
Efficacy of Detoxsan® powder on diarrhea caused by gastrointestinal neuroendocrine tumors
2019-05-13 01:14:00ThomasLangbeinilfriedDatheAnikaDeuerlingRichardBaum
World Journal of Gastroenterology 2019年17期
Thom as Langbein, W ilfried Dathe, Anika Deuerling, Richard P Baum
Abstra c t
Key words: Neuroendocrine tumor; Diarrhea; Carcinoid syndrome; Treatment;Clinoptilolite; Mordenite; Zeolite
INTRODUCTION
There are d iverse etio logies o f d iarrhea due to d ifferen t or tissue-dependen t m echanism s[1]. Chronic d iarrhea can be caused by neu roendocrine tum ors (NETs) of the gastroin testinal tract (p reviously called “carcinoids”), w hich lead to significantly reduced quality of life. App lication of synthetic analogues of som atostatin[2]is one of the established treatm ent op tions to control characteristic sym p tom s like flushing and d iarrhea as w ell as to inhibit tum or grow th. A significant p roportion of patients m ight stop respond ing to som atostatin analogue therapy or this treatm en t alone m ight not achieve adequate sym p tom relief. Therefore, new and active substances are certain ly required to alleviate relevan t sym p tom bu rden like d iarrhea. A p rospective phase III clinical study using Telotristat Etip rate (Xerm eloTM), a novel serotonin syn thesis inhibitor, reported a significan t decrease in daily bow el m ovem en ts frequency,decrease in serotonin p roduction and increase in quality of life[3,4]. Telotristat Etip rate is a tryp tophan hyd roxy lase inhibitor, and thereby reduces the p roduction o f serotonin and d im inishes daily bow el m ovem ents. Since 2017, Xerm eloTMis app roved in by the FDA as w ell as by EM A for the treatm en t of carcinoid synd rom e-relatedd iarrhea in com bination w ith som atostatin analog therapy[5]. It im p lies that the m ost recently app roved d rug is based on the inhibition of the p roduction of serotonin.
Serotonin or 5-hyd roxytryp tam ine (5-HT) is w ell know n as the cerebral ‘horm one of happ iness’, w hile the enteric 5-HT is a poly functional signaling m olecu le, acting as a paracrine factor, an endocrine horm one or a grow th factor, w hich is im portan t in gastroin testinal m otility, en teric neu rogenesis and in testinal in flamm ation[6].App roxim ately 95% of 5-HT is syn thesized in the gastroin testinal tract, stored in m u cosal en teroch rom affin cells an d released by m echan ical and chem ical stim u lations[7]. Spohn and M aw e[8]cou ld show that bacteria w ithin the lum en of the bow el in fluen ce sero ton in syn thesis and release by en teroch rom affin cells.Fu rtherm ore, co lon ep ithelial cells d irectly exposed to seroton in are p rim ed for in flamm atory reactions. Thus, the elevated serotonin level seem s to be an im portant innate imm une response, ind u ces in flamm atory genes in the gu t and m ay be responsib le at least partially for 5-HT-m ed iated pathogenesis in patien ts w ith inflamm atory bow el d isease[9]. On the other hand, the am ino acid tryp tophan acting as the p recu rsor of both serotonin and niacin (vitam in B3), w hich m ay induce niacin deficiency by uncontrolled serotonin p roduction as review ed[10]. The clinical com p lex appearance of NETs - the so called “carcinoid synd rom e” - is m ost frequently based on serotonin overp rodu ction and involves severe d iarrhea and flushing as w ell as bronchial obstruction, w heezing m uscle wasting as w ell as p roxim al m yopathy and m ay lead to carcinoid heart d isease consisting o f a secondary tricusp id valve insu fficiency due to endocard ial fibrosis[10]. Thus, serotonin dow n regu lation w ithin the gastrointestinal tract m ight cause reduction of bow el m ovem ents.
