
Papillary cystadenoma of the parotid gland: A case report
2019-02-22 07:33:48LiWangShiKunZhangYingMaPatrickHaZhiMingWang
World Journal of Clinical Cases 2019年3期
Li Wang, Shi-Kun Zhang, Ying Ma, Patrick K Ha, Zhi-Ming Wang
Abstract BACKGROUND Papillary cystadenoma is a rare benign epithelial tumor of the salivary gland,which is characterized by papillary structures and oncocytic cells with rich eosinophilic cytoplasm. We found only one case of papillary cystadenoma in nearly 700 cases of salivary gland tumors. Our case was initially mistaken for a tumor of the right temporomandibular joint (TMJ) capsule rather than of parotid gland origin. Preoperative magnetic resonance imaging (MRI) and computed tomography (CT) should be carefully studied, which allows for appropriate preoperative counseling and operative planning.CASE SUMMARY Here, we report an unusual case of a 54-year-old woman with a parotid gland papillary cystadenoma (PGPC) that was misdiagnosed as a tumor of the right TMJ capsule. She was initially admitted to our hospital due to a mass anterior to her right ear inadvertently found 5 d ago. Preoperative CT and MRI revealed a well circumscribed tumor that was attached to the right TMJ capsule. The patient underwent a resection through an incision for TMJ, but evaluation of an intraoperative frozen section revealed a benign tumor of the parotid gland. Then we removed part of the parotid gland above the temporal facial trunk. The facial nerve was preserved. Postoperative histopathological findings revealed that the tumor was PGPC. No additional treatment was performed. There was no recurrence during a 20-mo follow-up period.CONCLUSION The integrity of the interstitial space around the condyle in MRI or CT should be carefully evaluated for parotid gland or TMJ tumors.
Key words: Papillary cystadenoma; Parotid gland; Temporomandibular joint; Case report
INTRODUCTION
Cystadenoma is a rare benign epithelial tumor of the salivary gland. It can be divided into mucinous and papillary subtypes[1]. It is mainly characterized by polycystic growth, with the epithelial component showing adenomatous hyperplasia[2]. It can occur in all the salivary glands, and is most commonly seen in the parotid and palatal glands[3]. For many years, the classification of cystadenoma and knowledge about its properties were unclear. Cystadenoma was once known as a cystic duct adenoma or oncocytic cystadenoma. This tumor was described in 1990 by the World Health Organization as a separate entity, which was classified as a subtype of salivary gland tumor[4]. However, in 2005, it was defined as a specific type of salivary gland epithelial tumor[5]. Papillary cystadenoma is easily confused with papillary cystadenoma lymphomatosum (Warthin tumor), due to their histologic similarity: papillary structures and oncocytic cells with rich eosinophilic cytoplasm. However, Warthin tumors are rich in lymphoid stroma. Here, we report a case of papillary cystadenoma of the right parotid gland, which was preoperatively misdiagnosed as a tumor of the temporomandibular joint (TMJ). The main treatment in this case included removal of the entire tumor and locally extended excision of the parotid gland. The histopathological diagnosis was papillary cystadenoma of the parotid gland.
CASE PRESENTATION
Chief complaints
A 54-year-old female patient was initially admitted to our department due to a mass anterior to her right ear inadvertently found for 5 d.
History of present illness
There were no significant changes in size since she found the mass. The patient complained of dull pain when she opened her mouth, but did not take any medicine for it.
History of past illness
At admission, her medical history was otherwise unremarkable.
Personal and family history
The patient was a nonsmoker, without personal or family history of other diseases.
Physical examination upon admission
On physical examination a palpable mass, about 2.5 cm × 2.0 cm, was found to be located near the right parotid region immediately anterior to the tragus. The mass had unclear boundaries, was fairly immobile, and was not tender.
Laboratory examinations
Laboratory results including complete blood count, electrolytes, and coagulation panels were within normal limits, with a white blood count of 4.21 K/μL, red blood cell count of 4.5 × 1012/L, and hemoglobin of 138 G/L.
