
Theoretical knowledge and psychomotor skill acquisition of basic life support training programme among secondary school students
2019-02-23 02:02:14IsraelOlatunjiGabrielJoelAluko
Israel Olatunji Gabriel, Joel O. Aluko
1 School of Post Basic Nursing Programmes (Anaesthesia), Ahmadu Bello University Teaching Hospital, Zaria, Kaduna State, Nigeria
2 The Department of Nursing, University of Ilorin, Kwara state, Nigeria
KEY WORDS: Cardiopulmonary resuscitation; Basic life support; Education; School students; Lifesaving skills; Nigeria
INTRODUCTION
A compelling challenge facing modern medicine is increased in cardiovascular diseases. According to World Health Organization,[1]among 56.4 million global deaths in 2015, 39.5 million or 70% were due to noncommunicable diseases (NCDs), and 17.7 million people(45% of all NCDs deaths) died from cardiovascular diseases, mainly because of sudden cardiac arrest(SCA).[2]The prevalence of this disease has been and is expected to continue increasing.[3]Despite the technological advancement in the treatment and other advances in prevention, SCA remains a substantial issue in public health and a leading cause of death globally.[4,5]SCA affects about 350,000 to 700,000 people in Europe annually, and the number is expected to rise to more than 23.6 million by 2030.[6]In the United State of America(USA), incidence of SCA was 356,461 individuals between June 1, 2014, and May 31, 2015. In 2016, more than 350,000 individuals were affected, 46.1% of cases were witnessed by a bystander and the survivor rate was 12%.[7]SCA is a medical emergency that, if not treated without delay, it causes sudden death.[8]However, with fast and appropriate medical care like high quality chest compression and defibrillation, survival is possible.[9]The medical science opined that the first 4-8 minutes in sudden collapse is the most crucial period in which resuscitation intervention is most needed in saving victims life.[10]
It is estimated that a majority of SCA occurs outside hospital, and 85% of cases have a witness who were unable to do much.[11]Out-of-hospital cardiac arrest (OHCA) is serious public health concern because though the process is potentially reversible, the probability of recovery is small.The survivor rate in the USA varies between 9% and 12%,and this statistic has remained unchanged for about three decades in the USA. For instance, survivor rate for the year 2012, 2013, 2014, 2015, and 2016 were 11.4%, 9.5%,10.4%, 10.6%, and 12% respectively.[12]However, reliable statistics are lacking in most developing countries. Early CPR has a pivotal role in management of OHCA, every minute lost in initiating BLS leads to 10% decrease in survival rates of the victim.[13]
BLS is an evolving life-saving technique of modern medicine that comprises a series of life-saving actions that is useful in cardiac arrest.[10]It consists of chest compression and rescue breaths which re-establish oxygenated blood flow to the vital organs of an individual who has suffered cardiac arrest.[10]BLS can be administered by a trained person before the arrival of emergency medical services, this skill must be acquired by all adults, since many sudden cardiac arrest occurred outside the hospital setting.[14]The most important actions that have been proven to significantly reduce mortality rates is considered to be the more basic actions of BLS, known as high quality chest compression.[15]Other actions within the CPR realm, such as advanced life support (ALS) (administering medications,ventilation, intubation, intravenous fluids etc.), have also shown to have a significant effect on reducing mortality rates in SCA if BLS is initiated early. This places greater emphasis on the need to optimise the actions that are considered to be basic and more easily attainable by a greater number of the youth. Thus BLS is considered to be the foundation to save lives following SCA.[15]
African countries have in the past focused public health efforts on infectious/communicable diseases, but NCDs such as cardiovascular disease is on the rise in this continent.[16]The World Health Organization,[17]reported that NCDs are becoming a significant cause of morbidity and mortality in African countries, and that about 50%of this burden is attributable to cardiovascular disease.Unlike advanced countries, the incidence rates and survival from OHCA in Africa remain undefined despite carrying over 80% of the cardiac disease’s burden.[18]Waiting for health personnel who is trained in BLS in victims of SCA would mean brain damage and death.[19]Therefore, this placed an emphasis on the need to train non-medical persons on the administration of BLS most especially in the schools where all kinds of activities take place.[20]Non-medical personnel training can include all adults from age 15 and above.
