
Survival rate and the determinants of progression from HIV to AIDS and from AIDS to the death in Iran: 1987 to 2016
2019-02-27 05:24:58MohammadMirzaeiMaryamFarhadianJalalPoorolajalParvinAfsarKazerooniKatayounTayeriYounesMohammadi
Mohammad Mirzaei, Maryam Farhadian, Jalal Poorolajal, Parvin Afsar Kazerooni,Katayoun Tayeri, Younes Mohammadi
1Department of Epidemiology, School of Public Health, Hamadan University of Medical Sciences, Hamadan, Iran
2Research Center for Health Sciences, Department of Biostatistics, School of Public Health, Hamadan University of Medical Sciences, Hamadan, Iran
3Modeling of Noncommunicable Diseases Research Center, Department of Epidemiology, School of Public Health, Hamadan University of Medical Sciences,Hamadan, Iran
4HIV/AIDS Research Center, Shiraz University of Medical Sciences, Shiraz, Iran
5Iranian Research Center of HIV & AIDS, Tehran University of Medical Sciences, Tehran, Iran
6Social Determinants of Health Research Center , School of Public Health, Hamadan University of Medical Sciences, Hamadan, Iran
ABSTRACT Objective: To examine the prognostic factors of progression from HIV to AIDS and AIDS to the death in people living with HIV/AIDS in Iran. Methods: In this registry-based retrospective cohort study, we recruited 28 873 HIV-infected people from 158 Behavioral Diseases Counseling Centers of Iran. Two outcomes of interest included survival rates from HIV diagnosis to AIDS and from AIDS to the death. We used Kaplan-Meier and Cox regression model to investigate survival rate and factors affecting on survival controlling effect of confounding factors. Results: The one, three, five, and ten-year survival rate from HIV to AIDS were 85%, 73%, 61% and 32%, and for AIDS to death were 90%, 81%, 74% and 55%, respectively. Multivariate Cox regression analysis indicated that the risk of progression from AIDS phase toward death in individuals with CD4 less than 200/mm3, infected with tuberculosis (TB) and not treated by antiretroviral therapy (ART) was 2.17 (95% CI: 1.62-2.90), 1.49 (95% CI: 1.01-2.20) and 4.88 (95% CI: 3.42-6.96) times higher respectively. The risk of progression to AIDS in patients with baseline CD4 less than 200/mm3 was 2.32 (95%CI: 2.14, 2.51) times higher than patients with CD4 > 200/mm3 (P=0.001). On the other hand, tuberculosis increases the risk of death by 49.0% (P=0.04). The hazard ratio of death in patients who did not receive ART was 4.88 (95% CI: 3.42, 6.96) times higher than patients who received ART (P<0.001). Conclusion: The early detection of HIV, the screening and treatment of TB and receiving the ART improve the survival of HIV/AIDS patients significantly, and prevent the transmission of HIV to other people.
Keywords:HIV/AIDS Prognostic factor Survival time Tuberculosis Cohort study
1. Introduction
Human immunodeficiency virus (HIV) and acquired immunodeficiency syndrome (AIDS) is a major public health concern[1]. HIV attacks the immune system, especially cluster of differentiation4 (CD4) cells (T cells), and leads to progression to AIDS. The progression of the disease can destroy some organs of the human body, and finally leads to the patient’s death. AIDS is the final stage of HIV infection that immune system is seriously destroyed. In the presence of HIV, CD4 cells reduce and the patient will be susceptible to opportunistic infections[2,3].
Highly active antiretroviral therapy or short form antiretroviral therapy (ART), which has been established since 1997, is the combination of several antiretroviral treatments which are used to suppress HIV viral replication[2]. The statistics indicate that, by the end of 2016, the new cases of HIV, and death cases for each years is approximately two million and over one million people respectively,and for now, about 37 million people were live with HIV (PLHIV)worldwide[3, 4]. To date, although there is no radical treatment for HIV/AIDS, ART can effectively improve the quality of life, survival rate and life expectancy of the patients and prevent the transmission of HIV[5-7]. Despite the widespread use of ART and reduction of the incidence and mortality rate globally, this reduction is not uniform for all countries. The statistics showed the global coverage of ART in the patients is 53.0%, that was, about half of the patients do not receive the treatment at all[4,7].