Imaging examinations
Computed tomography (CT) revealed an occupying lesion just outside the right TMJ capsule. A clear capsule surrounded the mass, which contained cystic structures. The right mandibular condyle showed no evidence of bone destruction (Figure 1). Closedposition magnetic resonance imaging (MRI) revealed symmetrical bilateral TMJs without evidence of bone destruction. T2-weighted scanning showed a mixed polycystic lesion in the lateral right condyle. The mass measured approximately 2.0 cm × 1.6 cm. Open-position MRI showed stripe-like high-signal images in the right TMJ (Figure 2).
FINAL DIAGNOSIS
The preoperative diagnosis was a tumor in the right TMJ capsule. Although we strongly recommended a fine needle aspiration biopsy before surgery, the patient refused our suggestion due to her deep worry about the tumor spread.
TREATMENT
At surgery, we designed and performed an incision for TMJ, that was a 3 cm preauricular vertical incision and a 3 cm temporal incision in the hair line with an angle of 135° to the preauricular incision as described in the literature[6]. After further dissecting procedures, a cystic mass was found, which was loosely attached to the TMJ capsule. The mass was resected completely without opening the TMJ capsule. It measured approximately 2.0 cm × 1.5 cm (Figure 3). Evaluation of an intraoperative frozen section revealed a benign tumor of the parotid gland. Because the tumor was located within the upper part of the parotid gland, we decided to remove the part of the parotid gland above the temporal facial trunk. Thus, we extended the vertical incision down to the earlobe and then around it as an S-shaped incision for the parotid gland. After dissection anterior to the surface of the sternocleidomastoid muscle, the main trunk of the facial nerve was exposed. Dissection was performed along the temporal facial trunk, and the upper part of the parotid gland was resected.The facial nerve was preserved. This operation took 105 min and estimated blood loss was 60 mL. The patient’s postoperative course was uneventful. Postoperative histopathological examination found cystic regions that were lined by one to three layers of cuboidal or columnar cells. Multiple papillary projections extended into cyst lumens. The lumens contained eosinophilic material with inflammatory, scattered epithelial and foamy cells. Based on these findings, the patient was diagnosed with parotid gland papillary cystadenoma (PGPC) (Figure 4).
OUTCOME AND FOLLOW-UP
There was no recurrence during a 20-mo follow-up period according to postoperative CT.
DISCUSSION
Cystadenoma has also been reported to occur in intrahepatic bile ducts, the pancreas,ovary, epididymis, and kidney[7-11]. The prevalence of salivary gland papillary cystadenoma is low. In a study of 360 cases of salivary gland tumors, three patients(all female) were found to have cystadenoma of the parotid gland, which accounted for about 0.83% of all study tumors and about 1.0% of the benign study tumors[12]. A review of 30 cases of papillary cystadenoma of the minor salivary glands reported 17 male and 13 female patients[13]. Our study of 700 patients with salivary gland tumors during 2010 to 2016 found only one patient (female) with PGPC, which accounted for about 0.14% of all study tumors and about 0.15% of benign study tumors. We listed the reported cases of PGPC with comparatively complete data between 2009 and 2018 in Table 1[3,14-17], while solely retrospective studies without detailed data were excluded. Because of the rarity of cystadenoma of the salivary glands, the gender ratio of patients remains unclear and the etiopathogenesis of this disease has not been well discussed in textbooks and other published articles.