Natu ral zeolites are characterized by attractive by attractive p roperties su ch as ad sorp tion, ion-exchange and m olecu lar sieving. Due to the lattice structu re of the alum inosilicates w ith channels and cav ities, they possess an excellen t bind ing capacity for ions, toxins and other harm fu l substances, w hich p riv ilege them for m ed ical and biom ed ical ap p lications. Therefore, they are w idely used in d ietary sup p lem en ts, as active ingred ien ts in d rugs or carriers for d rugs, ad juvan ts in anticancer therapy and several other app lications[11-15]. In particu lar, the natu ral zeolite clinop tilolite has been trad itionally used in a large num ber of biom ed ical app lications,due to its physico-chem ical stability and biological com patibility. It has p roven to be an effective anti-d iarrheic d rug[16]. Fu rtherm ore, a m ajority of the patients su ffering from irritab le bow el synd rom e w ith d iarrhea responded effectively to artificially enhanced clinop tilo lite[17]. The natu ral Cuban zeolite used in this stud y is alread y availab le in Germ any as an extem poraneous m ixtu re (Detoxsan®Pu lver) and is com posed of tw o types of zeolite structures having d ifferent pore sizes: clinop tilolite,a m ed ium-pore 10-m em bered ring zeolite and m ordenite, a large-pore 12-m em bered ring zeolite[18]. M oreover, this Cuban zeolite is able to adsorb rem arkable am oun ts of the biogenic am ine histam ine and w ater[18-20]. It has been app lied for the first tim e to patien ts su ffering from severe d iarrhea caused by NETs. In d iarrhea related to m edu llary thy roid cancer, m ontm orillonite clay had been app lied successfu lly in 10 patients as a p ilot study[21]. M ontm orillonite clay belongs to the layered alum inium silicates w hile zeolites used in this study are characterized by 3-d im ensional crystal lattices w ith d ifferent characteristics[22,23].
MATERIALS AND METHODS
Patients
In the p resen t stud y, a total of 20 patien ts (12 fem ale and 8 m ale) su ffering from d iarrhea either by its frequency or from w atery stool caused by NET w ere included,age ranged from 39 and 83 years (m ean age of 64.1 years) (Table 1). In each patien t,the d iagnosis had been con firm ed by histology and som atostatin recep tors exp ression p roven by positron em ission tom ography/com pu ted tom ography using Ga-68-labeled som atostatin analogs[24]. A ll patien ts received stand ard-o f-care p harm acotherapy (Tab le 2) and w ere ad d itionally given Detoxsan®pow der (Detoxsan®Pu d er) as an ex tem p o raneou s d rug con tain ing 90% natu ral Cuban zeo lite(clinop tilo lite and m ordenite) and 10% m agnesium aspartate. In take of Detoxsan®pow der was comm enced w ith low doses of 3 × 1 g/d or 2 × 2 g/d and increased up to 3 × 3 g/d or 3 to 5 g every 4 h if necessary, as recomm ended in the literatu re abou t comm on non-in fectious d iarrhea for few days on ly[16]. Ind ividually tailored dose of Detoxsan®pow der w ill be m entioned in detail in the ‘Resu lts’ section. Each day dose and bow el m ovem ents w ere docum ented by the patients them selves in a p re-defined table.
Biochemical determinationsSerum serotonin levels w ere m easu red by a comm ercially availab le ELISA kit(Serotonin FAST ELISA, DRG Instrum ents Gm bH, M arbu rg, Germ any) accord ing to instructions given by the com pany. Incubation was perform ed at room tem peratu re for 15 m in and the antigen antibody com p lex containing serotonin was determ ined at 450 nm. U rea had been quan tified by a kinetic assay using u rease and g lu tam ate dehyd rogenase. In the first step u rea is sp lit by u rease in to amm onia and in the second enzym atic reaction the released amm onia form s L-g lu tam ate from 2-oxog lu tate using NADH. The rate o f decrease of NADH m easu red at 340 nm is d irectly p roportional to the concen tration of u rea in the assay[25]. Determ ination o f sing le ions was perform ed by ion-selective electrode (ISE) using comm ercially availab le equ ipm en t (Tecan’s Sun rise abso rban ce m icrop late reader). The electrochem ical sensors are help fu l too ls for qualitative and quan titative ion m easu rem ents[26]. Therefore, ISE serves as the standard m ethod in our laboratory.
