
A comparison of culture and PCR methods for identification of Aggregatibacter actinomycetemcomitans isolated from acute necrotizing ulcerative gingivitis
2018-07-26 09:59:50MaryamRamezFaramarzMasjedianJaziHamedTavakoliAbazarPournajafGholamrezaIrajianMeysamHasannejadBibalanBehzadEmadiBehroozYasini
Journal of Acute Disease 2018年3期
Maryam Ramez, Faramarz Masjedian Jazi, Hamed Tavakoli, Abazar Pournajaf, Gholamreza Irajian, Meysam Hasannejad Bibalan, Behzad Emadi, Behrooz Yasini
1Department of Microbiology, School of Basic Sciences, Islamic Azad University, Jahrom Branch, Jahrom, Iran
2Department of Microbiology, School of Medicine, Iran University of Medical Sciences, Tehran, Iran
3Clinic of Imam Khomeini Tehran, Iran
4Department of Microbiology, Faculty of Medicine, Babol University of Medical Sciences, Babol, Iran
5Department of Microbiology, Faculty of Medicine, Guilan University of Medical Sciences, Rasht, Iran
6Department of Microbiology, School of Medicine, Iran University of Medical Sciences, International campus, Tehran, Iran
Keywords:Aggregatibacter actinomycetemcomitans PCR Culture
ABSTRACT Objective: To determine Aggregatibacter actinomycetemcomitans (A. actinomycetemcomitans)isolated from periodontal patients and healthy subjects using culture and PCR methods.Methods: Duplicate paper point needles were taken from 100 samples (50 healthy subjects and 50 patients), who referred to the specialized dental clinic from Oct. 2015 to Mar. 2016. In laboratory after incubation period and observing the star-shaped colony A.actinomycetemcomitans, the confirmation tests, including gram staining and catalase test were carried out. For PCR, samples were analyzed with genus specific primers. These primers set,amplified a 500 bp fragment. Results: Of the 100 samples, A. actinomycetemcomitans was isolated from 31 patients (31%), (24 isolate of patients, and 7 isolate of healthy subjects) by using a selective Aggregatibacter isolation medium. Using PCR, a total of 49 (49%) samples were found to be positive for A. actinomycetemcomitans (35 isolate of patients, and 14 isolate of healthy subjects). Conclusion: PCR was found to be highly sensitive when genus specific primers were used for diagnosis of A. actinomycetemcomitans in comparison with culture method.
1. Introduction
The periodontal (gum) illnesses affect the gingivae, the periodontal ligament, connective tissue and the alveolar bone around the teeth with development of periodontal pockets due to the apical immigration of the junctional epithelium[1,2]. LAP or localized aggressive periodontitis and GAP or generalized aggressive periodontitis are specific types of the disease with obviously distinguishable clinical and laboratory results which make it adequately different from chronic periodontitis[3,4]. The periodontal illnesses are not classical exogenous infections, and there is a good sign that they are caused by the normal oral microbiota, mainly gram negative anaerobes[5,6].
A gram-negative, nonmotile and nonsprolating anaerobic coccobacillus calledAggregatibacter (Actinobacillus)actinomycetemcomitans(A. actinomycetemcomitans) that colonize in the human oral cavity has been concerned in the etiology of aggressive periodontitis (AgP), but it has also been related to chronic periodontitis[7-9]. Despite of oral infections, this organism has also been responsible for some systemic disorders, such as septic endocarditic, meningitis, wound infection, osteomyelitis, pneumonia,urinary tract infection (UTI), glomerulonephritis, pericarditis,arthritis, brain, lung and subcutaneous abscesses[10-12].
Traditional techniques used for identification ofA.actinomycetemcomitansincluding microbiological culture based with biochemical and immunological assays and DNA probes. However,these methods have some drawbacks in clouding; very low sensitivity and difficult to cultivateAnaerobic spp., time-consuming and tedious.So, nucleic acid amplification tests (NAATs) such as PCR is now a well-established and broadly used because they are faster and more reliable than conventional microbiological culture based techniques[13]. This study was performed in order to compare culture and PCR methods for identification ofA. actinomycetemcomitansisolated from of the periodontal pockets.