BLS programme in schools has been receiving increasing global attention because of its great potential in increasing the number of potential bystander BLS providers not only in schools’ environments but ultimately in the larger communities. Although the OHCA incidence at schools is low, it accounts for only 2.6% of all public location. About one third of OHCA occurred during sports activity or at the sports facility;a trained student could witness the medical emergency that requires BLS in this location. A bystander who administers BLS to an OHCA victim can increase survival chances by 2-3 times. And since nearly 88%of the SCA occurs at home, there is a good chance bystander BLS would play an effective role in saving the SCA victim through the golden hour.[21]The teaching of BLS among secondary school students is encouraged globally, and many developed countries of the world have complied. In fact, few countries give lifesaving training for children as young as eight. However, the case is different in Nigeria where most adult and school children don’t have the knowledge and practice of BLS.[22]More so, there is paucity of publication on the knowledge and psychomotor skill of BLS among secondary school students in Nigeria.
The aim of this study was to evaluate the theoretical knowledge and psychomotor skill acquisition of BLS by a group of secondary school students in Nigeria before and after exposing them to BLS training. The study objectives were to: (1) assess the level of theoretical knowledge and psychomotor skill prior to BLS training; (2) assess the level of theoretical knowledge and psychomotor skill post BLS training; (3) compare the knowledge and psychomotor skill before and after BLS training.
METHODS
The study was conducted in the school auditorium.A quasi-experimental design was utilised with 210 participants. Data were collected across two time periods:at baseline (pre-training), and four-day from baseline(post-training).
Participants
Participants were the students of Demonstration Secondary School, Ahmadu Bello University, Kongo Annex, Zaria, Nigeria. The inclusion criteria were:students between age 14 and 19, literate with a minimum of ninth grade education (junior secondary school level). The exclusion criteria were: the teachers, as their knowledge and information could influence their participation, and anyone who previously had the training of BLS.
Intervention programme
The intervention was adapted with permission from the AHA. The intervention programme comprised threesessions of face-to-face training; two sessions on the first day and the third session on the second day, delivered by the researcher and research assistants (registered nurse anaesthetists who are certified BLS instructors). The first two sessions were 2 hours each in length; 90 minutes presentation of content relating to the session theme followed by questions and discussions. The third session was practicum for demonstrated of the psychomotor skill on a Resusci-Anne manikin (Table 1).
Data collection instruments
Two data collection instruments were utilised. To assess knowledge of the participants, the AHA BLS questionnaire was used. This is a 20-item multiple choice questionnaire related to cognitive knowledge of the participants. The detail distribution of the items was in the areas of: understanding of BLS, chest compression,opening of airway, compression ventilation ratio, adult BLS sequence, and AED. AHA observational checklist was utilised to assess psychomotor skill.[23]See Table 2.
Data collection
The study was conducted from 31stMay to 7thJune, 2018. Following ethics approval from the Institutional Review Board, the Principal of the school was approached; information about the study was explained to her in order for her to serve as mediator between the researcher and the students. Teachers were requested to give the information sheet to potential participants identified by them. A total of 428 students were approached within 2 days (from 31stMay to 1stJune, 2018). Of these, 420 agreed to participate in the study. Those who showed interest in participating in the study were asked to provide their names. Each student was given number sequentially (1-420). Those witheven numbers were recruited for the training (n=210),and those with odd numbers were discharged; not being part of the study. Data were collected prior to the commencement of the training (baseline), and at four-day from baseline (at completion of the training programme).