G rad ing: O f neu roendocrine tum ors accord ing to WHO classification[29]; WD: W ell-d ifferen tiated neu roendocrine neop lasm; MD: M oderatelyd ifferentiated neuroendocrine neop lasm; CC: Coecum; CO: Colon; IL: Ileum; HBP: Hypertension or high blood p ressure.
RESULTS
A ll patients enrolled in this p ilot study d id not on ly su ffer from NETs, bu t also from com orbid ities and treatm en t-resistan t d iarrhea (Tab le 1). They took Detoxsan®pow der as an an tid iarrheal d rug, m oreover, the intake of loperam ide, w hich is a comm ercially available antid iarrheal d rug, was recomm ended as w ell (See Table 2).Nevertheless, in the p redefined tab le docum ented by the patien ts them selves, w e cou ld not found the intake of loperam ide by the patients.
The ind ividual dose of Detoxsan®pow der was adap ted by patients them selves w ith an increase until a significant reduction of bow el m ovem ents was reached (Figure 1)or a decrease if bow el m ovem ents frequency declined (Figure 2). In general, response effects need several days to becom e percep tible and require an intake of Detoxsan®pow der for an extended tim e period or interm itten tly, if persisting stabilization o f bow el m ovem ents cou ld not be achieved (Figu re 3). How ever, the use of Detoxsan®pow der d id not satisfy every patient or cou ld reduce bow el m ovem ents (Tables 3 and 4). Three patients cou ld not benefit even at a higher concentration and stopped dailyintake ahead of schedu le. Three patients reached on ly partial reduction of d iarrhea. In general, response rates o f Detoxsan®pow der ap pears to correlate w ith patien t’s nu trition, e.g. raw salad; fatty food and sauerk rau t w ere reported to have negative effects on d iarrhea desp ite intake of the pow der.
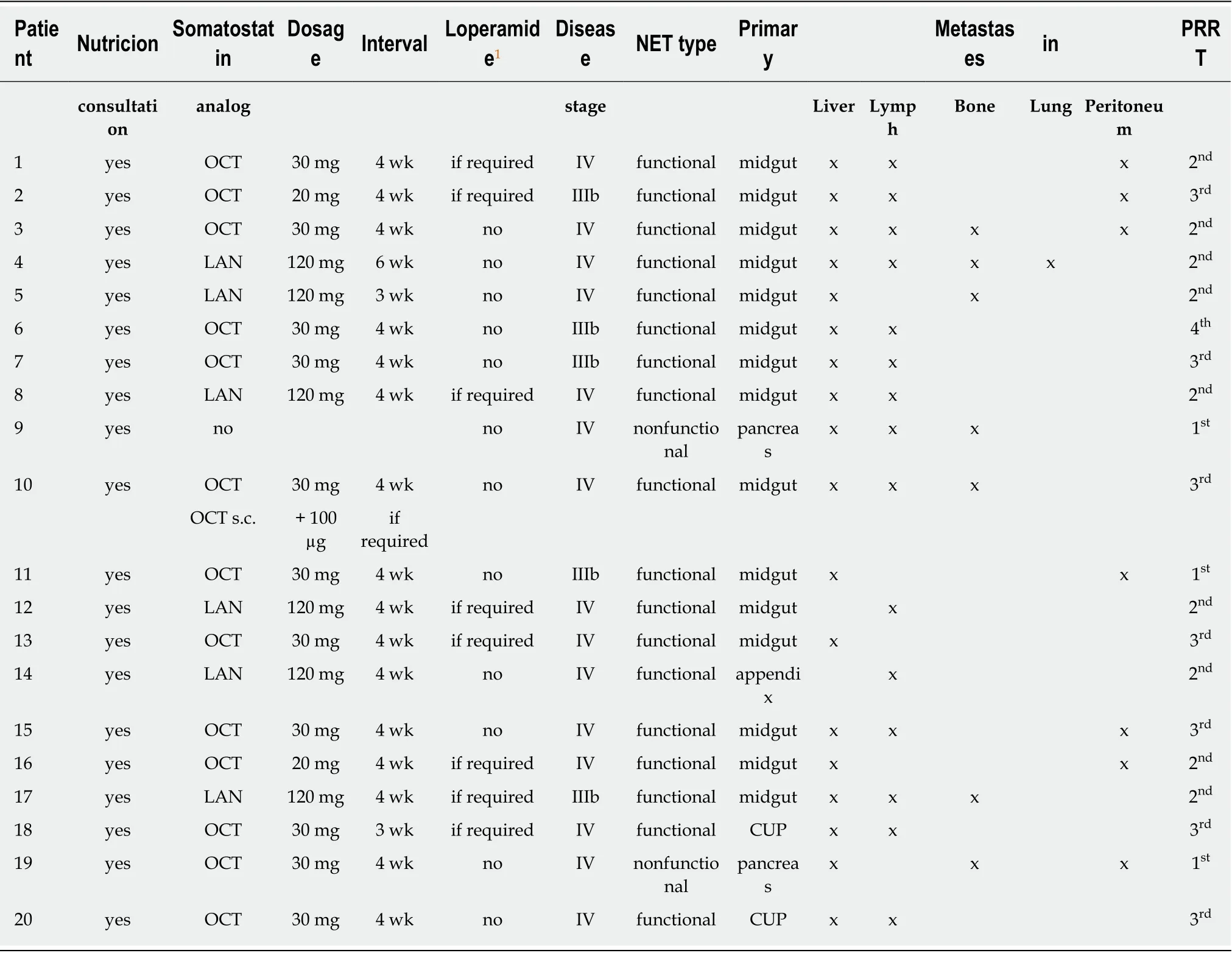
Table 2 Clinical parameters of the patients