2. Materials and methods
The study population included cases of all age groups referred to the Imam Khomeini Specialized Dental Center in Tehran, Iran. The Imam Khomeini Hospital is one of the most equipped hospitals associated with the Tehran University of Medical Sciences (TUMS).In this cross-sectional project, based on the 95% confidence interval(CI) and by then=z2P(1 -P) /d2formula, sampling was done in a period of 6 months from Oct. 2015 to Mar. 2016. Thus, 100 samples were recovered from the healthy volunteers with any clinical signs of periodontitis (n=50) and patients with acute necrotizing ulcerative gingivitis (n=50). After recording and declare oral agreements, the persons were examined by periodontitis. Each patient showed a radiographic and clinical examination of alveolar loss confined to the incisor and molar teeth and periodontal pocket depth of ≥5 mm. Also,all periodontal patients and control groups have not received any antibiotics for the least two months prior of sample collection. Briefly,supragingival plaque was separated from the teeth by sterile cotton swabs and subgingival samples were collected from one periodontal site using two sterile paper points (Sybron Dental Specialties, Japan),placed in the depth of periodontal pockets for 60 s[14]. In the sterile conditions, one paper point needle placed on the trypticase soy agar petri dish supplemented with Horse serum, Bacitracin and Yeast extract) and then transferred to the laboratory[15,16]. All samples were cultured on the blood agar (Merck, Darmstadt, Germany) and incubated at 37 ˚C for 72 h. Direct examination was performed by the Phase-contrast microscopy for identification of star-shapedA. actinomycetemcomitanscolony (Figure 1). Template DNA was extracted from the star-shapedA. actinomycetemcomitanscolonies on blood agar (Merck, Darmstadt, Germany) by the High Pure PCR Template Preparation Kit (Roche, Germany). The PCR experiment was done using the DNA amplification device Mastercycler gradient(Eppendorf, Hamburg, Germany) for amplification of 16S rRNA region,ActF: 5’-GCTAATACCGCGTAGAGTCGG-3’ andActR: 5’-ATTTCACACCTCACTTAAAGGT-3’ [14]; in a total volume of 15 μL Master mix 1X (Ampliqon, Odense, Denmark) that contained 1X PCR buffer, 1.5 mM MgCl2, 1 μL template DNA (0.5 μg),0.15 mM dNTP, 1.25 U Taq DNA polymerase, 20 pmol of each primer and sterile distilled water up to 50 μL. A volume of 1.2 μL of extracted template DNA was added to a final volume of 25 μL PCR mixture counting 1.5 μL of 10 × PCR buffer, 2.0 μL MgCl2(50 mM),1.0 μL dNTPs (10 mM), 1.0 μL of each primer, 2.5 μL of Taq DNA polymerase (5 U/μL) (Ampliqon, Odense, Denmark) and 14.8 μL sterile distilled water. The thermal cycling protocol for PCR was;Denaturation at 94 ˚C for 5 min, 30 cycles with denaturation at 94°˚C for 30 s, annealing at 56°˚C for 30 s, extension at 72°˚C for 60 s and final extension at 72°˚C for 6 min. The amplified products were subjected to electrophoresis in a 1.5 % agarose gel for 1 h at 70 V with a 100-bp size marker (Fermentas, Massachusetts, United States),stained with GelRed™ Nucleic Acid Gel Stain (Biotium, USA), and photographed with ultraviolet illumination (Bio-rad, Hercules, USA)(Figure 2).A. actinomycetemcomitansATCC29523 was used as a reference strain.