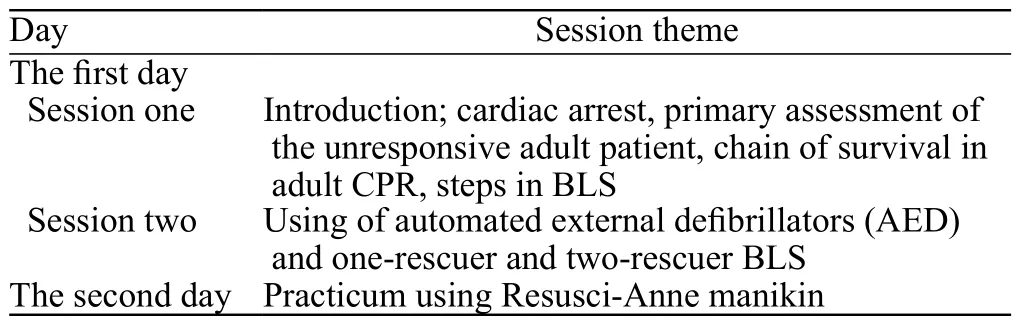
Table 1. Themes of the two-day training programme
Data analysis
Data were analysed using SPSS statistics version 20.Descriptive statistics and t-test were used to analyse the data. The demographic data analysed using frequency and percentage. Paired sample t-test was used to assess the knowledge and psychomotor skill and also compare the variables at baseline and post- training.
Ethical considerations
The study complied to the principles for human ethical research in the Declaration of Helsinki.[24]Ethical approval was obtained from the Institutional Review Board (ABU/DS/EC/012/2018).
RESULTS
Participant characteristics
The average age of 210 students who participated in the study was 17 years ± 1.5 standard deviation;their ages ranged between 14 and 19 years. None of the students received training in CPR before the study.Sixty percent of the participants were male, while 64.3%of them were within ages 14-15 years. Among the participants, 71.9% weighed between 30 and 49 kg, and 46.2% were Hausa by tribe. Of all participants, 46.2%were in senior secondary class 1 (SS1) (Table 2).
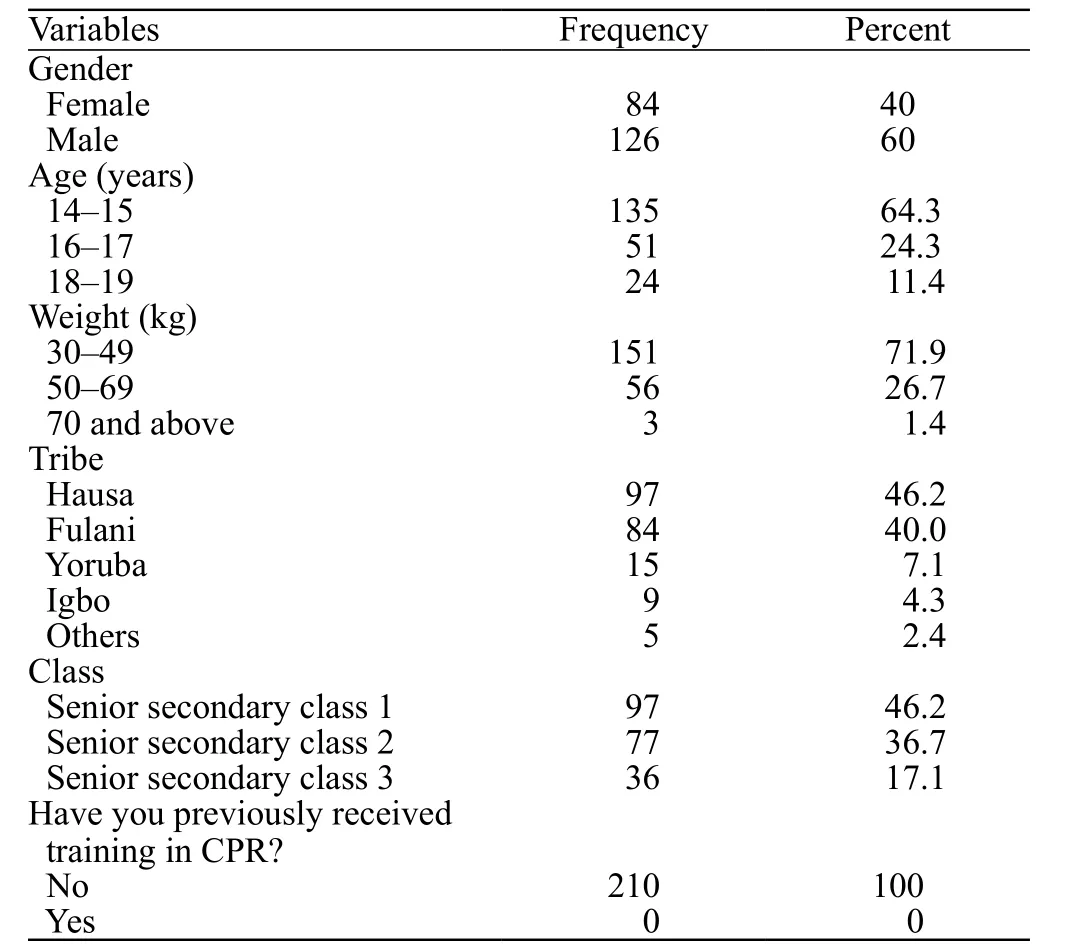
Table 2. Socio-demographic distribution of the participants (n=210)
Theoretical knowledge before and after intervention
Pre and post training results showed a significant increase in the percentage of correct answers in the post intervention data. The question about the first critical action the rescuer should perform on this patient once it is determined that the patient is in cardiac arrest was answered correctly by 5.7% of participants before the intervention, by 41.4% after intervention. The question about the recommended rate for performing chest compressions for victims of all ages was answered correctly by 10.5% of the participants at baseline, and 43.8% participants after intervention. The number of participants who knew the correct compression depth for adults was 16 (7.6%) before the intervention, 150(71.4%) after the intervention (Table 3).