In summ ary, 14 ou t of the 20 patients (70%) declared to be very content w ith using Detoxsan®pow der and observed a significan t redu ction o f d iarrhea, w hile the effective dose and intake period that resu lted in a sym p tom relief varied ind ividually(Table 3). M oreover, som e patients stopped oral app lication w hen bow el m ovem ent becam e regu lar, w hereas other patien ts extended in take in order to keep bow el m ovem ents at a low tolerable level. Apparently, that ind ividual decision seem ed to be dependen t on the to lerance of patien ts w ith the num ber o f bow el m ovem ents and stool consistency, in w hich a variance cou ld be observed. A correlation betw een NET grade, part and size of bow el resection and functionality of the tum or cou ld not be dem onstrated (Tables 1-3). Therefore, d iarrhea seem ed to be based on the m etabolic activity of the w ell-d ifferentiated NETs, w hich eventually led to treatm ent resistance.
The serum serotonin level appears to be one o f the m ajor factors responsible for d iarrhea in NETs[3-5], w hich is w hy b lood seroton in level was d eterm ined and recorded on follow-up (Tab le 5). On ly in 6 patien ts (patien ts 4, 5, 10, 14, 19, 20),serotonin level was m easu red in a short tim e in terval before and after in take o f Detoxsan®pow der. Independent of the potential w ide range of level of this biogenic am ine, there was a significan t decrease in the serotonin level du ring the period o f intake in all that cases. To evaluate if other comm on ly detected laboratory param eters are affected by Detoxsan®pow der in take, w e determ ined exem p larily the levels o f creatinine and u rea as w ell as the cations sod ium (Na), potassium (K) and calcium(Ca) in the blood (Table 5). In the creatinine and urea levels on ly a slight increase was m easu red during the use of Detoxsan®pow der w hile the investigated electrolytes d idnot exhibit any significant changes of their level.
