
A rare cause of foot drop: Tired bullet
2018-09-03 03:29:14EgemenEserVeliEmrerkmen
Egemen Küçük, Eser Gümüş, Veli Emre Türkmen
1 Emergency Department, Sakarya Universty Educational and Research Hospital, Sakarya, Turkey
2 Neurosurgey Department, Sakarya Yenikent State Hospital, Sakarya, Turkey
Dear editor,In some communities, the using of firearms during the celebrations have become a traditional behaviour.Injuries with free falling bullets that named “tired bullet” are increasing in accordance with the increased uncontrolled using of firearms. In the literature, serious disabilities and even deaths have been reported as a result of this rare injuries. We present a patient injured due to tired bullet with foot weakness and headache.
CASE
A fifteen-year-old male patient with complaints of headache and left foot weakness was brought to emergency room. During the examination, his measured blood pressure was 100/60 mmHg, heart rate 75 per minute, and oxygen saturation 99%. The patient’s Glasgow Coma Scale was evaluated as 15 points. The patient devoloped a headache after an object hitting to his head, while walking on the sidewalk about six hours before emegency room admission. After 1 hour of injury the patient developed numbness and loss of power in left foot which was gradually increasing.
During the examination of head, there was a hyperemic lesion of 0.5 centimeters diameter in a circular view with irregular edge, near the right parieto-occipital suture and at a distance of approximately 1 centimeters of the sagittal suture. There was no burning, blacking and tattooing around the wound. External examination of the whole body showed no signs of another injury. All of the systemic examination was normal but weaknesses of the left knee and ankle flexion and toe dorsiflexion without sensory loss were only positive signs in the neurological examination. The power of left ankle dorsiflexion and left toe was grade 1/5 and positive Babinski’s sign,hyper-reflexia in left deep tendon reflex were noted.Additionally peripheral pulses were detectable. In computerized tomography (CT) imaging of the patient,there was a intact bullet in the same area with skin lesion that penetrated brain parenchyma and caused a minimal contusion just under the bone (Figure 1).
Blood samples were taken for hemogram,biochemistry, coagulation parameters, and blood type analyzes. Tetanus prophylaxis, antibiotherapy and fluid resuscitation were applied and a consultation was requested from a brain surgeon. Finally the patient was admitted to the neurosurgery clinic. The value of Glasgow Coma Scale was not changed during emergency room management. After two weeks of surgery, we did a telephone interview with the patient, he complained of left leg numbness and partial dorsifl exion limitation.
DISCUSSION
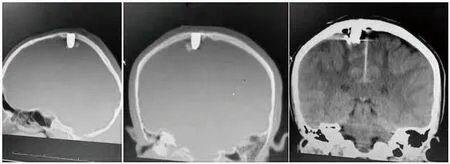
Figure 1. The computerized tomography (CT) imaging of patient.There was a intact bullet in the same area with skin lesion that penetrated brain parenchyma and caused a minimal contusion just under the bone.
Along with an increase in individual armament,uncontrolled using of firearms in social events such as newyear, childbirth, victory and wedding party,has become a progressive and important public threat.[1]In stray shooting to air, the bullet loses its energy and makes free falling motion, injuries related to this movement of the bullet are rare and referred to as tired bullet or falling bullet injuries.[2]In the literature, there are several case reports of chest, heart and limb injuries due to tired bullets, but the number of reports related to head injuries are limited.[3–5]However, Ordog and colleagues investigated 118 patients that had tired bullet injuries. In this study, they found head (77%–36%) and shoulder (12%–18%) were the most affected areas. In addition, mortality rate was reported as 32%.[6]In an experimental study made by Öğünç et al[7]gunshots made from different angles with different diameters of bullets, and possibility of injuries due to free falling bullets were investigated. They found total kinetic energy values of bullets that 9×19 mm and 7.65×17 mm in diameter, could penetrate skin and fl at bones. In addition,they found 65 falling tired bullet injury cases between 2000 and 2012 years in Turkey, 27 of these patients died and the mortality rate was calculated as 41.5% in such injuries. In accordance with the results of these studies,we determined an intact bullet that penetrated to brain parenchyma just under the right parietal bone of the head. In a study by Özdemir and colleagues, a 8-year-old female patient who had a frontal head gunshot wound during a wedding party was investigated. In this report,the tired bullet movement along with the brain and spinal canal was investigated. Unlike to our study, entrance of bullet was frontal region of the head and the path that the bullet travels was quite long.[8]In our study, bullet had entered the top of head at an angle of 90 degrees, and stopped just after passing through the parietal bone by losing its energy. It caused a mild contusion in the brain parenchyma. The extent of trauma in this type of injury depends on the type, kinetic energy and mass of bullets and the location of the injury area.[9]
Most prominent complaint of the patient was left foot numbness and weakness in our study, and power of left toe was grade 1/5 in neurological examination.Acute foot drop is a result of anterior tibialis muscle weakness and usually caused by peripheral nerve lesions and lumbar disc herniations.[10]Primary brain tumors and masses which are commonly at parasagittal location and affecting the pyramidal tract may result in foot drop.[11]In the literature, there are many case reports about foot drop that develops in relation with some lesions such as parasagittal located brain abscess,and meningioma.[12,13]And also there are many reports of foot drop that develops with trauma. In a study by Kang and colleagues,[14]they reported a 49-year-old male patient with head trauma due to falling from height and foot drop presented. Like to our study, neurological examination of patient was normal except for foot drop in this study. In the CT imaging of the patient, there was a sagittal suture fracture and hemorrhagic contusion in the left premotor area. In an another study by Atac and colleagues,[15]a 21-year-old male patient was presented.There was a superfi cial fi rearm injury at right parasagittal area of the head and the left foot dorsifl exion limitation was developed nearly 24 hours after the event. In the CT imaging of the head, there was a hemorrhagic contusion in parasagital area of the right parietal lobe. Similarly to these reports, there was a bullet injury and minimal contusion in right parasagital area of the brain in our study. Left foot drop was developed depending on these lesions.
CONCLUSION
To prevent this type of injuries, which may cause morbidity and mortality, individual arming and uncontrolled use of firearms should be limited.Additionally, in the cases of acute foot drop, falling tired bullet injuries should be kept in mind, because the possibility of injury around the parasagittal area is quite high in such injuries.
Funding:None.
Ethical approval:Not needed.
Conflicts of interest:The authors declare that there are no confl icts of interest relevant to the content of the article.
Contributors:EK proposed the study and wrote the fi rst draft. All authors read and approved the fi nal version of the paper.
 World journal of emergency medicine2018年4期
World journal of emergency medicine2018年4期
- World journal of emergency medicine的其它文章
- Subject index WJEM 2018
- Author index WJEM 2018
- Information for Readers
- Instructions for Authors
- Emergency department diagnosis of an ovarian inguinal hernia in an 11-year-old female using pointof-care ultrasound
- A case of thyroid emergency with cardiac arrest supported by extracorporeal membrane oxygenation