Psychomotor skill before and after intervention
In Table 4, we can see that the participants’ skill on BLS is zero to nothing; they demonstrated poor psychomotor skill on the subject matter. None of the participants could score even a point. For example,0% was recorded on the assessment and activation and application of AED. However, the correct BLS application steps increased after the BLS applied training. Among the participants, 78.6% checked responsiveness, 62.9% of the participants shout for help/sent someone to phone and get an AED and 69.5% of the students checked breathing. While 70.5% of the students performed the step of applying the appropriate pressure for the chest compression correctly (high-quality compressions) in cycle 1 of CPR, only 53.3% of the students performed it correctly in cycle 2 of CPR, and cycle 3 of CPR recorded 74.8% performance.
Comparison of the participants’ baseline and post training knowledge and psychomotor skill
The mean knowledge score of the participants before the BLS training was 1.9. This score increased after the training to 11.4. The knowledge score changed significantly over time (P<0.000). In the advanced analysis which was conducted in order to determine the source of the change, it was determined that the knowledge scores in the post test were significantlyhigher than the baseline.
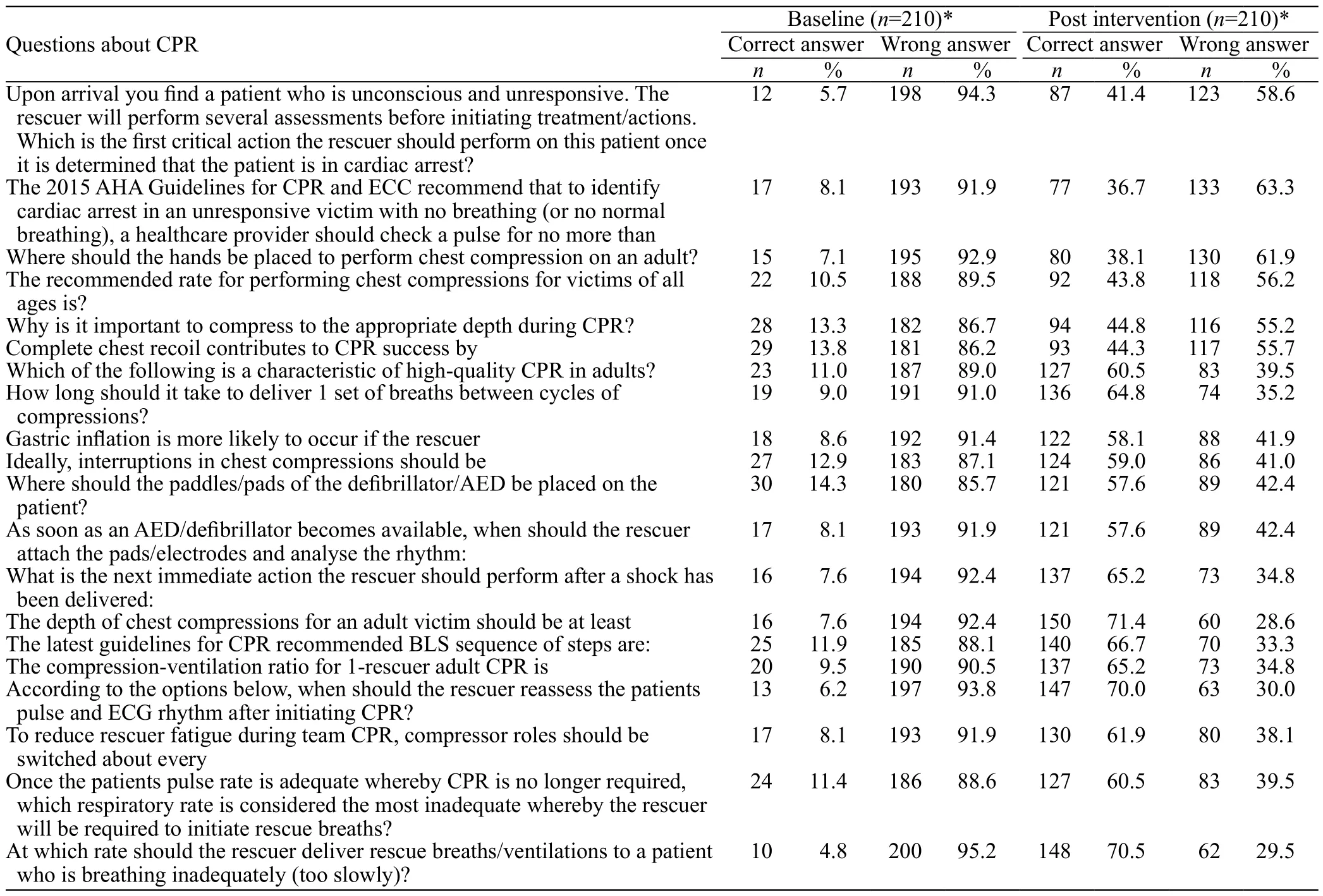
Table 3. Distribution of the answers provided regarding the knowledge of BLS at baseline and post-intervention
The mean psychomotor skill score of the participants was 0.0 before the training and 8.9 after the training. The skill score changed significantly over time (P<0.000).The average skill score was significantly higher in the post training than the baseline (Table 5).