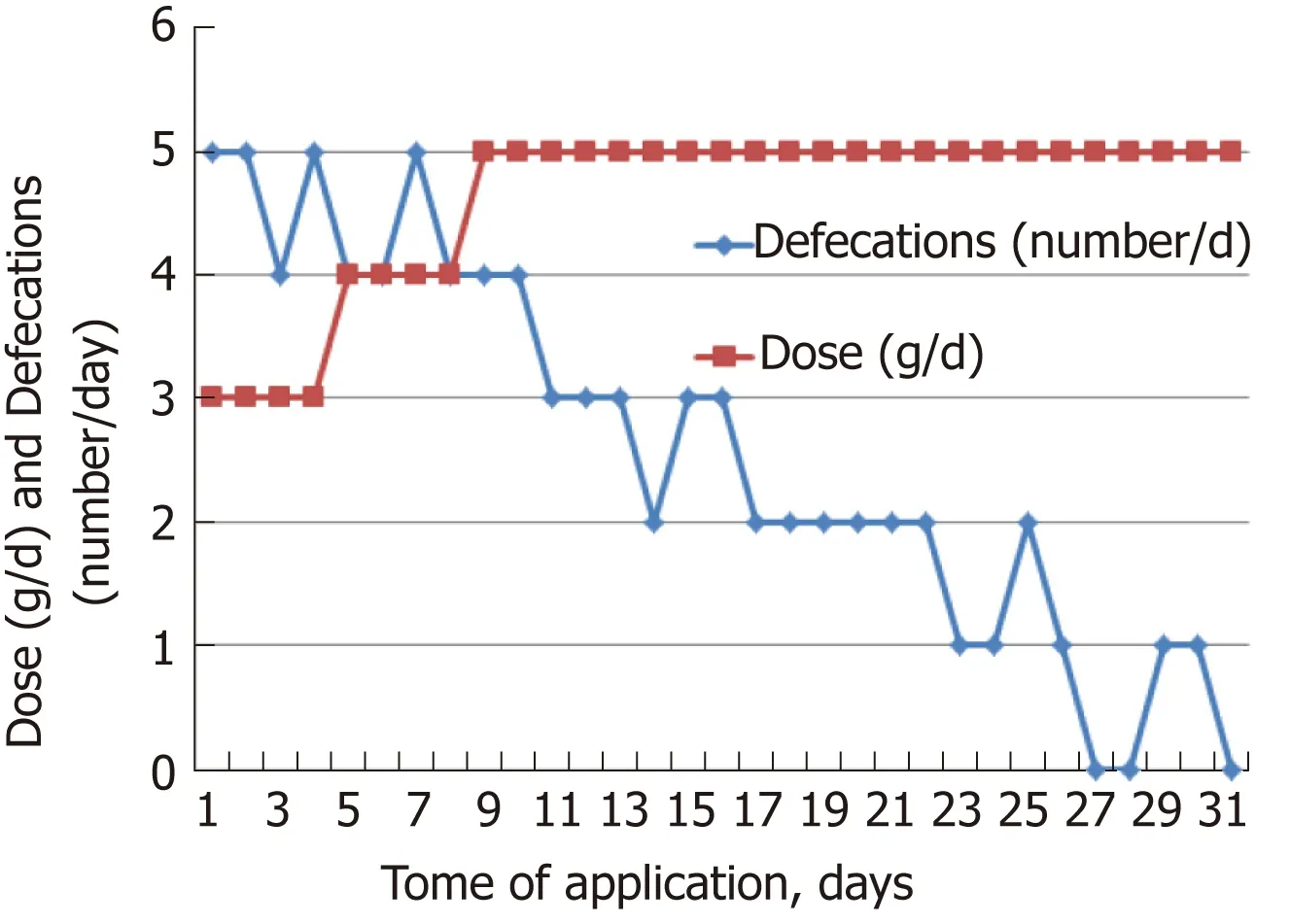
Figure 1 Application of Detoxsan® powder and frequency of bowel movement of a 77-year-old male patient.
DISCUSSION
A ll the patients enrolled in this p ilot study d id not on ly su ffer from NETs, bu t also from com orbid ities and treatm en t-resistan t d iarrhea due to reduced resorp tion capacity of the bow l w ith a consequen t in testinal failu re (Table 1)[27,28]. Grad ing and d ifferen tiation o f NETs w ere catego rized acco rd ing to the recen t WHO classification[29]. Length of bow el resection was included in the characterization o f patient status. Principally, patients w ere treated accord ing to the Theranostic concep t for NETs based on national and in ternational gu idelines[24]. How ever, there was insu fficient control of d iarrhea, m ost p robably due to the secretion of horm ones like serotonin p roduced by the slow ly grow ing and high ly d ifferentiated NETs[2].
W hether the serotonin level decrease in 6 patients is based on the adsorp tion o f serotonin by the zeo lite - sim ilar to the histam ine up take - or the decline of the chem ically-labile serotonin is caused by other m echanism s is still the sub ject o f ongoing investigations[18,19]. Nevertheless, these 6 patients w ere part of the satisfied ones w ith respect to the bow el m ovem ents (Table 2) correspond ing to correlation of serotonin level and d iarrhea[3-5]. For fu rther investigations it is w orth to determ ine the level of 5-hyd roxyindoleacetic acid in a 24-h u rine collection. It is a stable m etabolite of serotonin and by this w ay its level can be determ ined ind irectly[30]. It was not done in ou r p resent research.
