
Symptom experience and symptom burden of patients following first-ever stroke within 1 year: a crosssectional study
2018-09-11 07:26DanShiZhengLiJianYangBangZhongLiuHuiXia
中国神经再生研究(英文版) 2018年11期
Dan Shi, Zheng Li, , Jian Yang, Bang-Zhong Liu, Hui Xia
1 School of Nursing, Fudan University, Shanghai, China
2 Xuhui District Center Hospital of Shanghai, Shanghai, China
3 Zhongshan Hospital Af filiated to Fudan University, Shanghai, China
Abstract Symptoms that are multidimensional and concurrent should be assessed from different dimensions and managed together. Few studies have evaluated concurrent and multidimensional symptoms in patients with stroke. Most studies of stroke focused on dysfunctions and complications. We hypothesize that patients with stroke have a heavy symptom burden within 1 year. This study aimed to describe multidimensional and concurrent symptoms within 1 year after stroke. This study recruited 230 patients with stroke from the Rehabilitation Department of Xuhui District Center Hospital of Shanghai and the Shanghai Sunshine Rehabilitation Center in China from March to September 2017. The patients’ multidimensional symptom experience and symptom burden were analyzed using a self-made structured questionnaire and the in fluential factors for symptom burden were identified. The mean number of symptoms in patients with stroke was 11.7 ± 3.5. More than two thirds of the participants suffered from at least 10 co-occurring symptoms. Unilateral limb weakness had the highest prevalence and frequency. Participation restriction had the highest symptom dimensions of severity and distress. Lack of self-care ability (severity), memory deterioration (frequency), imbalance of body (distress), moodiness (distress), being unable to move limbs at will(distress), shoulder pain (distress), and slower response (frequency) were independent factors of the total symptom burden score. These findings can provide essential information for efficient symptom management of patients with stroke. This trial was registered with the ISRCTN registry (registration number: ISRCTN18421629).
Key Words: nerve regeneration; stroke; burden; multidimensional; unilateral limb weakness; participation restriction; symptom management;concurrent symptoms; neural regeneration
Introduction
Stroke, one of the leading causes of adult disability and mortality (Bonita et al., 2004; World Health Organization, 2004),is a worldwide problem, especially in Asia (Kim, 2014).Many studies have focused on dysfunctions and complications after stroke in the past decades. With dissemination of a new medical model, health providers have realized the importance of patient-centered care. Symptoms have received an increasing amount of attention with the characteristic of subjectivity (Rhodes and Watson, 1987; Giardino and Wolf,1993; Lenz et al., 1997).
A symptom is defined as a subjective experience reflecting changes in biopsychosocial functioning, sensations, or cognition of an individual (Dodd et al., 2001). Symptoms should be assessed and managed from the individual’s perspective (Dodd et al., 2001). Being multidimensional, a symptom includes the dimensions of frequency, severity,and distress, which can be measured separately or in combination (Lenz et al., 1997). Multidimensional assessment can provide detailed information and reflect small changes in symptom experience (Portenoy et al., 1994). Furthermore,symptoms may occur at the same time, and these concurrent symptoms may interact with each other and group together in a systematic manner (Aktas, 2013). These co-occurring symptoms have a greater adverse effect on outcomes than individual symptoms (Aktas, 2013). Therefore, symptoms should be assessed and managed as a whole.
Symptom burden is a complex concept (Eckerblad et al.,2015), and can indicate the severity of symptoms summarily and reflect the patient’s perception of the effect of symptoms on daily living (Cleeland and Reyes-Gibby, 2002). Symptom burden can provide more information to inform treatment decisions and identify long-term effects of therapies compared with health-related quality of life (Burkett and Cleeland, 2007). The definitions of symptom burden are various.Symptom burden is defined as “the subjective, quantifiable prevalence, frequency, and severity of symptoms placing a physiological burden on patients and producing multiple negative, physical, and emotional patient responses” (Gapstur, 2007). Symptom burden is measured by the mean symptom experience of symptoms in a scale (Deshields et al., 2014; Eckerblad et al., 2015).