The available studies have explored the role of the prognostic factors in the progression of HIV/AIDS. They revealed that the early detection of HIV along with the early initiation of ART can decelerate progression toward both AIDS stage and death in the patients[8,9]. Moreover, these studies indicated that delay in the detection of HIV negatively associated with the survival of the patients[10,11]. Furthermore, it has been documented that risk of getting tuberculosis (TB) infection and risk of dying from TB in individuals with HIV/AIDS is 20 times and three times of that in individuals without TB, respectively[12]. In general, the early detection of the disease, the early treatment with ART and the complete adherence to ART, CD4 cell count at the time of diagnosis,the treatment of TB and other infections such as hepatitis C virus have been considered as the most important determinants of survival rate and life expectancy of HIV/AIDS patients[13,14]. However, due to the small sample size and the different statistical methods, the results are contradicted.
Despite reduction in the new cases of HIV infections by 36.0%and mortality from AIDS by 38.0% worldwide, it still has been left as a major health problem[7], therefore, examining factors contribute in survival of the patients is crucial.
In Iran, the available evidence suggested that the factors such as ART, TB were associated with the survival of patients[9,10]. However,due to the small samples and being unrepresentativeness of the samples, our information on the survival rate of the PLHIV and the related prognostic factors is limited. Therefore, the aim of this study was to investigate survival rate and the determinants of progression from HIV to AIDS and from AIDS to death in Iran.
2. Material and methods
2.1. Study design and data sources
In this registry-based retrospective cohort study, we recruited 28 873 HIV positive patients from 158 Behavioral Diseases Counseling Centers (BDCC) from 31 provinces of Iran during 1987 to 2016.These centers established in 2000 and then were expanded to the medical universities and prisons nationwide. However, before the establishment of BDCC and during 1987 to 1999, the cases of HIV/AIDS were reported and registered by the sentinel sites located in prisons and blood transfusion organization and then, the patient was referred to health centers to receive the health services.
The process of data collection and preparation by BDCC were as follows: When the patient was identified by hospitals, prisons,sentinel site, Blood Transfusion Organization, harm reduction centers; he/she was referred to BDCC to receive health and medical care services. In BDCC, all patients receive a private code by which he/she can use the required health service across the country. In BDCC, patient information was collected and sent to Iranian Centers for Disease Control and Prevention (CDC). Then, the data were checked by experts of CDC, and the data would be sent back to BDCC for corrections if it is wrong.
The required services for HIV/AIDS patients in BDCC include health education, pre-test and post-test consultation, implantation of the harm reduction program, supplying ART, the prevention of mother to child transmission, pre-exposure and post-exposure prophylaxis and the treatment of the sexually transmitted infection.
2.2. Inclusion/exclusion criteria
In this study, inclusion criteria was the patients who were positive for anti-HIV antibody by ELISA tests and confirmed by western blot test and were followed-up. On the other hand, we excluded the patients without the date of diagnosis or follow-up period[10].Regarding to our eligibility criteria, 28 873 patients were included in this study.
2.3. Data collection tool
We used the data registered by Iranian BDCC. These centers used a checklist to collect data. The checklist included the demographic and clinical questions such as age at the diagnosis time, gender,the date of HIV diagnosis, the mode of HIV transmission [(unsafe sexual contact, injecting drug users, mother to child and unknown)],HIV status, the date of entrance to AIDS stage, the clinical stage of HIV/AIDS at diagnosis time (stage ⅠⅡⅢ and Ⅳaccording to the WHO categorization), receiving or not receiving ART, the first date of receiving ART, CD4 cells count at the time of HIV diagnosis, the level of education and marital status.
