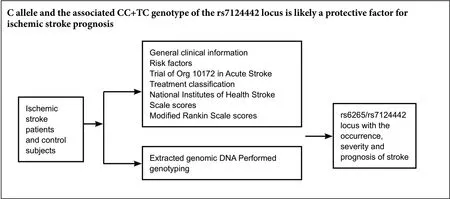
Graphical Abstract
Introduction
Stroke is a common, frequently occurring disease that seriously harms human health. The results from an epidemiological survey on cerebrovascular diseases in China showed that the age-corrected prevalence, annual incidence and mortality rates of stroke were 1114.8/100,000, 246.8/100,000,and 114.8/100,000, respectively (Wang et al., 2017). Ischemic stroke is the most common type of stroke, accounting for 69.6-77.8% of all stroke cases (Wang et al., 2017). Brain-derived neurotrophic factor (BDNF) is one of the members of the neurotrophic factor family. Mature BDNF is an alkaline protein with 119 amino acid residues and a relative molecular weight of 14 kDa (Mowla et al., 2001). It is mainly synthesized and secreted by neurons and glial cells in the central nervous system (Mowla et al., 2001; Wurzelmann et al., 2017). There are two secretory modes of BDNF: constitutive release and activity-dependent release (Poo, 2001). In recent years, studies have suggested that BDNF plays important roles in neuroprotection, neuroplasticity and neuroregeneration (Lee et al., 2003;Machaliński et al., 2012; Zhao et al., 2017).
The secretion and functions of BDNF depend on the expression of the BDNF gene. Single-nucleotide polymorphisms are one of the most common types of human genetic variation.Single-nucleotide polymorphisms in the BDNF gene may affect BDNF secretion and/or function, thereby affecting the incidence, severity and prognosis of ischemic stroke (Egan et al.,2003; Orefice et al., 2013; Kotlęga et al., 2017). A large number of single-nucleotide polymorphisms in the BDNF gene are known. It has been reported that the mutation at the rs7124442(C/T) locus in the 3′-untranslated region (3′UTR) of the BDNF gene is associated with the recovery of cognitive functions after traumatic brain injury (Rostami et al., 2011), but few studies on this topic have been published. No studies have reported on the correlation between nucleotide variations at this locus and susceptibility to ischemic stroke, neurological deficits during the acute phase of ischemic stroke and ischemic stroke prognosis.Additionally, rs6265 (A/G) is one of the most studied and most clinically significant single-nucleotide polymorphism loci of the BDNF gene (Kotlęga et al., 2017). Rs6265 is a missense mutation located in the exon of the BDNF gene and is present in approximately 30-50% of the population (Shimizu et al., 2004).This mutation of G to A changes the amino acid at position 66 of the BDNF precursor protein (pro-BDNF) from valine to methionine (Val66Met). Although this missense mutation does not affect the function and basic secretion of BDNF, it causes a 25% reduction in the activity-dependent secretion of BDNF(Egan et al., 2003). However, the results from existing clinical studies on the correlations of polymorphism at the rs6265 locus with ischemic stroke susceptibility and prognosis are not entirely consistent (Cramer et al., 2012; Kim et al., 2012, 2013; Zhao et al., 2013; Stanne et al., 2014; Keshavarz et al., 2016). Animal studies have found a decrease in BDNF levels in the central nervous systems of knock-in mice with a BDNF (Met/Met) mutation; this reduction was associated with the severity of motor defects (Qin et al., 2011). However, the rs6265 polymorphism has not been found to be associated with the severity of neurological deficits during the acute phase of ischemic stroke in clinical studies (Zhao et al., 2013; Stanne et al., 2014).
This study investigated the correlations of BDNF polymorphism at the rs7124442 locus with the occurrence, severity and prognosis during the acute phase in ischemic stroke patients in the Han population of southwest China. The rs6265 locus was also examined for the presence of the these correlations in ischemic stroke patients.