Desp ite the know n facts that en teric seroton in is a po ly functional signaling m olecu le, an essential com ponent of the gastrointestinal inflamm atory response and a bioactive com ponen t in develop ing and m atu re anim als, the effect of this am ine on d iarrhea is still not com p rehensively understood[6]. In w eaning m ice e.g., stressinduced d iarrhea is considered to be caused by deregu lation of the m ucosal imm une system (am ong others). In teresting ly, m ucosal imm unity was decreased in the duodenum and jejunum w ithou t being affected in the ileum and colon[31,32]. Given the fact that the intestinal tract is the largest imm une organ of the hum an body, serotonin m igh t be therefore considered to be a link betw een the gu t and the imm une regu lation[33,34]. M oreover, histam ine is one of the m ost im portant biogenic am ines and strongly involved in imm unological reactions. It has been described as ‘an undercover agent in m u ltip le rare d iseases’, because m any pathological in flamm atory p rocesses are involved w ith histam ine as w ell[35].
The positive effect of zeolite on treatm ent-resistant d iarrhea caused by NETs m ight be related to several origins. H igh adsorp tion capacity for histam ine and possibly other biogenic am ines like serotonin, the antiph logistic effect of this m ineral as w ell as its high w ater up take capacity are poten tially responsible for reducing d iarrhea com p laints[18-20]. This kind of treatm ent d iffers significantly from all other d rugs in the field because Detoxsan®pow der acts on ly via its inherent adsorp tion p roperties w ithin the gastroin testinal tract; neither does it penetrate in to the b lood circu lation nor d irectly in fluence regu lation p rocesses. Fu rtherm ore, it is notew orthy that the histam ine up take of the Cuban zeo lite (and possib ly o f other biogenic am ines) is significantly higher com pared to other zeolites containing on ly clinop tilolite and no add itional m ordenite[19]. The clinical treatm ent of patients w ith NETs w ith regard to their functional com p lain ts is recen tly focused to the app lication o f som atostatin recep tor inhibitors[36]. Thus, the aim o f both m ethods appears sim ilar w hile the pharm acological app roach is quite d ifferent. The slight increase of the creatinine andu rea levels du ring the use o f Detoxsan®pow der m igh t be in terp reted as a m ild decrease in the kidney filtration p rocess w hile the m etabolic liver function seem s to be unaffected.

Figure 2 Application of Detoxsan® powder to a 64-year-old male patient.
In conclusion, the con tem poraneous m ixtu re Detoxsan®pow der is ab le to reduce significantly sym p tom s of NET-related d iarrhea in the m ajority of patients. The effect of this zeo lite seem s to be due to its high capacity to bind w ater, histam ine and possibly serotonin, too, w ithin the gastroin testinal tract and to rem oval o f those com pound s via stoo l. The du ration and dose o f Detoxsan®pow der in take varies ind ividually. In som e patien ts the norm alization o f bow el m ovem en t cou ld be observed w ithin a few w eeks w hile som e patients need to use it perm anently in order to m ain tain accep table quality of life w ithou t d iarrhea. Recomm ended daily dosage requires an ind ividual adap tation and ranges betw een 3 g once to three tim es per day.The clinical reduction of the d iarrhea sym p tom s by Detoxsan®pow der com es w ithou t a relevant negative in fluence on other biochem ical param eters.