In this study, we just considered the baseline examinations of the patients in model. Variables such as age, marriage status, the mode of transmission were analyzed in the categorical form. On the other hand, CD4 and ART were considered as dichotomous variables.
2.4. Outcome
In this study, two outcomes of interest were time from HIV diagnosis to AIDS phase and time from AIDS phase to the death.The patients who were lost to follow up or died from other causes were considered censored.
2.5. Statistical analysis
To estimate the survival time, we constructed life table and plotted it by the Kaplan-Meier method. To calculate survival probability in life table method; first, probability of death was obtained as the number of event (deaths or AIDS) divided by the number of people who lived at the beginning of each period minus half of the censored or lost to follow-up people. Finally, probability of death was subtracted from 1 to calculate survival probability.To investigate the association of the prognostic factors include age,gender, mode of HIV transmission, marital statu, education, TB,ART treatment and CD4 cell counts at diagnosis with survival time and progression of the disease, Cox proportion hazard model was used. Moreover, Schoenfeld’s residual test was used to investigate the proportional hazards (PH) assumption of the model.
P-value less than 0.05 were statistically significant. We used the statistical software, Stata version 12 (Stata Corp, college station,Texas, USA) for analysis of data.

2.6. The ethical consideration
In this retrospective cohort study from 1987 to 2016, we used the data registered by BDCC. This study is a part of thesis project in master of epidemiology (No. 9508044500). The study has been approved by the Ethics Committee of Hamadan University of Medical Sciences (No. P/16/35/10/198, 25 October 2016).
3. Results
3.1. The demographic and clinical characteristics
From 1987 to December 2016, data for 28 873 HIV-positive patients were extracted from 158 BDCC from 31 provinces of Iran.Out of 28 873 patients, 24 253 (84.0%) were males, 24 908 (86.3%)were 25-44 years old, and the mean age of subjects was (34.0±10.0)years. The mean age for women and men was (32.0±11.0) and(34.0±9.0) years old, respectively. Moreover, 9 817 (34.0%) were married and 19 345 (67.0%) of them injecting drugs which was the most commonly recorded route of transmission. Examining the patients showed that 1 117 (3.9%) of them infected with TB. In terms of CD4 test, 12 993 (45.0%) of patients had CD4 test. More than one third of the patients were in AIDS stage. The total number of the patients who received ART was 9 817 (34.0%).
3.2. Survival time
Figure 1 demonstrates the survival rate from HIV to AIDS stage and from AIDS stage to the death for both sexes using Kaplan-Meier method. As shown in the figure, survival rate for woman was higher than that for men.

Table 1 The survival time of progression from HIV-positive to AIDS and from AIDS to death in Iran from 1987 to 2016 by using life table.
The life table for survival rate from HIV to AIDS stage, and from AIDS stage to the death and from HIV-infection to the death was presented in Table 1. The total duration of follow-up for the included patients was 100 411 person-years with a median followup of (3.4±3.8) years. The one-year, three-year, five-year and ten-year progression rate from HIV to AIDS was 85% (1-3 466/23 699), 73%[(1-867/11 351)×79%], 61% [(1-674/7 440)×67%], 32% [(1-217/1 728)×36%], respectively.
In the same way, the one-year, three-year, five-year, and ten-year survival rate from AIDS stage to the death was 90% (1-832/8 195),81%[(1-212/4 028)×85%], 74% [(1-73/1 719)×77%] and 55%[(1-14/157)×60%], respectively.
Moreover, the one-year, three-year, five-year and ten-year survival rate from HIV to the death was 90.0%(1-(2 568 / 24 507), 78.0%[1-(844/13 955)×83%], 68.0%[1-(627/9 780)×73%] and 48.0% [1-(238/2 872)×52%], respectively.