Participants and Methods
Participants
This was a case-control study. Ischemic stroke patients treated and registered at the Department of Neurology in West China Hospital, Sichuan University, China, from September 2011 to December 2014 were recruited. The 2010 China Guidelines for Diagnosis and Treatment of Acute Ischemic Stroke was used as the reference for the diagnostic criteria adopted in this study(Acute Ischemic Stroke Diagnosis and Treatment Writing Group of Cerebrovascular Disease in Neurology Branch of Chinese Medical Association, 2010). Assessments were made by more than two neurologists. These neurologists took part in the study, and were blind to the participants' genotypes. The specific inclusion criteria were as follows: patients aged ≥18 years in the Han ethnic population of southwest China; patients who met the ischemic stroke diagnostic criteria and were admitted to hospital within 7 days of disease onset; patients who had ischemic stroke lesions confirmed by computed tomography or magnetic resonance imaging; and patients who had new-onset acute ischemic stroke or who had a history of stroke but with no residual dysfunction (score ≤ 1 point on a modified Rankin scale) (Cheng et al., 2014). The exclusion criteria were as follows: subjects with transient cerebral ischemia or hemorrhagic stroke (but not excluding hemorrhagic transformation after ischemic stroke); and subjects with complications of primary subarachnoid hemorrhage, subdural hematoma, cerebrovascular malformations, intracranial venous thrombosis or intracranial tumors. The subjects in the control group were recruited from the Department of Neurology of West China Hospital over the same period. They showed no history of stroke during clinical examination and cerebral infarction lesions in cranial imaging (computed tomography or magnetic resonance imaging). The exclusion criteria of the control group were the same as those of the ischemic stroke group.
Written informed consent was obtained from all participants or their next-of-kin, when participants were unable to communicate or write. The study protocol was approved by the Ethics Committee of West China Hospital, Sichuan University, China (approval ID number 2008[4]) on July 25,2008 (Additional file 1) and conducted in accordance with the ethical guidelines of the 1975 Declaration of Helsinki. The study flow chart is shown in Figure 1. This study follows the Standard Protocol Items: STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) guidance for study (Additional file 2).
Collection of clinical information
General clinical information, such as age and sex, along with the assessment of risk factors, including history of hypertension, diabetes, hyperlipidemia, atrial fibrillation, smoking and drinking, were collected by neurologists. Ischemic stroke was divided into the following five types according to the Trial of Org 10172 in Acute Stroke Treatment (TOAST) classification:large-artery atherosclerosis, cardioembolism, small-artery occlusion, stroke of other determined etiologies and stroke of undetermined etiology (Adams et al., 1993). Meanwhile, the severity of their neurological deficits in the acute phase immediately after admission to the hospital was assessed using the National Institutes of Health Stroke Scale (NIHSS) (Lyden,2017). A stroke with an NIHSS score ≤ 6 was considered mild, while a stroke with an NIHSS score ≥ 7 was considered severe. Early prognosis was evaluated using Modified Rankin Scale (mRS) scores (Cheng et al., 2014) from ischemic stroke patients when they were discharged. Patients with mRS scores≤ 1 were considered as having good prognoses, while those with mRS scores ≥ 2 were considered as having poor prognoses. The above criteria were employed to remain consistent with the criteria adopted in existing relevant studies on the correlation between BDNF single-nucleotide polymorphisms and ischemic stroke to facilitate the comparison of findings from different populations (Zhao et al., 2013; Stanne et al.,2014).

Figure 1 Study flow chart.
Blood sample collection
Fasting peripheral venous blood samples (5 mL) were collected from superficial veins of the upper extremity at the elbow of each participant in the morning, with ethylenediamine tetraacetic acid as the anticoagulant. The samples were then stored at -20°C for extraction of genomic DNA from whole blood.
Genotyping
Genomic DNA was extracted from peripheral blood using an AxyPrep Blood Genomic DNA Maxiprep Kit (Axygen,Union City, CA, USA). Genotyping of rs7124442 and rs6265 was performed using Kompetitive Allele Specific polymerase chain reaction genotyping technology (LGC Genomics, formerly KBioscience, http://www.lgcgenomics.com/).