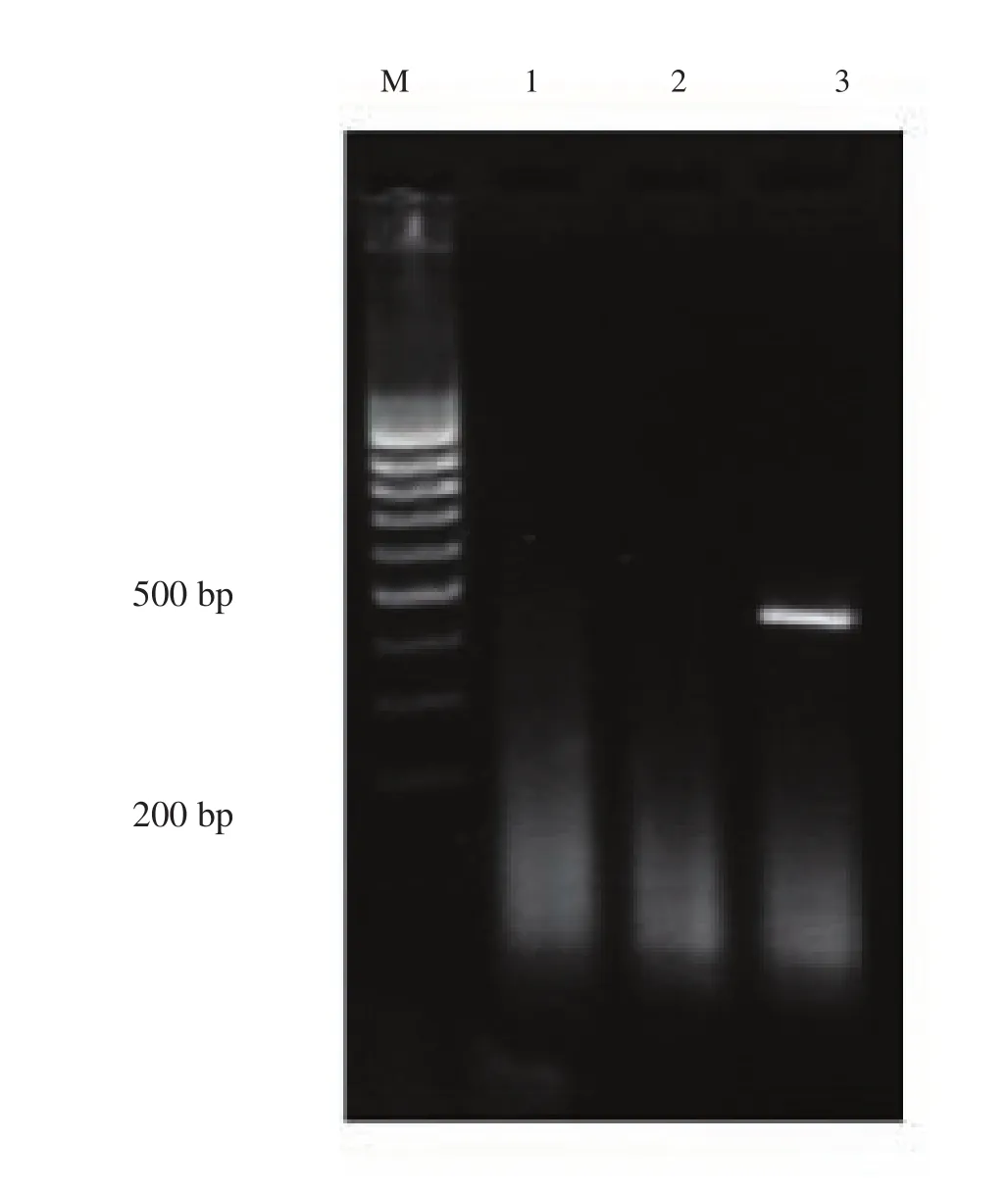
Figure 1. Agarose gel electrophoresis of PCR amplified products generated from patient DNA samples. Lane M is DNA size marker (100bp DNA ladder,SM#333). Lanes 1 is negative control showing no A. actinomycetemcomitans infection. Lane 2 is negative sample showing no A. actinomycetemcomitans infection. Lane 3 shows 500 bp A. actinomycetemcomitans.
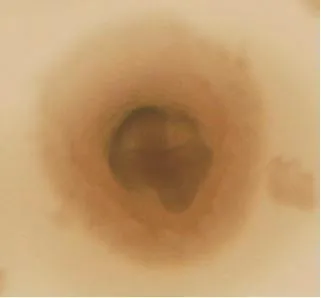
Figure 2. Star-shaped colony of A. actinomycetemcomitans bacterium below a phase-contrast microscope.