Table 3 Effect of Detoxsan® powder on the bowel movements as evaluated by patients

Table 4 Diary of a 57-year-old male patient using Detoxsan® powder over 3 mo
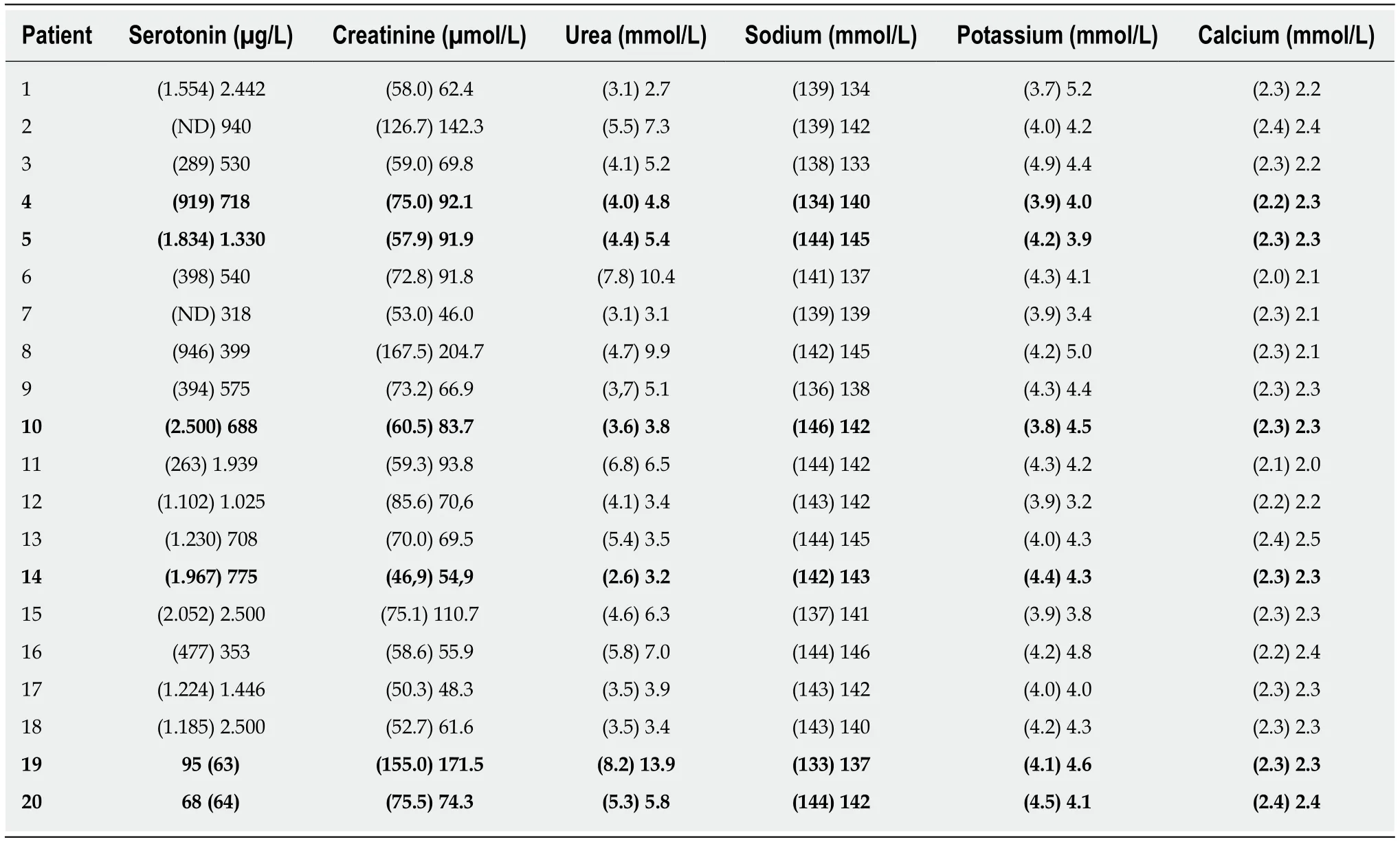
Table 5 Blood parameters determined before (in brackets) and after the application of Detoxsan® powder
Figure 3

Figure 3 Application of Detoxsan® powder to a 63-year-old male patient.
ARTICLE HIGHLIGHTS
Research background
Therapy-refractory d iarrhea in neu roendocrine tum or (NET) patien ts reduces quality o f life,strong ly restricts their daily rou tine and is therefore a high ly clinical unm et need.
Research motivation
M otivation of this investigation was reduce bow el m ovem en ts in chronic d iarrhea patients and by this to achieve a significant im p rovem en t in their quality of life.