3.3. The prognostic factors
The hazard ratio (HR) of the association between the prognostic factors and progression from HIV to AIDS and AIDS to the death is presented in Table 2 and Table 3 respectively. As shown in Table 2, there was a significant difference in the risk of progression to AIDS between age groups (P=0.001). The risk of progression to AIDS in the married patients was 21.0% higher than single patients (P<0.001). Moreover,compared with injecting drug users, the risk of progression in patients with the unsafe sexual contact was 39.0% higher (P=0.001).Individuals with CD4 less than 200/mm3were 2.32 (95%CI: 2.14,2.51) times more likely to progress to AIDS than individuals with CD4 more than 200/mm3(P=0.001).
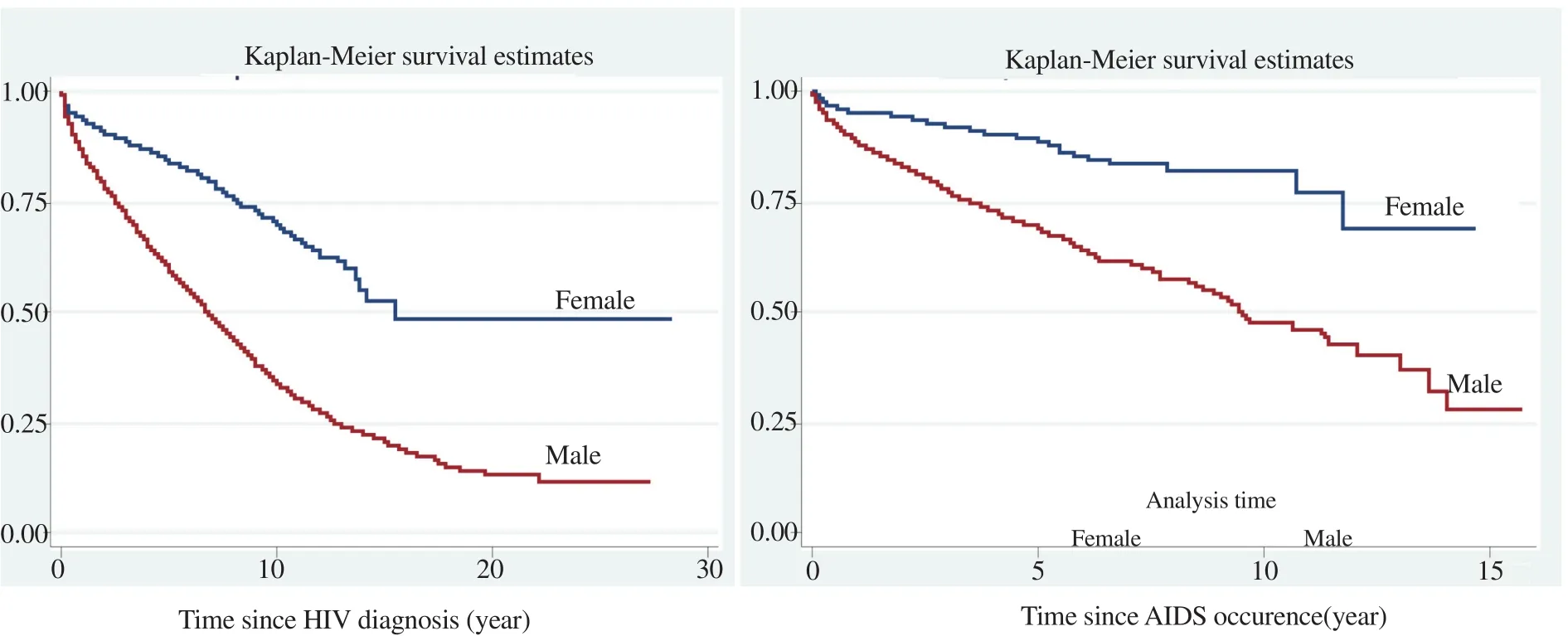
Figure 1. Survival time of HIV/AID patients in Iran between 1987 to 2016 by gender.