DISCUSSION
The main findings from this study were that most of the students lacked knowledge regarding BLS before training, and were found to have no skills exposure whatsoever concerning BLS at baseline, but after the training, they performed reasonably well in the “handson skills”. Looking at the results of this study, it can be seen that the number of students who correctly answered the question about the depth of chest compressions for an adult’s victim was not very high before the BLS training (7.6%), there was increase in the percentage of correct answers after training (71.4%). Among the participants, 10.5% got the question on the recommended rate for performing chest compressions for SCA victim at baseline, but post-training result was 43.8%. This result is similar to those of Rajeswaran & Ehlers,[25]who reported improved BLS knowledge after training, but deteriorated over the three months.
Students’ BLS skills were poor at baseline, as no one got a mark (Table 5); they demonstrated poor psychomotor skill. However, there was a great demonstration of skills on the Resusci-Anne skillmeter manikin after the training. Of the participants,78.6% checked responsiveness, 62.9% shout for help/sent someone to phone and get an AED, 69.5% checked breathing, and 70.5% of the participants performed the step of applying the appropriate pressure for the chest compression correctly (high-quality compressions) in cycle 1 of BLS. This is consistent with findings reported in Bahrain and Ireland.[26,27]The skills which no students performed correctly in this study included checking responsiveness, checking breathing, performing highquality compressions, placement of the hand during BLS,the required number of compressions per minute, and the correct rate of compressions.
