
Breathing adapted radiation therapy for leukemia relapse in the breast: A case report
2019-03-21 13:13OmerSagerFerratDincoglanSelcukDemiralBoraUysalHakanGamsizFatihOzcanOnurhanColakYeldaElcimBaharDiricanMuratBeyzadeoglu
World Journal of Clinical Oncology 2019年11期
Omer Sager, Ferrat Dincoglan, Selcuk Demiral, Bora Uysal, Hakan Gamsiz, Fatih Ozcan, Onurhan Colak,Yelda Elcim, Bahar Dirican, Murat Beyzadeoglu
Abstract BACKGROUND Infiltration of the breast by leukemic cells is uncommon but may manifest as an oncological emergency requiring prompt management. Extramedullary relapse of T-cell acute lymphoblastic leukemia (T-ALL) within the breast is exceedingly rare and there is paucity of data in the literature regarding this entity. No consensus exists on management of isolated extramedullary breast relapses of T-ALL.Herein, we report a case of isolated extramedullary breast relapse of T-ALL treated with breathing adapted radiation therapy (BART) using the active breathing control (ABC) system.CASE SUMMARY The patient was a 33-year-old female with diagnosis of T-ALL. She received intensive systemic chemotherapy that resulted in complete remission of her disease, and then underwent allogeneic hematopoietic stem cell transplantation.After a 15 mo period without symptoms and signs of progression, the patient presented with palpable masses in both breasts. She complained from severe pain and swelling of the breasts. Imaging workup showed bilateral breast lesions, and diagnosis of breast infiltration by leukemic cells was confirmed after immunohistopathological evaluation. The patient suffering from severe pain,discomfort, and swelling of both breasts due to leukemic infiltration was referred to the Radiation Oncology Department for symptomatic palliation. Whole breast irradiation was delivered to both breasts of the patient with BART using the ABC system. The patient had complete resolution of her symptoms after treatment with BART.CONCLUSION BART with the ABC system resulted in complete resolution of the patient’s symptoms due to leukemic infiltration of both breasts with T-ALL. This contemporary treatment technique should be preferred for radiotherapeutic management of patients with leukemic infiltration of the breasts to achieve effective symptomatic palliation.
Key words: T-cell acute lymphoblastic leukemia; Breast relapse; Breathing adapted radiation therapy; Active breathing control; Case report
INTRODUCTION
A considerable proportion of patients with leukemia suffer from relapse during the course of their disease, mostly in the bone marrow[1]. The central nervous system and testes are frequent locations and sanctuary sites for extramedullary relapses.Involvement of the breast by leukemia is uncommon but may manifest as an oncological emergency requiring prompt management[2-4]. Acute myeloid leukemia constitutes the most common type of acute leukemia in adults, and is also the most common type infiltrating the breasts. Isolated extramedullary relapse of T-cell acute lymphoblastic leukemia (T-ALL) within the breast is exceedingly rare and there is paucity of data in the literature regarding this entity[5-7]. No consensus exists on management of isolated extramedullary breast relapses of T-ALL. Herein, we report a case of isolated extramedullary breast relapse of T-ALL treated with breathing adapted radiation therapy (BART) using the active breathing control (ABC) system.
CASE PRESENTATION
Presenting symptoms and medical history
The patient was a 33-year-old female with diagnosis of T-ALL. Initial laboratory data showed increased leukocyte count of 105 × 109per liter (L), decreased hemoglobin level of 7.8 mg per deciliter (mg/dL), and decreased platelet count of 28 × 109/L. She received intensive systemic chemotherapy including L-asparaginase, prednisone,vincristine, and intrathecal methotrexate, hydrocortisone, and cytosine arabinoside,which resulted in complete remission of her disease, and then underwent allogeneic hematopoietic stem cell transplantation. After a 15 mo period without symptoms and signs of progression, the patient presented with palpable masses in both breasts. She complained from severe pain and swelling of the breasts.
Diagnostic workup
Polymerase chain reaction analysis of bone marrow aspirates demonstrated complete allogeneic hematopoietic chimerism, and there were no leukemic lesions at other sites including the bone marrow and cerebrospinal fluid. Imaging workup included bilateral mammography, doppler ultrasonography and breast magnetic resonance imaging (MRI). On ultrasonography, lesions were detected in the upper inner quadrant of the right breast with mixed echo and significant hyperechogenicity.Another lesion was detected in the left breast with mixed echo and significant hyperechogenicity. Doppler ultrasonographic assessment showed vascularization in these breast lesions. Diffusion-weighted and dynamic contrast-enhanced breast MRI revealed significant diffusion restriction and type 2 and 3 contrast patterns. Lesion on the right breast was heterogeneously hypointense with contrast enhancement. The lesion in the left breast also showed contrast enhancement, and was hypointense on T1 weighted sequencing, and hyperintense on fat suppressed MRI.
FINAL DIAGNOSIS
The patient was referred for biopsy, and diagnosis of breast infiltration by leukemic cells was confirmed after immunohistopathological evaluation. Immunohistopathological assessment revealed presence of small to medium size lymphoblastic cells with narrow cytoplasm and hyperchromatic nuclei. Atypical cells were positive for terminal deoxynucleotidyl transferase, cluster of differentiation 3(CD3), CD5, and CD34 on immunohistochemical analysis. Paired box gene 5 was weakly positive. Myeloperoxidase, CD10, CD117, and CD20 were negative. The Ki-67 proliferation index was 40%.