Statistical analysis
To compare differences in the clinical backgrounds of the participants, SPSS for Windows (Version 21.0, IBM, Armonk,NY, USA) was employed for chi-square or independent samples t-test analyses. The Hardy-Weinberg equilibrium test was performed using the SHEsis software (Shi and He, 2015).Three common genetic analysis methods (allele frequency,dominance model and recessive model) were used to analyze the correlations between polymorphism of the selected locus and the risk, severity of neurological deficits and early prognosis of ischemic stroke. If “A” represents wild type and “a” represents mutant type, the methods of allele mean participants with the a alleles versus those with the A allele,while the dominance model means aa + Aa versus AA; the recessive model means aa versus Aa + AA. Chi-square testing was employed to analyze the distribution of allele frequencies between the ischemic stroke and control groups. Logistic regression analysis was used in the dominant and recessive models to correct for the relevant risk factors (sex, age, smoking history, history of alcohol consumption, hypertension, diabetes, hyperlipidemia and atrial fibrillation). The three types of analyses described above were performed using PLINK v1.07 (http://pngu.mgh.harvard.edu/purcell/plink/) (Purcell et al., 2007). Values of P < 0.05 were considered statistically significant.
Results
Baseline characteristics of ischemic stroke cases and controls
A total of 778 ischemic stroke patients and 865 control participants were included in this study. The comparison of general clinical information between the two groups is shown in Table 1. The differences in age and sex were statistically significant between the two groups (P < 0.001). Among the common risk factors for ischemic stroke, the proportions of participants with hypertension, diabetes, hyperlipidemia, atrial fibrillation and history of smoking were significantly higher in the ischemic stroke group than those in the control group(P < 0.001). No significant differences were found in alcohol consumption between the ischemic stroke and control groups(P = 0.132).
The results from the TOAST classification are shown in Table 1. The ischemic stroke group included 281 cases with large-artery atherosclerosis. Statistically significant differences were found in age and sex between the large-artery atherosclerosis group and the control group (P < 0.001). Rates of hypertension, diabetes and history of smoking or drinking were higher in the large-artery atherosclerosis group than in the control group (all P < 0.05). There were 160 cases of cardioembolism in the ischemic stroke group, with a significant difference in age when compared with the control group(P < 0.001). The rates of hypertension, diabetes and atrial fibrillation were all higher in the cardioembolism group than those of the control group (P < 0.001). A total of 210 cases of small-artery occlusion were included in the ischemic stroke group. Significant differences in age (P = 0.002) and sex (P <0.001) were detectable between the ischemic stroke group and the control group (P < 0.01). The rates of hypertension, diabetes, hyperlipidemia and history of smoking were significantly higher in the small-artery occlusion group than in the control group (all P < 0.05).
As shown in the analysis of the subtypes of the ischemic stroke group in Table 2, 477 mild stroke patients (61.3%)(NIHSS score ≤ 6) and 301 (38.7%) severe stroke patients(NIHSS score ≥ 7) were included. No significant differences were observed in sex, age, or rates of hypertension, diabetes,hyperlipidemia or history of drinking or smoking between the two groups (P > 0.05). However, the rate of atrial fibrillation was lower in the mild stroke group than that of the severe stroke group (P < 0.001). There were 189 patients (24.3%)with good prognosis (mRS score ≤ 1; good prognosis group)and 589 patients (75.7%) with poor prognosis (mRS score ≥2; poor prognosis group). These two groups exhibited no significant differences in sex, age, rate of diabetes or hyperlipidemia or history of drinking or smoking (P > 0.05). However,the rate of atrial fibrillation in the good prognosis group was lower than that in the poor prognosis group (P = 0.045). The rate of hypertension was higher in the good prognosis group than in the poor prognosis group (P = 0.022).