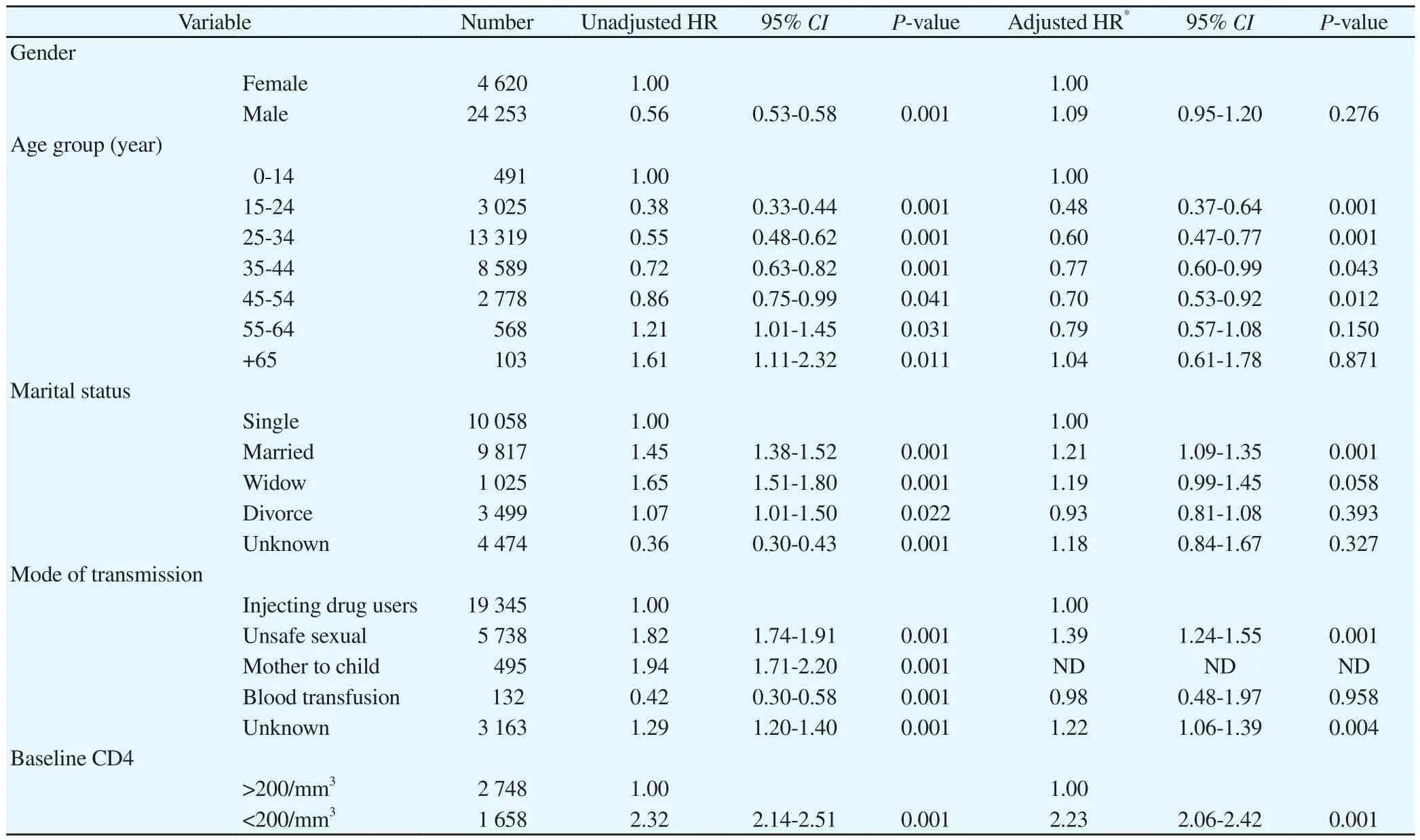
Table 2 Effect of prognostic factors on survival time of progression from HIV-infection to AIDS stage using Cox regression model in Iran from 1987-2016.