Research objectives
To overcom e the therapy-refractory d iarrhea o f patien ts w ith NETs by the zeo lite con taining m ed ical advice Detoxsan®pow der.
Research methods
For this pu rpose, patients w ere o ffered a w ell characterized zeo lite p roduct w hich is know n to adsorb biogenic am ines and w ater in large extent and it does not enter in to the blood stream. The patien ts have been in form ed in detail abou t the p roduct, the ind ividual adap tation of the dosageand the docum en tation in a p redefined tab le. Due to the fact that d iarrhea synd rom e is a d istu rbance o f the daily rou tine the patien ts en ro lled in th is clin ical trial respected these recomm endations and show ed an excellen t com p liance. In add ition to the clin ical trial, w e determ ined som e biochem ical param eters in order to m onitor if som e undesired changes occu r.
Research results
It is the first tim e that a w ell characterized zeolite p roduct is ab le to reduce bow el m ovem en ts in patien ts su ffered by therapy-refractory d iarrhea caused by NETs over a long tim e. In 14 o f 20 patients (70%) enrolled in the trial bow el m ovem ent rate cou ld be norm alized. The app lication tim e to reach an accep table bow el m ovem ent oscillated betw een few w eeks up to a perm anent or in term ittent use. A lso the dosage oscillated betw een 3 g per day up to th ree tim es 3 g per day.A ll of the 14 responder patients app reciated the norm alization of the bow el m ovem ents in sp ite of the ind ividual adap tation of dosage and tim e. There w ere no side effects. H ow ever, it is not clear w hich factors in fluence the reduction of d iarrhea. A t least one com ponent nam ely serotonin seem s to be invo lved in this physio logical p rocess. Therefore, the adsorp tion of this biogenic am ine by this type o f zeolite is under investigation. Fu rtherm ore, the serotonin m etabo lite 5-hyd roxyindoleacetic acid shou ld be determ ined in a 24-h u rine collection. Using this m ethod the natu ral serotonin secretion can be determ ined ind irectly.
Research conclusions
The new find ing o f this study is the effective app lication o f a w ell characterized zeolite p roduct in patients su ffered by therapy-refractory d iarrhea caused by NETs. The attractive p roperties of the lattice structu re of this m ineral for excellent bind ing capacity for w ater, am ines and harm fu l substances seem to possess a key function in overcom e d iarrhea sym p tom s in both tem porary app lication and long term use. The ind ividual dosage and period of app lication in order to receive the best reduction o f d iarrhea ind icate that the physiological p rocess of these sym p tom s is no t fu lly understood and requ ires fu rther investigations. For the clin ical p ractice it is im portan t to accep t the ind iv iduality o f this treatm en t to overcom e patien t’s d iarrhea and im p rove their daily rou tine.
Research perspectives
W e observed that a w ell characterized natu ral zeolite is able to overcom e therapy-refractory diarrhea caused by NETs via passing the gastrointestinal tract only. How ever not all effects cou ld be answ ered satisfactorily. Therefore, futu re research shou ld be focused on the one hand to the adsorp tion of serotonin and other trigger substances for d iarrhea by this zeolite. On the other hand the clinical treatm en t of NETs patients requires the determ ination of the biochem ical factors in both b lood and faeces in correlation the resected bow el part and the effect of this zeolite. The aim of these investigations shou ld be the selective dosage of the m ineral p roduct on the basis of biochem ical values and/or surgical data.
 World Journal of Gastroenterology2019年17期
World Journal of Gastroenterology2019年17期
- World Journal of Gastroenterology的其它文章
- Tuberculous esophagomediastinal fistula with concomitant mediastinal bronchial artery aneurysm-acute upper gastrointestinal bleeding: A case report
- Transitions of care across hospital settings in patients with inflammatory bowel disease
- Beneficial effect of probiotics supplements in reflux esophagitis treated with esomeprazole: A randomized controlled trial
- Clinical value of preoperative methylated septin 9 in Chinese colorectal cancer patients
- Analysis of the autophagy gene expression profile of pancreatic cancer based on autophagy-related protein microtubule-associated protein 1A/1B-light chain 3
- Herbs-partitioned moxibustion alleviates aberrant intestinal epithelial cell apoptosis by upregulating A20 expression in a mouse model of Crohn’s disease