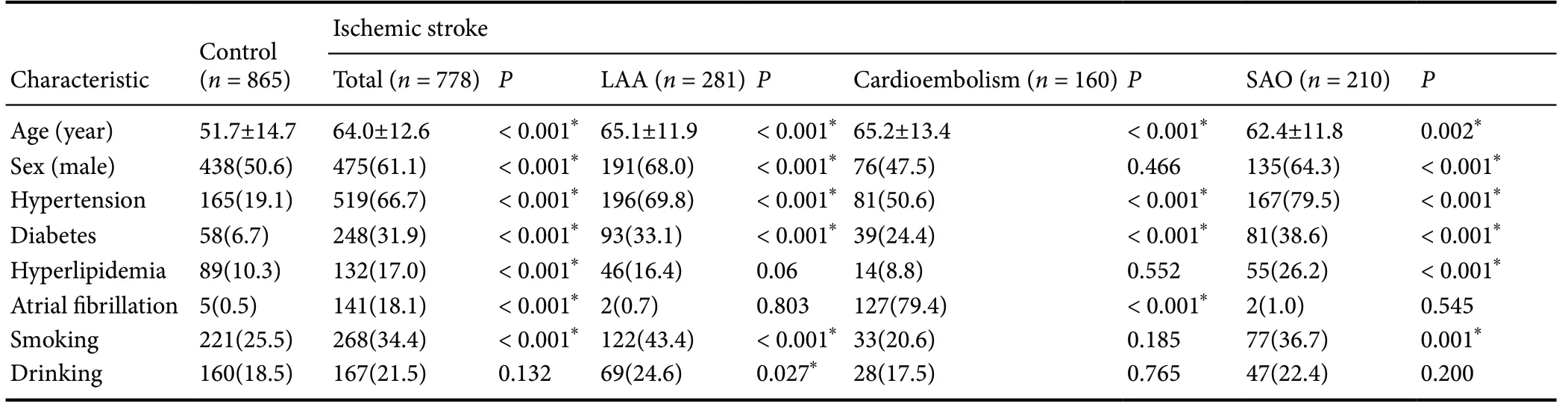
Table 1 Baseline characteristics of ischemic stroke cases and controls

Table 2 Baseline characteristics of ischemic stroke subtypes
Genotype and allele frequency distributions of single-nucleotide polymorphisms in ischemic stroke cases and controls
As shown in Tables 3 and 4, in the comparative analysis between the control group and the subtype groups based on TOAST classification in ischemic stroke patients, we performed logistic regression analysis for the rs7124442 locus to correct for potential confounding factors (sex, age, smoking, drinking, hypertension, diabetes, hyperlipidemia and atrial fibrillation), and no correlations were found between the rs7124442 polymorphism and the ischemic stroke subtypes (P > 0.05). However,after logistic regression analysis was performed for the rs6265 locus with the correction of potential confounding factors (sex,age, smoking, drinking, hypertension, diabetes, hyperlipidemia and atrial fibrillation), a negative correlation was found between the AA genotype (recessive model) and the occurrence of ischemic stroke in patients with large-artery atherosclerosis (odds ratio, OR = 0.58; 95% confidence interval, 95% CI: 0.37-0.90;P = 0.015). Polymorphisms at the rs6265 locus were found not to correlate with the risk of ischemic stroke or the incidence of cardioembolism or small-artery occlusion (P > 0.05).
rs7124442 and rs6265 genotypes/allele frequencies distribution and association with stroke severity at admission
The allele and genotype distribution frequencies in the mild and severe stroke groups are shown in Table 5. No significant differences were found in allele frequencies at the rs7124442 and rs6265 loci in the intergroup comparison (P > 0.05). Logistic regression analysis revealed that the dominant and recessive models of the rs7124442 and rs6265 loci had no correlation with the severity of the neurological deficits during the acute phase (P > 0.05). Because the distribution frequency of the CC genotype at the rs7124442 locus was zero in the severe stroke group, recessive model analysis was not performed.
rs7124442 and rs6265 genotypes, allele frequency distributions and association with stroke acute functional outcome
The allele and genotype distribution frequencies in the good prognosis group (mRS score ≤ 1) and the poor prognosis group (mRS score ≥ 2) during the acute phase are shown in Table 6. In the intergroup comparison between the patients with good prognosis and those with poor prognosis, the risk of poor prognosis was lower in patients who carried a C allele at the rs7124442 locus than in T allele carriers (OR =0.67; 95% CI: 0.45-1.00; P = 0.048). After logistic regression analysis was performed to correct for potential confounding factors (sex, age, smoking, drinking, hypertension, diabetes,hyperlipidemia and atrial fibrillation), the risk was lower in patients with the CC or TC genotype than TT carriers (OR =0.65; 95% CI: 0.42-1.00; P = 0.049).
The allele frequency of rs6265 was not significantly different between the two groups (P > 0.05), and the dominant and recessive models exhibited no correlation with prognosis (P > 0.05).