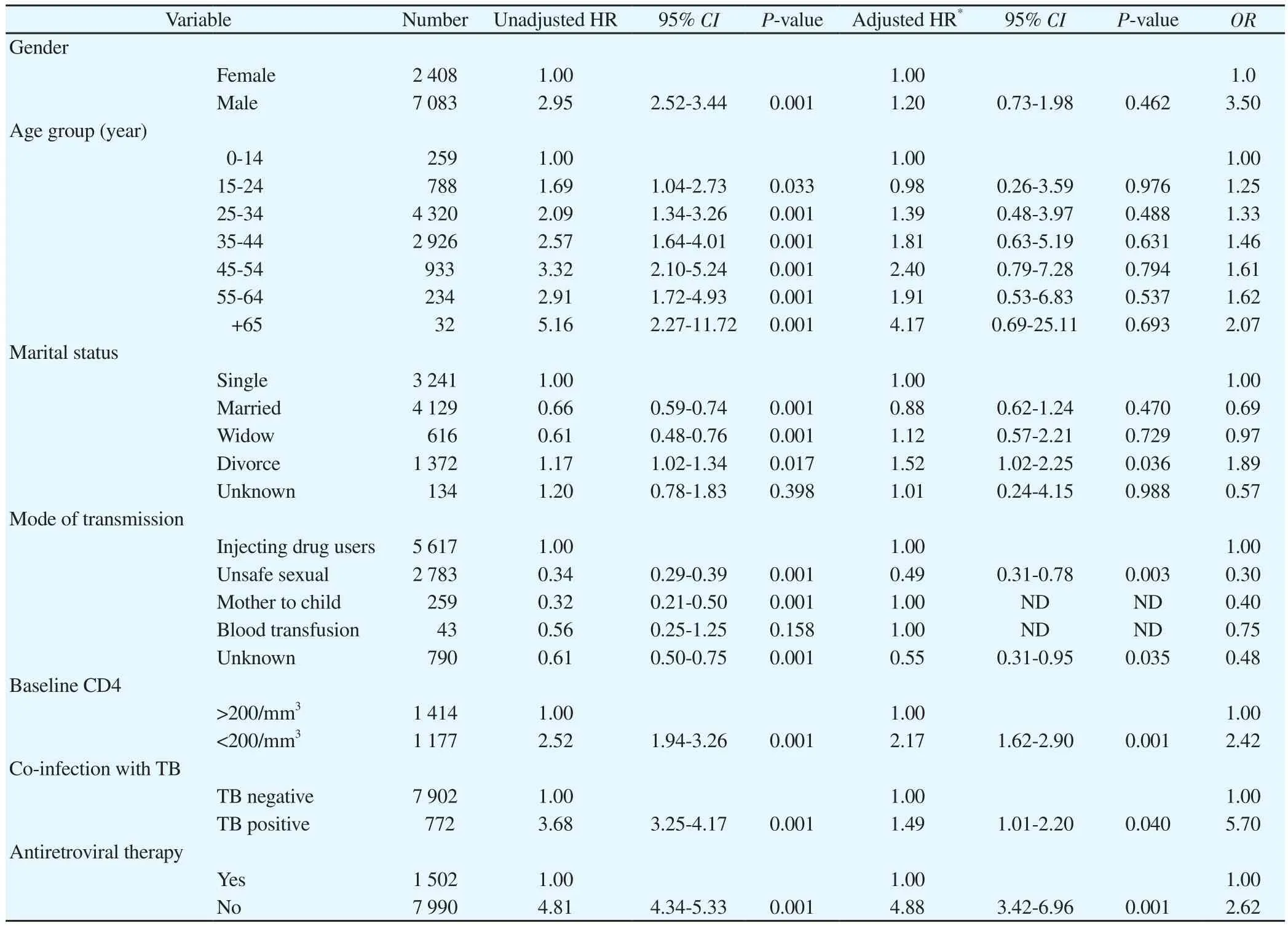
Table 3 Effect of prognostic factors on survival time of progression from AIDS stage to death using Cox regression model in Iran from 1987-2016.