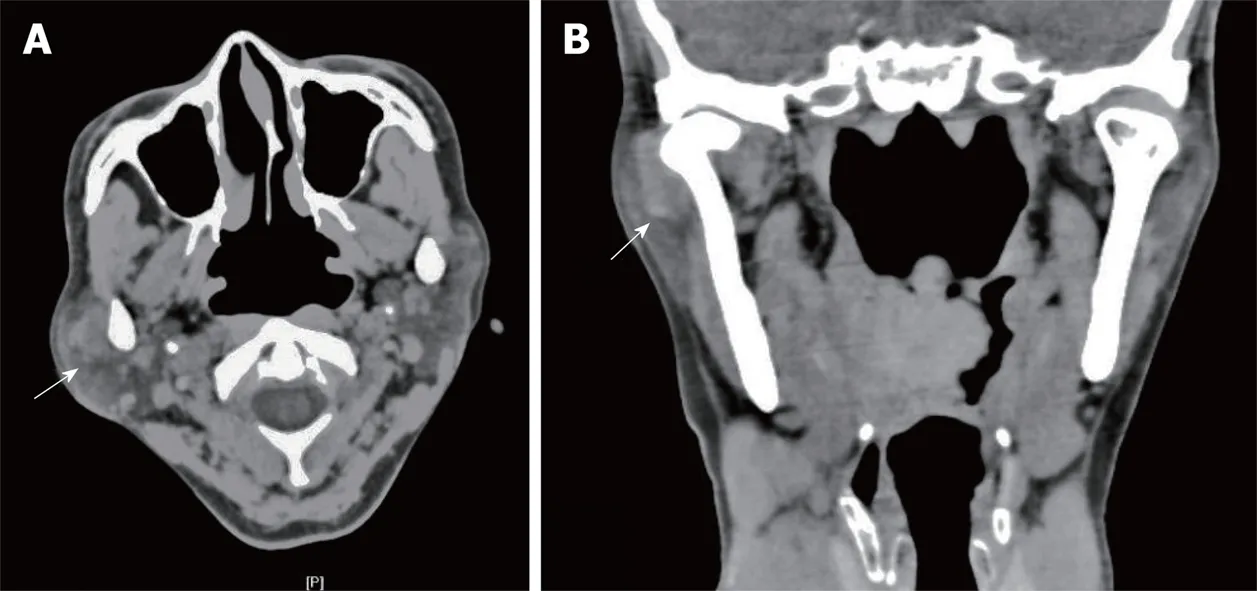
Figure 1 Computed tomography of the right temporomandibular joint. A: Axial computed tomography (CT)scan; B: Coronal CT scan. Axial and corona CT scans showed a clear semilunar mass (white arrow) surrounding the lateral aspect of the right temporomandibular joint (TMJ). The TMJ was free of bony involvement.
The preoperative imaging examinations of our case showed a well circumscribed mass. MRI of the parotid gland revealed a polycystic mass tightly surrounding the lateral and upper sides of the right TMJ capsule, which was misdiagnosed as a tumor of the TMJ capsule. However, during surgery the mass appeared to be a vascular malformation. The frozen section examination showed a benign tumor of the parotid gland that was diagnosed by postoperative histopathology as a papillary cystadenoma of the parotid gland. Therefore, the clinical manifestations and imaging examinations were not adequate for the correct definitive diagnosis. More notably, if the interstitial space around the condyle does not change and margin of the space is smooth in MRI, this indicates that the condyle is not damaged, and the mass is probably free of TMJ origin. Our case reminds surgeons of the utility of preoperative imaging, and surgeons should pay particular attention to the integrity of the interstitial space around the condyle in MRI, which stands for the condyle cortical plate. If the space is intact, the mass may come from the parotid gland, otherwise, it is of TMJ origin. Consequently, preoperative evaluation would potentially lead to a different incision design and an operative plan.
Surgical excision remains the main treatment of choice, despite the benign characteristics of this tumor; and the prognosis is good. Recurrence is seldom seen,with more tumors recurring in major salivary glands than in minor ones. Inadequate removal due to an incomplete capsule or tumor cell infiltration of the parotid gland is probably responsible for recurrence[13,18]. Although cystadenoma of the salivary gland is a benign tumor, postoperative malignant transformation has been reported[19]. A long-standing mass in the parotid gland may compress the facial nerve, causing hemifacial spasms[20].
The definitive diagnosis is made mainly on the basis of histopathological findings.Histologically, papillary cystadenoma is composed of well-defined unilocular or multilocular cysts, with intraluminal papillary projections[21]. The epithelial cells lining the cystic spaces are cuboidal or columnar, and the cystic structures are separated by a limited amount of interstitial tissue[13]. The differential diagnosis of papillary cystadenoma includes a variety of malignant and benign lesions, including Warthin tumor, intraductal papilloma, cystadenocarcinoma, and oncocytoma[13]. Warthin tumors are rich in lymphoid stroma. Sections of the lesion reveal multiple small cystic regions or a single large cyst surrounded by salivary gland lobules or connective tissue[22]. Intraductal papilloma is composed of dilated cystic ducts with papillary epithelial projections[23]. Oncocytoma is characterized by polyhedral oncocytic cells and absence of papillary projections[15]. Cystadenocarcinomas have structures similar to those of papillary cystadenomas, but cystadenocarcinomas have more cells invading the surrounding connective tissue[21,24].