Table 3 Genotypes and allele frequencies between ischemic stroke cases and controls

Table 4 Genotypes and allele frequencies between TOAST subtype and controls
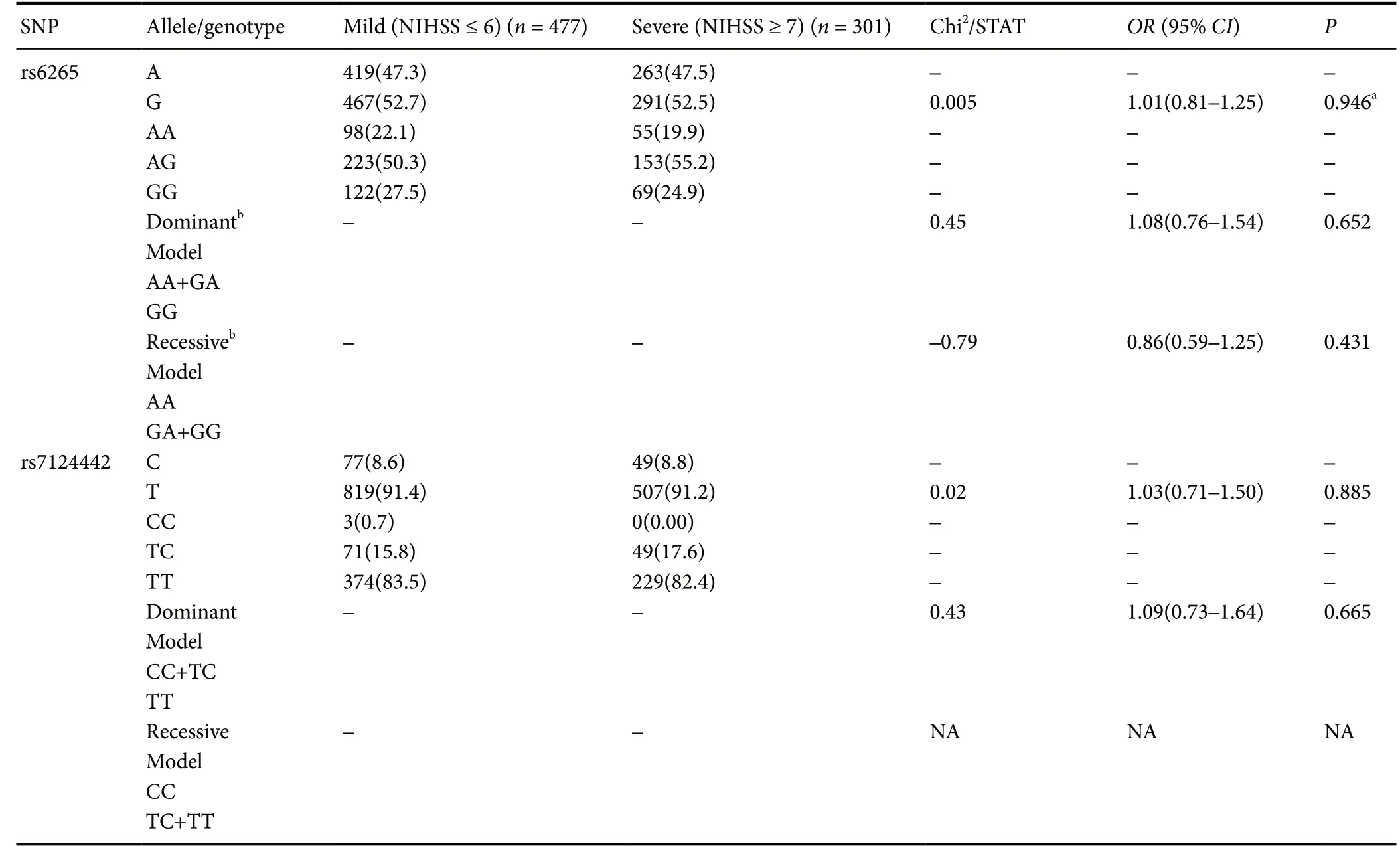
Table 5 Genotype and allele frequency distributions and association with severity at admission
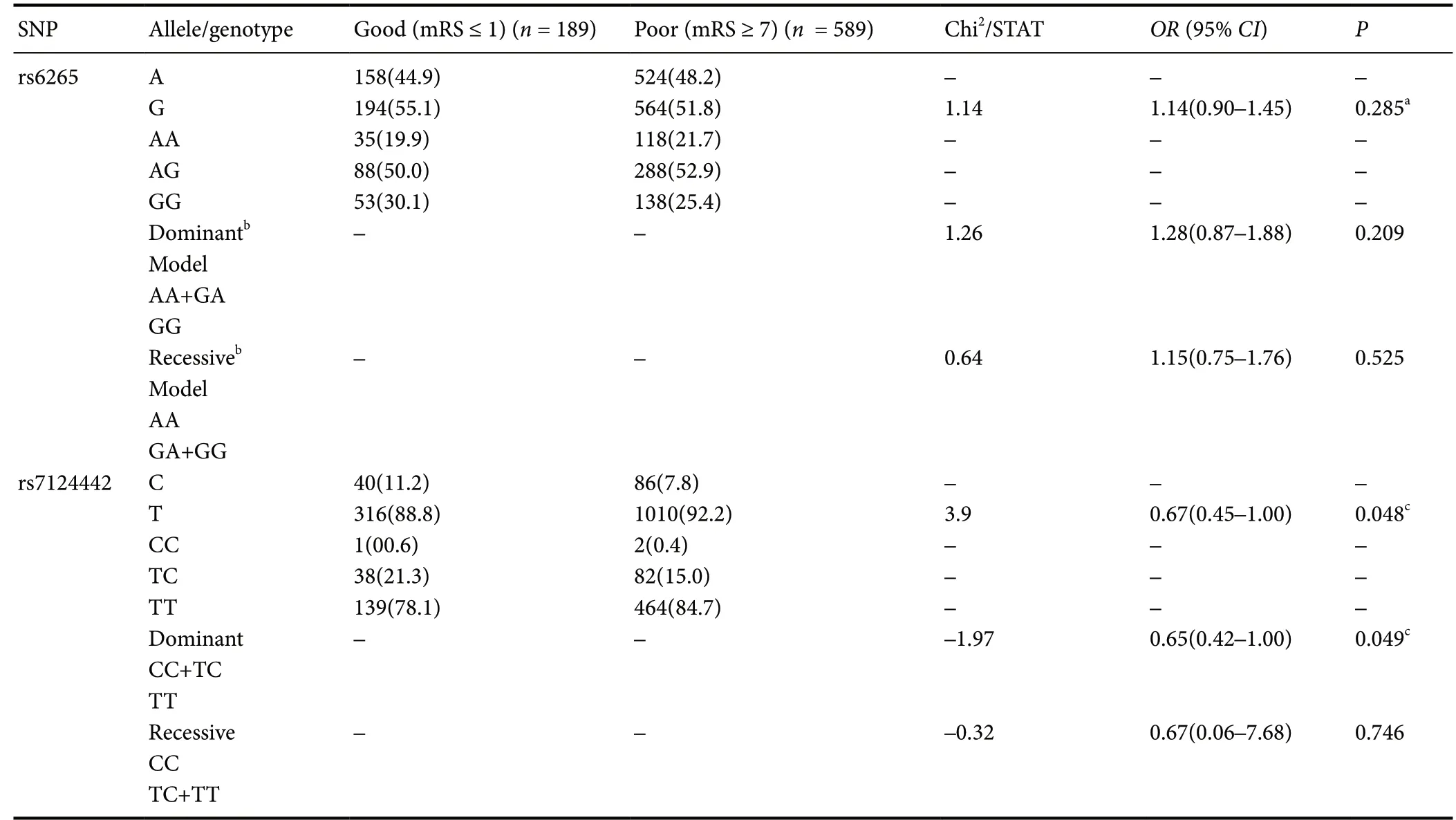
Table 6 Genotype and allele frequency distributions and association with acute functional outcome
Discussion
In this study, for the first time, we studied the correlations between polymorphism at the BDNF rs7124442 (C/T) locus and acute ischemic stroke. We discovered that patients carrying a C allele at the rs7124442 locus showed a lower risk for poor prognosis than T allele carriers (OR = 0.67; 95% CI: 0.45-1.00;P = 0.048). Additionally, the risk of poor prognosis in carriers of the CC or TC genotype (dominant model) was significantly lower than that in the carriers of the TT genotype (OR = 0.65;95% CI: 0.42-1.00; P = 0.049). We also found a correlation between the AA genotype (recessive model) at the rs6265 locus of the BDNF gene and the incidence of ischemic stroke in patiants with large-artery atherosclerosis (OR = 0.58; 95% CI: 0.37-0.90;P = 0.015).