Regarding to Table 3, in the adjusted method, there was no significant difference in progression of AIDS to death between men and women and between age groups (P>0.05). Compared to single patients, the divorced patients had 52.0% higher risk for progression from AIDS to death (P=0.036). The risk of progression from AIDS to death in patients with the unsafe sexual contact was significantly lower than the injecting drug users (HR= 0.49, 95%CI: 0.31, 0.78).Moreover, the risk of progression from AIDS to the death in patients with CD4 cell count less than 200/mm3was 2.17 (95%CI: 1.62,2.90) times of that in the patients with CD4 cell count over 200/mm3(P=0.001). Compared with the patients without TB, the patients with TB had 49.0% the higher risk for progression to death (P=0.04).
The results of both adjusted and unadjusted model indicated that ART is the most important prognostic factor associated with progression of HIV/AIDS disease. The risk of death in patients who did not receive ART was 4.88 (95%CI: 3.42, 6.96) times higher than patients who received ART (P=0.001). In addition to HR, the results are presented as odds ratio. Accordingly, the odds of death in patient with TB are 5.70 times of that in patients without TB. Moreover,odds of death in men are 3.50 times of that in women. On the other hand, odds of dying in patients who don’t receive ART was 2.62 times of patients who received ART, and finally, odds of death for patients who had baseline CD4 less than 200/mm3was 2.42 times of that in patients who had baseline CD4 more than 200/mm3.
4. Discussion
Today, throughout the country, the establishment of BDCC with the skilled personnel and physician provide the educational, counseling and health care services with antiretroviral therapy for all patients freely.
Identifying the prognostic factors contribute in the survival of HIV positive patients, especially in developing countries, is essential to design the effective interventions to increase the life expectancy of the patients. In this study, we aimed to identify these effective factors in Iran.
Our findings showed that the majority of HIV positive individuals were male, aged 25-44 year, and injecting drug was the most common route of transmission. The survival of HIV/AIDS patients reduced in the long run, so that it began about 90.0% in the first year, and then it reached to less than 50.0% in the tenth year. Being married, CD4 less than 200/mm3were the major prognostic factor for progression to AIDS. On the other hand, being divorced, CD4 less than 200/mm3, infection with TB and not receiving ART were the major prognostic factor for progression from AIDS to the death.Examining the literature indicates that our finding is in concordance with other studies. Liuet al.in china reported that the one-year,three-years, five-years, ten-year and eleven-year cumulative survival rate was 91%, 88%, 86.0%, 79.0% and 79.0%, respectively, and ART and low CD4 count at diagnosis time were presented as the significant factors[8]. Furthermore, in one more study published in 2012, the 10-year survival of HIV infected patients was 45.0%[15].However, the survival rates of our study were lower than mentioned studies. The differences may arise from difference in coverage of ART, prevalence of TB and access to medical services between populations.
Based on our findings, the majority of the HIV positive patients were male and injecting drug users. Due to cultural circumstance,men who have sex with men or with women usually deny the sexual relations, and therefore, this issue results in the increased reported statistics of HIV/AIDS through injecting drug. However,in the recent years, especially after 2012, change in pattern of HIV transmission from injecting drug to the unsafe sexual contact result in the increased number of HIV-positive cases among women. This finding is an alarm for Iranian health system, that if no immediate action plan is taken, under these circumstances, the disease will be expanded to general population rapidly, and therefore, it will be more difficult to control.
In our study, TB was one of the most important prognostic factors in the progression from HIV to death and patients who infected with TB had the higher risk of progression to the death than patients without TB. This finding is in consistence with other studies[13,14].Lopez-Gatelet al.showed that risk of AIDS-related death in the patients with TB was 2.4 times of that in patients without TB[16].Moreover, Whalenet al.in Uganda found that development of TB in the early stages of HIV infection may seriously decline the survival of the patients[13]. According to the report of the World health organization, the risk of developing TB in PLHIV is 17-22 times of that in people without HIV[12]. In our study, the cumulative prevalence rate of TB was 3.9% which positively associated with progression of the disease. Therefore, the detection and treatment of TB to increase longevity of the patients is so crucial.