Also, it is interesting to note that more male participants were involved in this study (60%) compared to similar study[28]in Port Harcourt, Nigeria with more female participants (62.67%). This could be due to religious differences between Zaria in North-west Nigeria having mainly Muslims, and River state in South-south Nigeria having mainly Christians.
Although the participants showed very poor pretraining BLS knowledge, their post-training BLS results improved very significantly. It should be noted that none of the participants had any previous BLS training before this study. The finding is in accordance with that of Dal & Sarpkaya;[8]the study reported that CPR knowledge score of the students after training was increased and significantly difference. However,this could not be sustained till 6 months. According to Adedamola Onyeaso & Onyeaso,[29]participants reported poor CPR knowledge at baseline, but there was statistically significant improvement after the training. Similarly, Sankar, Vijayakanthi, Sankar, &Dubey,[30]conducted a prospective longitudinal study among qualified and undergraduate nurses; the former reported insignificant higher mean knowledge scores while the latter had significantly higher skill scores,however, both groups had improved scores after training. Thus, knowledge and skills of qualified and undergraduate nurses in CPR significantly improved with training. In a related study conducted by Onyeaso& Onyeaso,[31]involving student and teachers, gave 26.7% baseline BLS knowledge which later improved significantly to 100% after the training. However, the participants in this current study had poor pre-training BLS knowledge than the student teachers. This is understandable because the participants in the present study are very ignorant secondary school students who have not acquired any knowledge on critical care/ first aids as mentioned earlier compared to the students teachers who would have acquired some knowledge on first aids.
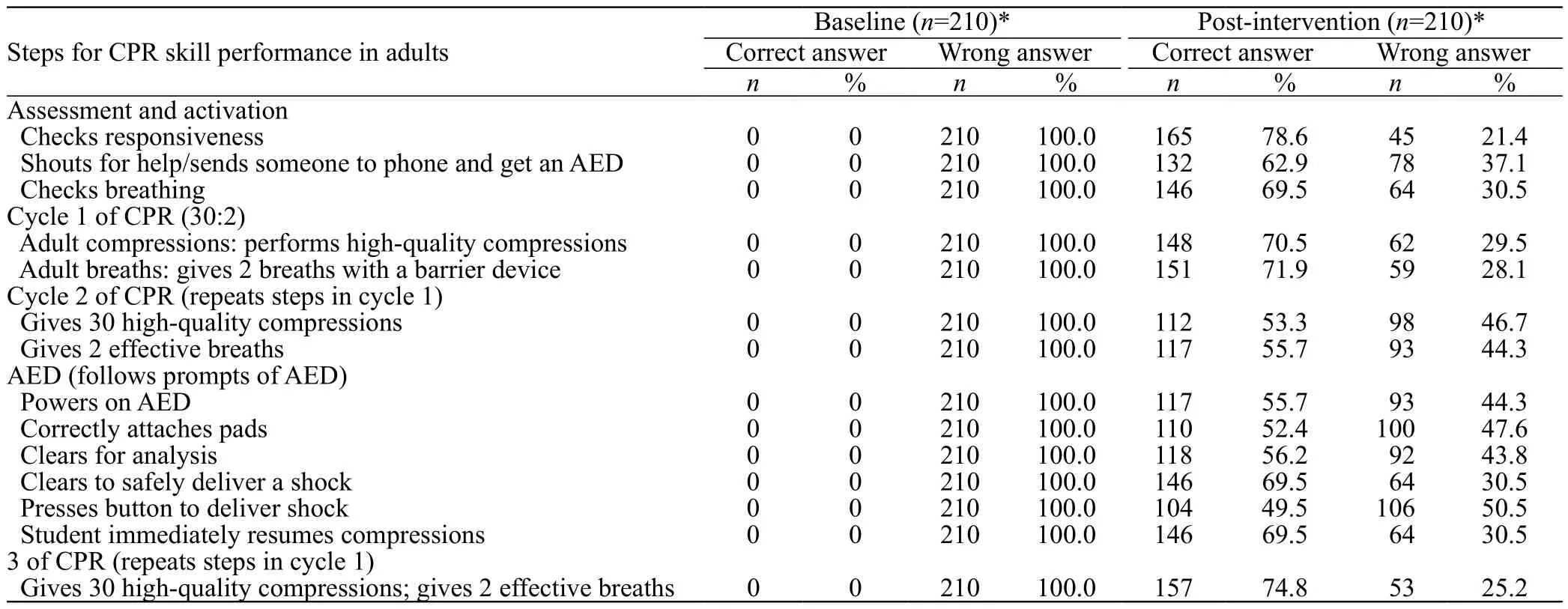
Table 4. Distribution of the answers provided regarding the psychomotor skill of BLS at baseline and post-intervention

Table 5. Comparison of the participants’ baseline, post intervention average knowledge and psychomotor skill scores
The comparison of psychomotor skill before and after training also shows significant difference (Table 5).Although the participants had virtually no CPR skills at the beginning, but after the training, the score changed significantly (P<0.000); they performed reasonably well in the “hands-on skills,” which is in agreement with the similar works of Meissner, Kloppe, & Hanefeld,[32]in that study, at baseline, 29.5% of the students performed chest compression as compared to 99.2% post-training. Hence,it was concluded that training in high school is highly effective considering the minimal amount of previous knowledge the students possessed.
Limitations