CONCLUSION
We present an unusual case of PGPC that was mistaken for a TMJ tumor.Preoperative MRI and CT should be carefully studied for all tumors near this area in order to evaluate the integrity of the interstitial space around the condyle. This allows for appropriate preoperative counseling and operative planning. If possible,preoperative fine needle aspiration should be strongly recommended so as to distinguish the tumor’s nature and origin. In the future, more cases are helpful to learn about this disease.
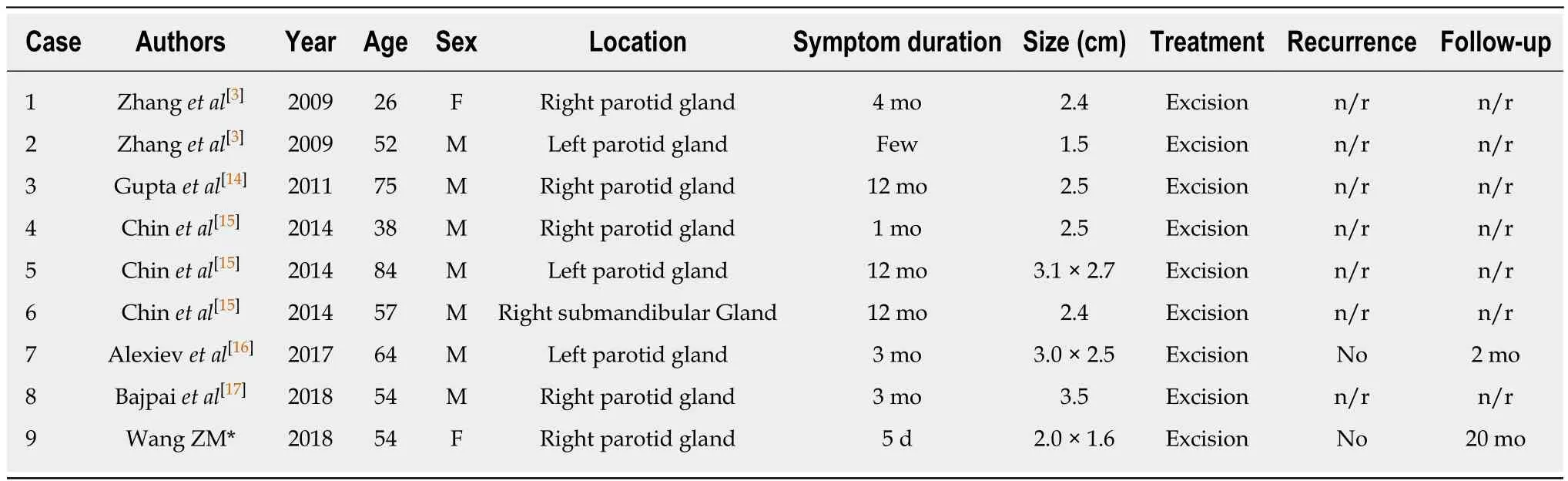
Table 1 Reported cases of major salivary gland papillary cystadenoma (2009-2018)
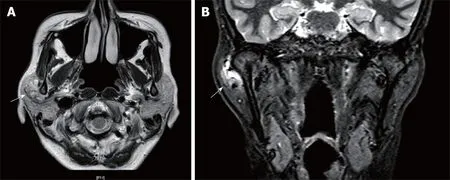
Figure 2 Magnetic resonance imaging of the right temporomandibular joint capsule. A: Axial T2-weighted scan; B: Coronal T2-weighted scan. Axial and coronal T2-weighted scans revealed a hypodense, multicystic, well circumscribed lesion, measuring 2.0 cm × 1.6 cm (white arrow), attached to the lateral side of the right temporomandibular joint capsule.