Our study found that individuals who did not receive ART had about five times risk of the death compared to the patients who received ART. Currently, with help of ART, AIDS has been changed to a chronic and controllable disease which needs lifetime care; despite in the early 1980s, HIV/AIDS was a highly fatal disease[17] ART strengths the immune system, improves the quality of life, extends life expectancy, and plays a highly effective and protective role for progression from HIV to AIDS and from AIDS to the death[9,11,18]. ART not only increases the quality of life and survival, but it can prevent transmission of HIV to others through sexual contact, mother to child and injection of drug[7]. Seyoumet al.reported that the risk of AIDS-related death was 4.2 times greater for patients had the low adherence to ART treatment[19]. In 2016, Poorolajalet al.reported that the longevity of the patients who receive ART is 10 years longer than the patients who did not receive ART, so that the majority of patients without ART die within two years from the onset of AIDS[9], Teeraananchaiet al.in a meta-analysis found that after starting ART, life expectancy for men and women infected with HIV increase by 23 and 33 years respectively[18]. In this study, we found that mean survival time for patients who received ART was 13 years and for the patients who did not receive ART was 3 years from onset of AIDS. This indicates that receiving ART will add at least 10 years to the longevity of AIDS patients. Therefore, we suggest that community health workers must timely detect HIV-positive patient and start ART as soon as possible for all PLHIV (test and treat strategy).
There are several limitations in this study. First, to estimate the patients’ survival rate exactly, a prospective cohort study with a reliable and high-quality data is needed, while we used retrospective cohort with data that registered and collected by Ministry of Health and Medical Education, and therefore, quality of the registered data may be questionable[20]. Second, one of the limitations in survival studies is censoring. In this study, we encountered with left censoring issue. In the other word, we do not know the exact date of HIV onset,while we used the date of HIV diagnosis as HIV onset, and therefore this issue may lead to the underestimation of the actual survival from HIV to AIDS stage. Third, to estimate the exact time of AIDS stage,we needed continuous follow-up, while some of the patients were not visited regularly, and therefore, information on some patients was not available, which this issue may lead to overestimation of the actual survival time.
This study was conducted at the national level (big sample size) and therefore, this study can portrays a comprehensive picture of HIV/AIDS status in Iran. Furthermore, this large sample size has two major advantages: the high statistical power with more reliability and validity and the generalizability of the results to Iranian HIV/AIDS population. Finally, using the advanced statistical methods,we controlled the effect of the confounding factors to investigate the relatively pure effect of each factor.
The results of this study showed that several modifiable and nonmodifiable factors contribute in the progression toward AIDS and death. ART, TB and CD4 are the most important prognostic factors of AIDS-death related. Therefore, the early detection of HIV, the treatment of TB and the timely initiation of ART for all patients may improves the survival of the patients and prevent the transmission of HIV to other.
Conflict of interest statement
The authors declare they have no conflict of interest.
Acknowledgements
We would like to appreciate the head and personnels of HIV/AIDS office of Center for Diseases Control and also staff and physicians of behavioral diseases counseling centers throught Islamic Republic of Iran for their services and technical assistance.
Fundation project
The study was funded by the Vice-chancellor for Research and Technology, Hamadan University of Medical Sciences (No.9508044500).
 Asian Pacific Journal of Tropical Medicine2019年2期
Asian Pacific Journal of Tropical Medicine2019年2期
- Asian Pacific Journal of Tropical Medicine的其它文章
- Observational study to assess pregnant women's knowledge and behaviour related to toxoplasmosis in Essaouira province, Morocco
- Insecticide susceptibility status and resistance mechanism of Anopheles cracens Sallum and Peyton and Anopheles maculatus Theobald (Family:Culicidae) from knowlesi malaria endemic areas in Peninsular Malaysia
- Occurrence of Chlamydia spp. in wild birds in Thailand
- Modeling and predicting dengue fever cases in key regions of the Philippines using remote sensing data
- Epidemiological, prevention and control updates of yellow fever outbreak in Brazil