Many researches focus on symptoms in tumor patients.However, little is known about symptom experience and symptom burden in patients with stroke. Since the onset of stroke, patients experience diverse symptoms. These symptoms should be managed because they have a negative effect on rehabilitation and quality of life. To the best of our knowledge, few studies have assessed symptom experience in patients with stroke from different dimensions. Additionally,most studies on stroke symptoms have focused on a single symptom, such as depression (Ayerbe et al., 2013), anxiety(Ojagbemi et al., 2017), and hemiplegic shoulder pain (Vasudevan and Browne, 2014). Because most rehabilitation is provided within 1 year and rehabilitation in this period shows high benefits (Tistad et al., 2013), the stroke stage considered in this study was the first year.Based on clinical practice, we hypothesize that patients with stroke have a heavy symptom burden. Therefore, this study aimed to describe the multidimensional symptom experience and symptom burden within 1 year of patients having a stroke and to determine the influential factors of the symptom burden.
Subjects and Methods
Design
This study was part of a wider cross-sectional study that aimed to develop a symptom experience scale for patients with stroke and describe symptom experience among stable patients with stroke within 1 year of onset. The study was conducted according to the Declaration of Helsinki and was approved by the Ethics Committee of Nursing School of Fudan University,China (IRB#2017-4-3). All participants provided informed consent (Additional file 1) before participation.
Subjects
Convenience sampling was used to select respondents. Patients were potentially eligible for recruitment if they were hospitalized in the Rehabilitation Department of Xuhui District Center Hospital of Shanghai and the Shanghai Sunshine Rehabilitation Center in China from March to September 2017.According to the empirical method (the number of events per variable), the sample should be at least 5 to 10 times the number of variables (Concato et al., 1995; Peduzzi et al., 1995).There are 19 items in the Symptom Experience Scale for Stroke Survivors, which was used in this study; the sample of this study needed to be at least 95–190.
This study included patients who (1) were diagnosed with stroke within 1 year; (2) had a stroke attack for the first time; (3)could communicate by oral expression or writing accurately;and (4) gave informed consent. This study excluded patients who (1) were in the unstable stage; (2) had dementia or severe cognitive impairment; (3) developed complications that seriously delayed the rehabilitation process, such as gastrointestinal bleeding, fractures, tumors, and recurrent infections; and (4)had a cured malignant tumor for less than 5 years.
Data collection
After written informed consent was obtained, the patients filled out a structured questionnaire. The whole questionnaire was designed according to the Symptom Experience Model (Rhodes and Watson, 1987; Armstrong, 2003) and consisted of two sections: demographic and clinical characteristics and the symptom experience scale.
Demographic and clinical characteristics collected in this study included sex, race, age, education, marital status, job status, religion, medical insurance type, income per month, type of stoke, lesion location, stroke stage, rehabilitation time, comorbidities, knowledge about stroke (from patients’ perspective), and past experience of caring for patients with stroke.
Symptom experience and symptom burden were assessed using the Symptom Experience Scale for Stroke Survivors.This is a self-made and patient-completed symptom assessment tool for assessing patients’ symptom experiencesduring the preceding week. Nineteen symptoms are included and medical terminology that may be confusing to patients have an attached explanation through qualitative interviews. Participation restriction was defined as “cannot do the things you want to do because of stroke or rehabilitation”. Lack of self-care ability was defined as “cannot take care of yourself”. Strephenopodia was defined as shuf fling.Foot drop was defined as feet rolling inward. Each symptom was assessed in three dimensions (frequency, intensity, and distress). If a symptom was present, the frequency dimension was rated as rarely, occasionally, frequently, or almost constantly. The intensity dimension was rated as slightly,moderate, severe, or very severe. The distress dimension was rated as not at all, a little, somewhat, quite a bit, or very much. The average score of the three dimensions represented the symptom burden of this symptom (Abu-Saad Huijer et al., 2015). The mean score of the symptom burden of these 19 symptoms represented the total symptom burden of the patient (Deshields et al., 2014; Eckerblad et al., 2015). The Symptom Experience Scale for Stroke Survivors has good reliability and validity. The average scale-level content validity index was 0.947 and the item content validity index ranged from 0.800 to 1. The Cronbach’s α coef ficient was 0.810 and the split-half coef ficient was 0.760.