The rs7124442 (C/T) locus is in the long 3′UTR of the BDNF gene. This untranslated sequence is immediately adjacent to the coding sequence in the mRNA and plays important roles in the post-transcriptional regulation of genes, such as involvement in mRNA transport and translation efficiency (Mignone et al.,2002). A study has shown that variations of polymorphisms at the rs7124442 (C/T) locus are associated with cognitive recovery after traumatic brain injury (Rostami et al., 2011), but there are still relatively few studies on this topic. No studies have reported on the correlation between polymorphisms at this locus with ischemic stroke susceptibility, neurological deficits during the acute phase and prognosis.
We are the first to study the correlation between polymorphism at the rs7124442 locus and acute ischemic stroke. The 3′UTR plays important regulatory roles in the transcription and translation of genes. Two studies found no significant associations between the rs7124442 (C/T) locus and BDNF levels(Hohenadel et al., 2014; Failla et al., 2016). However, one study found that rs7124442 in the long 3′UTR inhibited dendritic localization of BDNF mRNA (Orefice et al., 2013). Further mechanistic studies are needed to clarify how rs7124442 (C/T)locus polymorphism can influence the prognosis of stroke. No correlation was found between rs7124442 and ischemic stroke susceptibility and the severity of neurological deficits during the acute phase.
In this study, only the AA genotype (recessive model) at the rs6265 locus of the BDNF gene was negatively correlated with the occurrence of ischemic stroke in patients with large-artery atherosclerosis (OR = 0.58; 95% CI: 0.37-0.90; P = 0.015). This finding is not consistent with the results of previous studies.Zhao et al. (2013) found a correlation between the AA genotype of the rs6265 locus and the incidence of ischemic stroke, but no such correlation in subtype analyses. Additionally, in an Iranian population, Keshavarz et al. (2016) found that the GA or GG genotypes at the rs6265 locus are associated with the incidence of ischemic stroke. This discrepancy is likely due to different the populations included in these studies. This study only included the Han population in southwest China, while the population studied by Zhao et al. (2013) was mainly from the Shanghai area.
Other research has shown that BDNF may be associated with neurological deficits in the central nervous system. For example, Qin et al. (2011) found that knock-in mice with a BDNF mutation (Met/Met) had reduced BDNF levels in the central nervous system when compared with wild-type mice(Val/Val); this reduction was associated with motor function impairment severity. However, no correlations were found between the rs6265 polymorphism and the severity of neurological deficits during the acute phase of ischemic stroke in our study. In fact, this finding is consistent with the results from previous clinical studies in China and other countries (Zhao et al., 2013; Stanne et al., 2014). However, this finding is not consistent with the results of animal studies by Qin et al. (2011),though the reasons for this inconsistency require further investigation. One possible reason is that the factors affecting the severity of neurological deficits in the human body are more diverse than those in an animal ischemic stroke model and that the interactions between these factors are more complex.
When ischemic stroke prognosis was assessed using mRS scores, the current findings on the rs6265 polymorphism and prognosis were not consistent. In this study, the rs6265 polymorphism was not found to be associated with early ischemic stroke prognosis. Furthermore, no correlations were found between the rs6265 polymorphism and the prognosis of ischemic stroke patients in populations from Europe and the US (Cramer et al., 2012; Stanne et al., 2014). However, a study in the Korean population showed that the rs6265 polymorphism was not associated with prognosis at 30 days after ischemic stroke, but was associated with prognosis at 90 days after ischemic stroke(Kim et al., 2013). In another study of the Korean population,rs6265 polymorphism was found to be associated with poor prognosis at 14 days and 1 year after ischemic stroke (Kim et al., 2012). In the Chinese population, Zhao et al. (2013) found that the AA genotype was associated with poor prognosis at 90 days after ischemic stroke. The differences in these findings suggest that the rs6265 polymorphism exhibits differences in different races. Therefore, our results require further confirmation in different races with large samples.