The research was conducted in one school in Nigeria.This limits the inferences that could be made about other populations of students in Nigeria. There could be some degree of bias because the study design used a non-randomised design. The study was conducted using manikins that may not provide the participants with the same competence as a real-life situation would provide.Sample size was calculated based on previous study;however, a larger sample size would have provided a better result in identifying the impact of the training programme on the participants.
Recommendations
We recommend the following:
1 The theoretical and skill training should be taught and repeated every six months in the secondary school.
2 We highly recommend that BLS/CPR modules are implemented as a mandatory part of the health education curriculum in Nigeria.
3 There should be more focus on ensuring sustainability of this training during education.
4 The timing of students training needs to be reconsidered, since they are likely to require basic life support skills.
5 Longitudinal study of this nature should be encouraged as it would demonstrate students’retention of the subject matter.
CONCLUSION
A majority of school students did not have basic knowledge of BLS. The study has demonstrated that students’ acquisition of BLS knowledge is adequate and that psychomotor skill after training is stable. It can be concluded in this study that the training was highly effective and significantly impacted where the baseline BLS knowledge low and psychomotor skill was virtually zero and post training gain in both BLS knowledge and skill.
ACKNOWLEDGMENT
The authors acknowledge the support received from the management and students of the Demonstration School, Ahmadu Bello University, Zaria. The authors also acknowledge all the staff and students of Anaesthesia Programme, Post Basic Nursing Programmes, Ahmadu Bello University Teaching Hospital, Zaria, Nigeria, and all who contributed to the success of the study.
Funding:None.
Ethics approval:Ethical approval was obtained from the Institutional Review Board (ABU/DS/EC/012/2018).
Competing interests:The authors have no conflict of interest, no financial issues to disclose.
Contribution:All authors have substantial contributions to the acquisition, analysis, or interpretation of data for the work;drafting the work or revising it critically for important intellectual content; and final approval of the version to be published.
 World journal of emergency medicine2019年2期
World journal of emergency medicine2019年2期
- World journal of emergency medicine的其它文章
- Keeping nephrotic syndrome on the emergency department edema differential: A case report
- Instructions for Authors
- A patient presenting painful chest wall swelling:Tietze syndrome
- Central nervous system manifestations due to iatrogenic adrenal insufficiency in a Ewing sarcoma patient
- Perceived effectiveness of infection control practices in Laundry of a tertiary healthcare centre
- Can an 8th grade student learn point of care ultrasound?