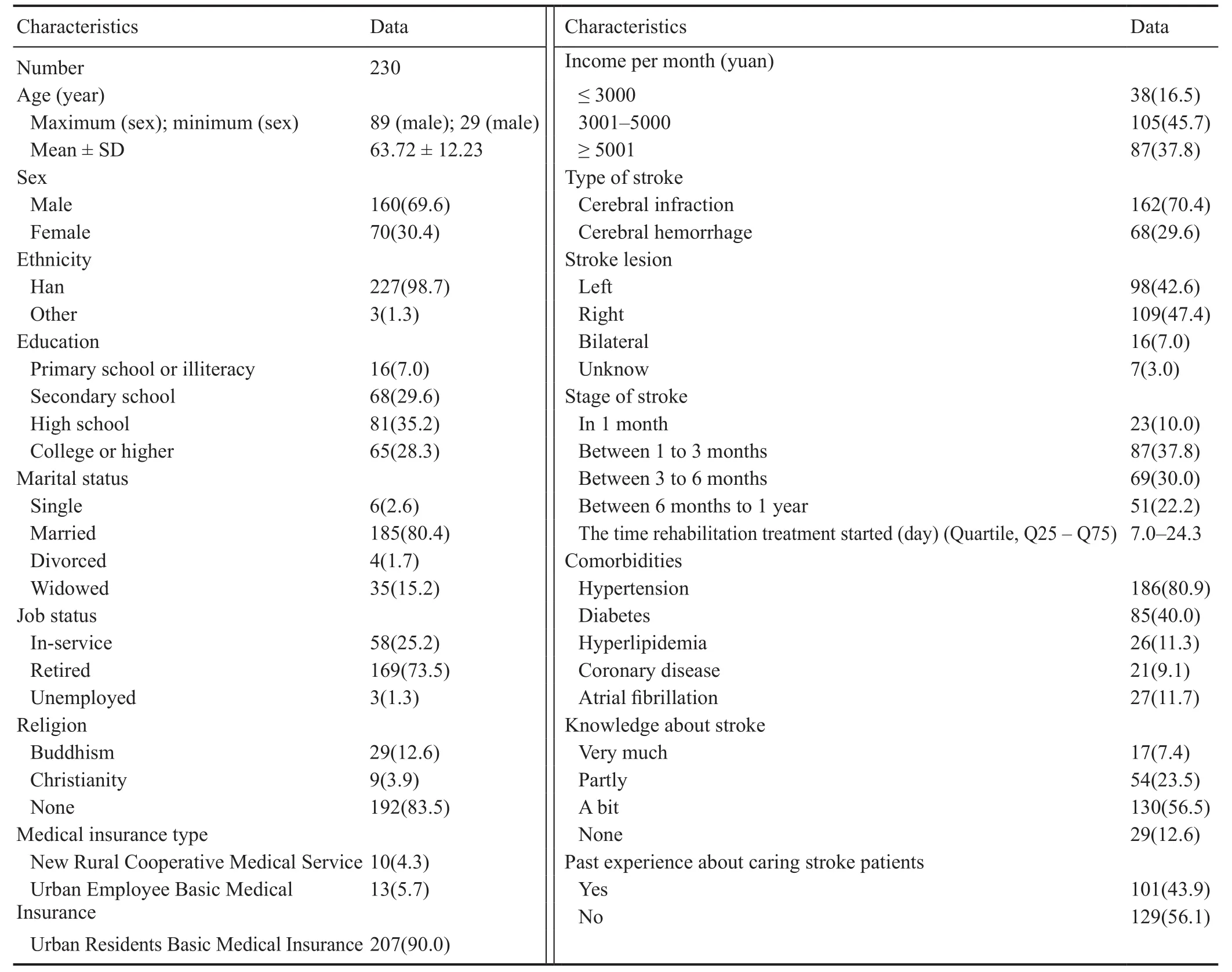
Table 1 Demographic and clinical characteristics of patients with stroke
Data analyses
Statistical analyses were conducted using IBM SPSS Statistics for Windows, Version 22.0 (IBM Corp., Armonk, NY,USA). Means and standard deviations (SDs) (quantitative variables) and frequencies and percentages (categorical variables) were calculated to describe various patients’ characteristics. The prevalence of symptoms was reported in simple proportions (numbers and percentages). Symptom burden was reported using mean and SD. The proportion of symptoms with a high frequency (frequently or almost constantly), intensity (severe or very severe), and distress (quite a bit or very much) (Eckerblad et al., 2015) was reported to emphasize the importance of those symptoms. The effects of demographic and clinical characteristics on the total symptom burden were analyzed by correlation analysis. Theeffects of individual symptom dimension on the total symptom burden were analyzed by multiple stepwise regression analysis. All tests were two-sided and the significance level was set at 0.05.