There are some limitations in this study. First, this study is a single-center study with a small sample size. The patients showed significant differences in age and sex when compared with the control group. Our results need further confirmation through multi-center studies of larger sample sizes matched in sex and age, because ischemic stroke is a complex disease that has a high incidence and is influenced by multiple gene interactions, the environment, and lifestyle. Second, this study only included the Han population in southwestern China,and its findings need to be further verified in different ethnic populations in different regions. Third, only two hotspot single-nucleotide polymorphisms of the BDNF gene were selected in this study, and the correlations between ischemic stroke and other BDNF single-nucleotide polymorphisms should be elucidated in subsequent studies to further clarify the relationship between the BDNF gene and ischemic stroke. Finally, this study included patients with ischemic stroke within 7 days of onset; the NIHSS score was assessed on the day of admission to assess the severity of neurological deficits, and the mRS score was evaluated on the day of discharge for early prognosis. Therefore, the two assessments of the patients may not be on the same timeline. Additionally, the observation period for ischemic stroke prognosis was short. The correlations between BDNF gene polymorphisms and long-term ischemic stroke prognosis should be further observed in follow-up studies.
For the first time, we discovered that the C allele (CC or TC genotypes) at the rs7124442 locus is likely a protective factor for ischemic stroke prognosis. We also found that the AA genotype of rs6265 is possibly a protective factor for the occurrence of ischemic stroke in patients with large-artery atherosclerosis. The mechanisms underlying the above observations should be further verified in subsequent studies.
Author contributions:Study design, data analysis and interpretation, experimental implementation, and manuscript writing: JZ and MMM; experimental implementation and statistically analysis: JHF; data collection and experimental implementation: LZ; data collection: MKZ; study design and manuscript revision critically for important intellectual content: JG and LH.All authors approved the final version of the paper.
Conflicts of interest:The authors declare that there is no conflict of interests regarding the publication of this paper.
Financial support:The study was supported by the National Natural Science Foundation of China, No. 81472162 (to MKZ). The funding body played no role in the study design, in the collection, analysis and interpretation of data, in the writing of the paper, or in the decision to submit the paper for publication.
Institutional review board statement:This study was approved by the Ethics Committee of West China Hospital, Sichuan University, China (approval No. 2008(4)) on July 25, 2008. The study was performed in accordance with the relevant laws and regulations of the Declaration of Helsinki, and the hospital's relevant ethical principles.
Declaration of patient consent:The authors certify that they obtained patients' or their guardians' consent forms. In the forms, patients or their guardians have given their consent for the patients' images and other clinical information to be reported in the journal. The patients or their guardians understand that the patients' names and initials will not be published and due efforts will be made to conceal their identity.
Reporting statement: This study followed the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) statement.
Biostatistics statement: The statistical methods of this study were reviewed by the biostatistician of West China Hospital of Sichuan University, China.
Copyright license agreement:The Copyright License Agreement has been signed by all authors before publication.
Data sharing statement:Individual participant data that underlie the results reported in this article, after deidentification (text, tables, figures, and appendices) will be in particular shared. Study protocol and informed consent form will be promulgated within 6 months after the completion of the trial.Anonymized trial data will be available indefinitely at www.figshare.com.
Plagiarism check: Checked twice by iThenticate.
Peer review:Externally peer reviewed.
Open access statement:This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
Open peer reviewer: Clarissa Cavarsan, Universidade Federal do Paraná,Brazil.
Additional files:
Additional file 1:Ethics committee approval (Chinese).
Additional file 2:STROBE checklist.

- 中国神经再生研究(英文版)的其它文章
- Improvement of ataxia in a patient with cerebellar infarction by recovery of injured cortico-ponto-cerebellar tract and dentato-rubro-thalamic tract: a diffusion tensor tractography study
- Tandem pore TWIK-related potassium channels and neuroprotection
- Dendritic shrinkage after injury: a cellular killer or a necessity for axonal regeneration?
- Regenerative biomarkers for Duchenne muscular dystrophy
- Exploring the efficacy of natural products in alleviating Alzheimer's disease
- Role of macrophages in peripheral nerve injury and repair