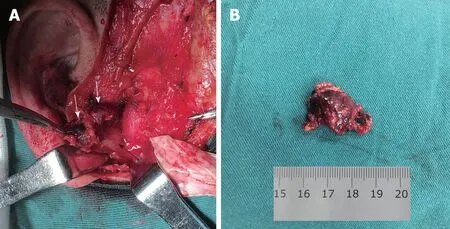
Figure 3 The cystic mass. A: The 2.0 cm × 1.5 cm mass was located lateral to the temporomandibular joint capsule, deep in the right parotid gland. The mass was soft and dark red in color, similar to a vascular lesion (Mass, white arrow; condyle, black arrow); B: The resected mass.
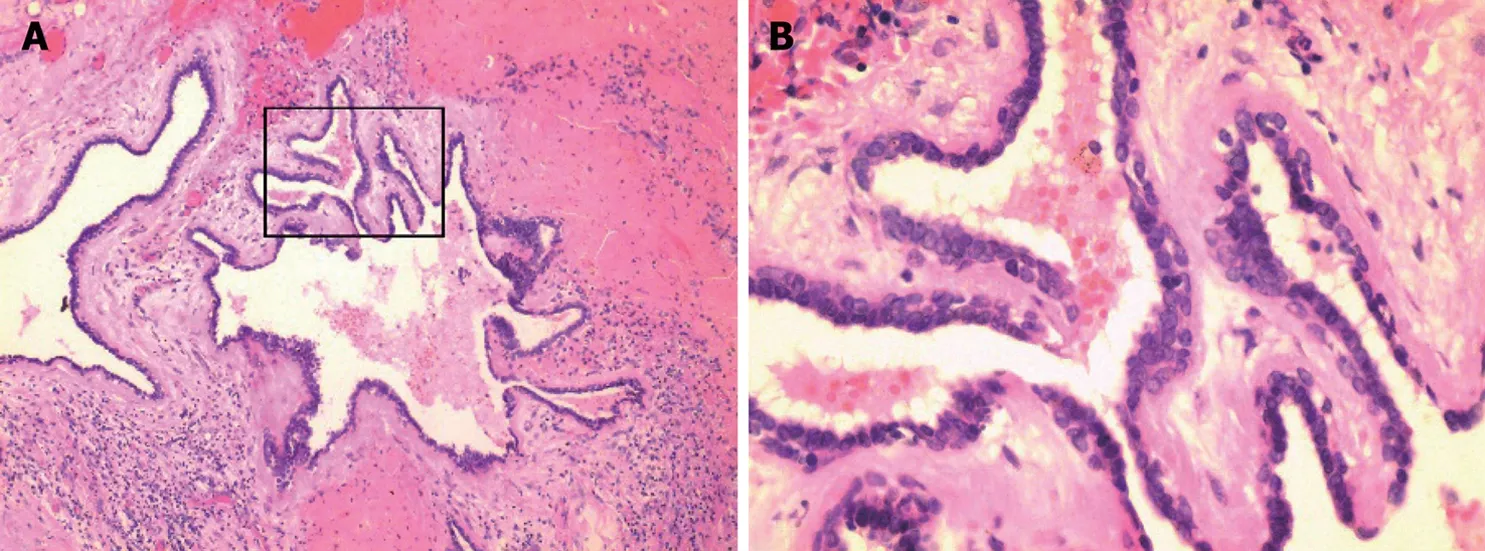
Figure 4 Postoperative histopathology. A: Cystic spaces with papillary projections supported by fibrous connective tissue and underlying capsular connective tissue; (H and E staining: ×100) B: The cystic papillary projections and the major cyst cavity were lined by one to three layers of oncocytic cuboidal or columnar epithelial cells. (H and E staining: ×400).
 World Journal of Clinical Cases2019年3期
World Journal of Clinical Cases2019年3期
- World Journal of Clinical Cases的其它文章
- Biventricular pacing for treating heart failure in children: A case report and review of the literature
- Gerstmann-Sträussler-Scheinker disease: A case report
- Considerations for routine coagulation monitoring with rivaroxaban:A case report and review of the literature
- Castleman disease presenting with jaundice: A case report and review of literature
- Ghost cell odontogenic carcinoma of the jaws: Report of two cases and a literature review
- Intravenous leiomyomatosis with different surgical approaches:Three case reports