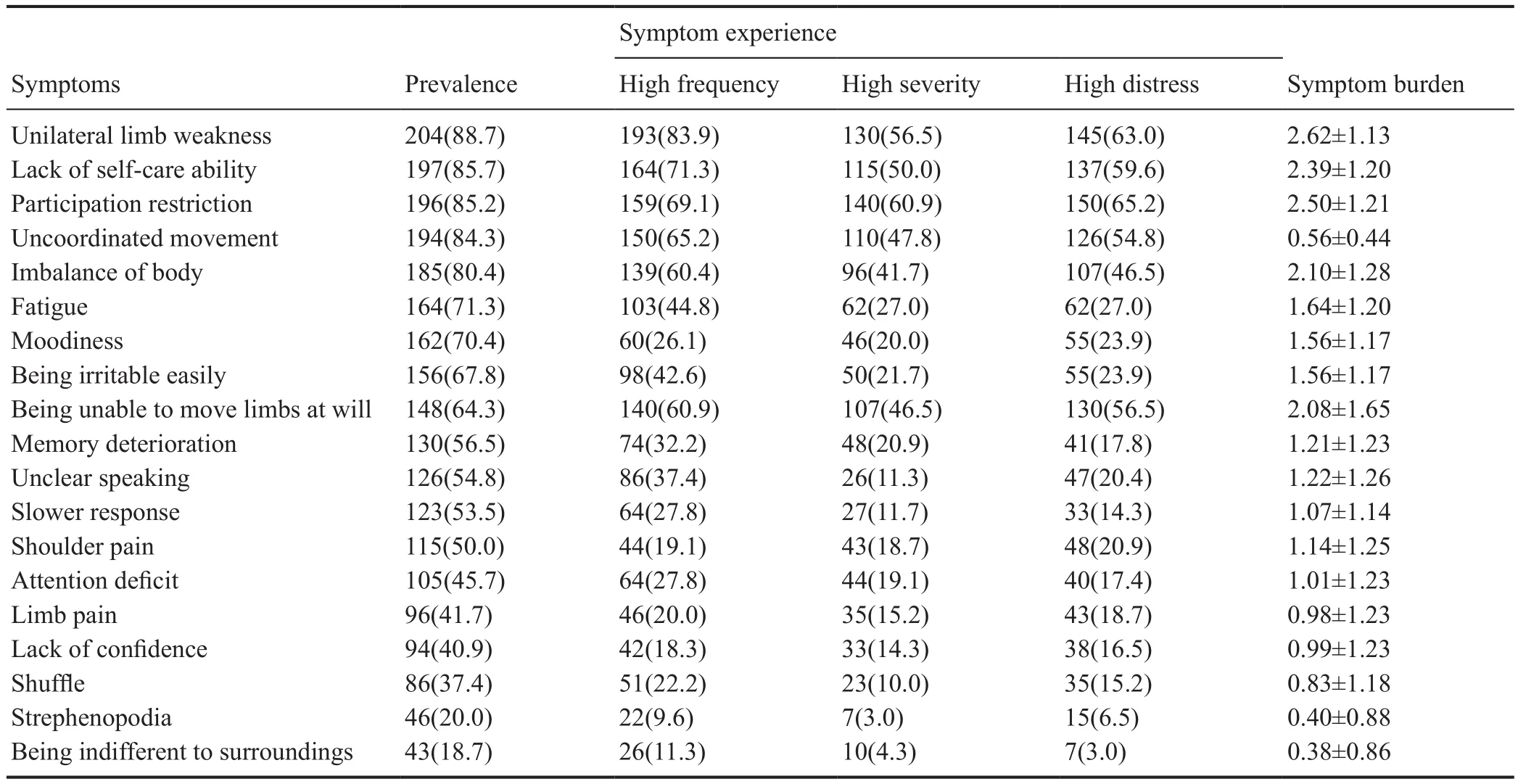
Table 2 Symptom prevalence, experience, and burden in patients with stroke
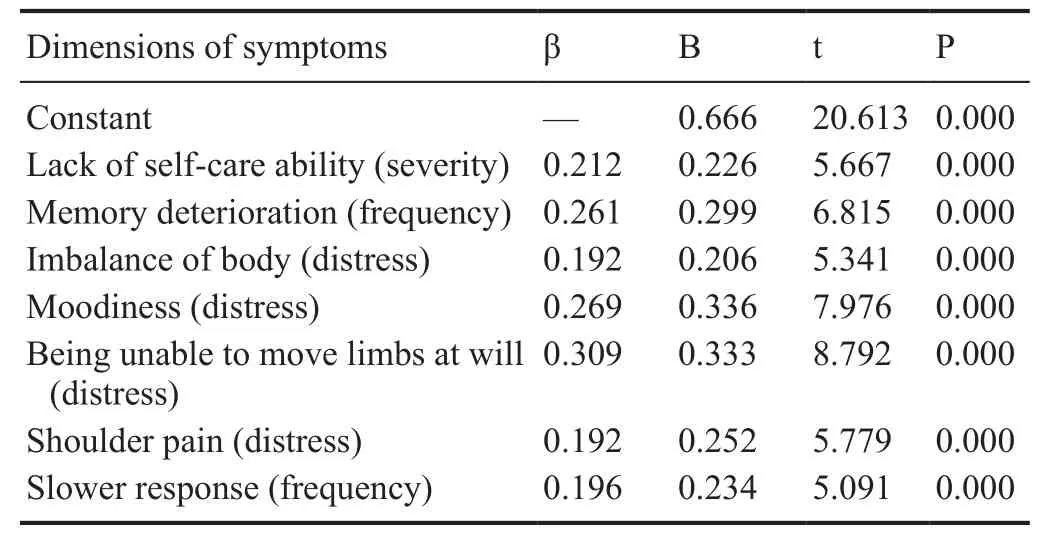
Table 3 Multiple stepwise regression analysis of the effect of dimensions of symptoms on the total symptom burden
Results
Demographic and clinical characteristics
A total of 230 patients with stroke were recruited. The mean age of these patients was 63.72 ± 12.23 years. The majority of participants were Chinese Han ethnicity (98.7%), men(69.6%), and had cerebral infraction (70.4%). The details of demographic and clinical characteristics are shown in Table 1.
Symptom prevalence
The mean value of stroke patients’ symptoms was 11.7 ± 3.5,ranging from 1 to 19. More than two thirds of the patients experienced at least 10 co-occurring symptoms. Among all of these 19 symptoms, unilateral limb weakness had the highest prevalence (88.7%). More than half of the participants (50.0–85.7%) reported lack of self-care ability, participation restriction, uncoordinated movement, imbalance of body, fatigue, moodiness, being irritable easily, being unable to move limbs at will, memory deterioration, unclear speaking, slower responses, and shoulder pain (Table 2).