MULTIDISCIPLINARY EXPERT CONSULTATION
After multidisciplinary expert consultation, the patient suffering from severe pain,discomfort, and swelling of both breasts due to leukemic infiltration was referred to the Radiation Oncology Department for symptomatic palliation.
TREATMENT
Whole breast irradiation was delivered to both breasts of the patient with BART using the ABC system (Elekta, United Kingdom). Total radiation dose was 50 Gy delivered in 25 daily 2-Gy fractions over 5 wk. The patient was trained for compliance with the ABC system before computed tomography (CT) simulation as per our institutional protocol[8]. Reproducible moderate deep inspiration breath holding (mDIBH) by use of the ABC system has been achieved after the training session, and planning CT images were acquired at the CT-simulator (GE Lightspeed RT, GE Healthcare, Chalfont St.Giles, United Kingdom) at mDIBH. A breast board was used for reproducible positioning and immobilization of the patient at each treatment fraction. After acquisition of the planning CT images, three-dimensional image data sets were transferred to the contouring workstation via the network. Delineation of both breast target volumes and critical organs including the spinal cord, heart, and lungs was performed at the Advantage Sim MD simulation and localization software(Advantage SimMD, GE, United Kingdom). Structure sets including the contoured target volumes and critical organs were sent to the treatment planning workstation.Radiation treatment planning for whole breast irradiation of both breasts was performed by using PrecisePLAN treatment planning system (PrecisePLAN, Elekta,United Kingdom). BART was delivered at the linear accelerator (Synergy, Elekta,United Kingdom) under image guidance for setup verification using electronic portal imaging device (Iview, Elekta, United Kingdom) and kilo-voltage cone beam CT (Xray volumetric imaging, Elekta, United Kingdom).
OUTCOME AND FOLLOW-UP
Compliance of the patient with treatment procedure was excellent and there was no need for any treatment breaks. The patient had complete resolution of her symptoms after treatment with BART. The timeline of the disease course is shown in Table 1.Axial CT images of the patient before and after treatment with BART are shown in Figures 1 and 2, respectively.
DISCUSSION
Literature review
There is paucity of data regarding extramedullary relapse of ALL in the breast.Although rare, extramedullary relapse should be vigilantly considered in differential diagnosis of a breast lump when a history of leukemia is present[9,10].
As a local treatment modality, radiation therapy has been judiciously used for management of extramedullary leukemia relapse in sanctuary sites such as the CNSand testes[11-13]. Regarding isolated extramedullary relapses of ALL within the breast,there is no consensus on standard management. Nevertheless, complete resolution of breast lesions by use of irradiation has also been reported in other studies consistent with our findings[14-16]. Future trials are clearly needed to shed light on optimal management of isolated extramedullary relapses of ALL in the breast.

Table 1 Timeline of the disease course
Discussion
Extramedullary relapse of T-ALL in the breast is exceedingly rare. To the best of our knowledge, management of leukemic infiltration of both breasts by T-ALL by use of BART has not been previously addressed in the literature. BART has been the primary mode of radiotherapeutic management of breast cancer in our department given the reported dosimetric benefits and significantly improved normal tissue sparing with incorporation of breath holding at moderate deep inspiration during treatment simulation and delivery[8,17,18].
Briefly, mDIBH with the ABC system was developed for management of respiratory motion for thoracoabdominal tumors and has been used for this purpose in both conventionally fractionated radiotherapy regimens and Stereotactic Body Radiation Therapy applications[8,17-21]. In addition to respiratory motion management,an additional benefit of mDIBH with the ABC system for breast cancer includes minimizing exposure of the heart particularly for left-sided breast cancer patients along with improved sparing of other critical organs, which has been supported in previous studies[8,17,18].
Given the benefits of BART, this contemporary technique was adapted for management of our patient with bilateral breast lesions and led to complete resolution of her symptoms. Bilateral whole breast irradiation using BART for leukemic infiltration of both breasts with T-ALL has not been subject to any previous reports.However, there is no standard management in the setting of leukemic infiltration of both breasts with T-ALL, and treatment decisions regarding management of this exceedingly rare entity are individualized based on patient and tumor characteristics along with institutional experiences. Incorporation of contemporary techniques such as BART at mDIBH with the ABC system may offer improved radiotherapeutic management of these patients, particularly in the setting of bilateral breast irradiation.
CONCLUSION
BART with the ABC system resulted in complete resolution of the patient’s symptoms due to leukemic infiltration of both breasts with T-ALL. This contemporary treatment technique should be preferred for radiotherapeutic management of patients with leukemic infiltration of the breasts to achieve effective symptomatic palliation.
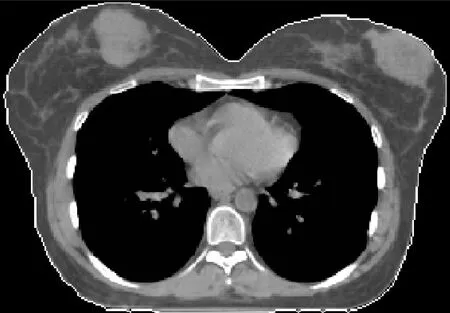
Figure 1 Axial computed tomography images of the patient showing bilateral breast lesions before breathing adapted radiation therapy.