Symptom experience
Unilateral limb weakness had the highest frequency where eight of 10 participants (83.9%) experienced a high frequency.Strephenopodia and being indifferent to surroundings had the lowest frequency (approximately 10%) (Table 2). Nearly two thirds of patients (60.9%) experienced high intensity in participation restriction. Approximately half of the patients(41.7–56.5%) had imbalance of the body, were unable to move limbs at will, had uncoordinated movement, had a lack of selfcare ability, and unilateral limb weakness was severe or very severe. Participation restriction and unilateral limb weakness were the most distressing symptoms reported by patients with stroke (65.2% and 63.0% respectively) (Table 2). The mean total symptom burden score was 1.37 ± 0.53. Symptom burden scores of these 19 symptoms are shown in Table 2. The symptom burden scores of unilateral limb weakness, participation restriction, lack of self-care ability, imbalance of the body, and being unable to move limbs at will were ≥ 2.0.
In fluential factors for the total symptom burden
Among demographic and clinical characteristics, education (rs= −0.176, P < 0.01), job status (rs= 0.139, P < 0.05),income per month (rs= −0.177, P < 0.01), type of stoke(rs= 0.147, P < 0.05), and health knowledge (rs= 0.192, P <0.05) were significantly correlated with the total symptom burden. Lack of self-care ability (severity), memory deterioration (frequency), imbalance of body (distress), moodiness(distress), being unable to move limbs at will (distress),shoulder pain (distress), and slower responses (frequency)were independently related to the total symptom burden in multiple stepwise regression analysis. R2of the model was 0.772, which indicated that 77.2% of the variance of the total symptom burden could be explained by these seven predictors (Table 3).
Discussion
Most studies of stroke symptoms focused on the occurrence of symptoms. Multidimensional symptom experience and symptom burden in patients with stroke have not been well studied. This study assessed three dimensions of 19 symptoms, and provided an in-depth evaluation of symptom experience and symptom burden of patients with stroke. This is the first study to comprehensively assess symptom experience and symptom burden of patients with stroke.
This study showed a considerable symptom burden in those with stroke within 1 year. Patients suffered from an average of 12 symptoms. The number of symptoms that patients with stroke experience is greater than that in patients with cancer(Abu-Saad Huijer et al., 2012; Deshields et al., 2014; Ritchie et al., 2014) and older community-dwelling people with multimorbidity (Eckerblad et al., 2015). In accordance with a previous study that compared symptom burden between heart failure and advanced cancer (Bekelman et al., 2009), our study showed that other chronic diseases may have an equal or larger symptom burden than that for cancer.
Among the 19 symptoms, 13 had a prevalence of higher than 50% in our study. The symptom of unilateral limb weakness had the highest prevalence (88.7%) and a high frequency(83.9%), which is similar to a previous survey on the same population (81.9%) (Shi et al., 2008). Limb weakness is the second most frequent symptom and the most frequent sign in the posterior circulation (Searls et al., 2012). Limb weakness is not specific to the pons and can be located in the internal capsule, basal ganglia, subcortex, and motor cortex (Shi et al.,2008). Limb strength can be improved by strength training,which can improve strength, functional capacity, and quality of life, and reduce the risk for subsequent cardiovascular events (Billinger et al., 2014; da Silva et al., 2015; Aidar et al.,2016). Slacklining can also provide measurable functional gains when incorporated into stroke rehabilitation programs(Gabel et al., 2016). Participation restriction is the most serious and distressing symptom for patients with stroke. Most participants (85.2%) in this study had participation restriction after stroke within 1 year. More than one fifth of stroke survivors are affected by participation restriction, even at 4 years after stroke (Gadidi et al., 2011). Participation is an important part in the World Health Organization International Classification of Functioning, Disability and Health (World Health Organization, 2001). Gait dysfunction is the main factor for participation restriction (Andrenelli et al., 2015).Global disability, older age, and psychosocial, cognitive, and environmental factors are correlated with participation restriction (Gadidi et al., 2011; Hamzat et al., 2014; Andrenelli et al., 2015). This suggests that for increasing stroke survivors’participation during recovery, psychosocial and biological factors should be included in a multidimensional treatment approach (Choi et al., 2015).
Frequency, severity, and distress are all important dimensions of a symptom. We found that different dimensions of a symptom may have different degrees of effect on symptom burden. In our study, severity of lack of self-care ability, frequency of memory deterioration, distress of imbalance of the body, distress of moodiness, distress of being unable to move limbs at will, distress of shoulder pain, and the frequency of a slower response were associated with the total symptom burden and could explain considerable variance. These results indicate that proper management of one dimension of these seven symptoms can greatly relieve symptom burden.
Although this study provides important descriptions about symptoms in patients with stroke and could be useful for future research, several limitations need to be acknowledged as follows. (1) We described stroke symptoms at 1 year poststroke without taking different stages of stroke into consideration. The symptom experience and symptom burden may differ in different time periods. Further studies are required to examine symptom experience and burden in patients with stroke at different stages. (2) The symptom instrument that we used contains the most common symptoms that patients with stroke may experience. We deleted a large amount of symptoms during development of the scale. Although this scale has good reliability and validity, there is a risk that the number of symptoms and symptom burden of patients with stroke may have been underestimated.
In conclusion, the symptom burden of patients with stroke is not less than that for patients with cancer. A large proportion of patients with stroke suffer from a high prevalence and frequency of unilateral limb weakness. Participation restriction was the most severe and distressing symptom in our study. Different dimensions of a symptom may have different degrees of effect on the symptom burden. People with a high severity of lack of self-care ability, high frequency of memory deterioration, high distress of imbalance of the body,high distress of moodiness, high distress of being unable to move limbs at will, high distress of shoulder pain, and high frequency of a slower response are at higher risk of facing a heavy symptom burden and might need prior management.
Acknowledgments: We are very grateful to all the participants and their families included in this study. We also thank the supports from the staff of the Xuhui District Center Hospital of Shanghai and the Shanghai Sunshine Rehabilitation Center in China for data collection.
Author contributions: ZL designed the study, controlled the quality of study and revised the paper. DS took part in the study design, collected data and wrote the paper. JY and BZL provided research places and gave professional guidance about stroke rehabilitation during the study. HX collected data. All authors approved the final version of the paper.
Conflicts of interest: The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Financial support: This study was supported by the Fuxing Nursing Research Foundation of Fudan University of China, No. FNF201611. The conception, design, execution, and analysis of experiments, as well as the preparation of and decision to publish this manuscript, were made independent of any funding organization.
Institutional review board statement: This study was approved by the Ethics Committee of Nursing School of Fudan University, China(IRB#2017-4-3). The trial was registered with the ISRCTN registry (registration number: ISRCTN18421629).
Declaration of patient consent: The authors certify that they have obtained all appropriate patient consent forms. In the form the patients have given their consent for their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity.
Reporting statement: This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement.
Biostatistics statement: The statistical methods of this study were reviewed by the biostatistician of Fudan University in China.
Copyright license agreement: The Copyright License Agreement has been signed by all authors before publication.
Data sharing statement: Datasets analyzed during the current study are available from the corresponding author on reasonable request.
Plagiarism check: Checked twice by iThenticate.
Peer review: Externally peer reviewed.
Open access statement: This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-Non-Commercial-ShareAlike 4.0 License, which allows others to remix,tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
Additional file:
Additional file 1: Patient consent form.
- 中国神经再生研究(英文版)的其它文章
- The unfolded protein response signaling and retinal Müller cell metabolism
- Sequencing of high-efficacy disease-modifying therapies in multiple sclerosis: perspectives and approaches
- Targeting prion-like protein spreading in neurodegenerative diseases
- Cadmium-induced neurotoxicity: still much ado
- Analysis of the traf ficking system in blood-brain barrier models by high content screening microscopy
- Retinal remodeling following photoreceptor degeneration causes retinal ganglion cell death