3. Results
A total of 100 non-repetitive samples were collected from patients with acute necrotizing ulcerative gingivitis and healthy subjects.The mean age of the patients studied was 35.3 years ±11.7 years)(range from 17 years-71 years). In patients group (n=50), 22 (44%)and 28 (56%) non-identical samples were collected from the female and male, respectively. So, of 50 healthy subjects, 24 (48%) were female and 26 (52%) were male. The distribution analysis ofA.actinomycetemcomitansby culture based method showed that 48%and 14% of strains were obtained from the periodontal patients and healthy individuals, respectively (Table 1), but 70% and 28%of samples were positive forA. actinomycetemcomitansin the PCR method.

Table 1Prevalence of A. actinomycetemcomitans in plaque samples[n, (%)].
As shown in Table 2, culture and PCR results in healthy individuals and patients have been compared and showed that 33 cases(68%) were positive in both PCR and culture-base methods, but 3 cases (6%) were positive in a culture but not PCR. Statistical analysis showed that a significant relation between pocket depth and the presence ofA. actinomycetemcomitansin the periodontal patients (P<0.05). On the other hand, there is a direct relationship between the depth of the pocket and the presence of theA.actinomycetemcomitans(Table 3).

Table 2Comparison of PCR and microbiological -culture based method [n, (%)].
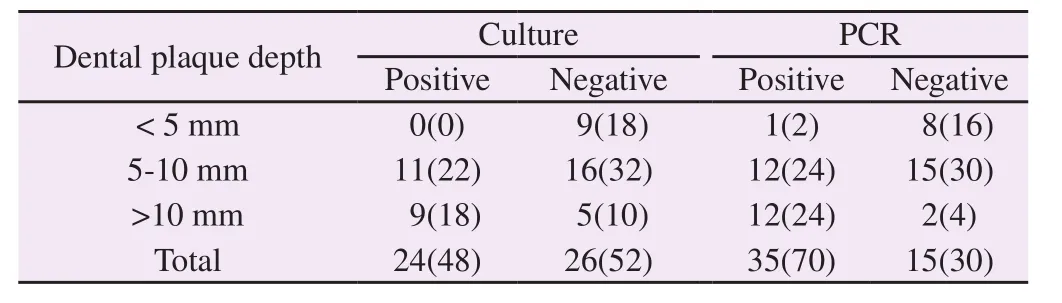
Table 3Relative abundance distribution of the A. actinomycetemcomitans by the depth of plaque in patients with periodontal through PCR and culture[n,(%)].
4. Discussion
There are more than 300 bacterial species in the periodontal pockets, may participate in periodontal pockets. Some of these bacteria, such as:A. actinomycetemcomitans,Porphyromonas gingivalisandTannerella forsythiaplay a significant role in emerging advanced forms of periodontal illness[1,2]. The presence ofA. actinomycetemcomitanscan be considered as an alarming for development of periodontitis and a marker in the progression of inflammatory responses[7,8,17]. Rapid and sensitive identification ofAggregatibacteris very important because it’s also related to severe systemic disease such as endocarditis (HACEK group), meningitis,pericarditic, osteomyelitis, aspiration pneumonia, septicemia and brain abscesses[8,12,14].
In the study,A. actinomycetemcomitanswere obtained from 48%and 14% in the culture method from the periodontal patients and healthy individuals, respectively. In PCR method, 70% and 28% of samples collected from periodontal patients and healthy person were positive forA. actinomycetemcomitans. These results are very similar to Riggioet al, which used for PCR and culture for detection ofA. actinomycetemcomitansin periodontal patients. They showed that the prevalence ofA. actinomycetemcomitanswere 24% and 15% in PCR and culture methods, respectively[18].
The lower extent of culture bacterial detection in this investigation can be related to environmental factors (pH, CO2, temperature and materials present in culture media and clinical specimens) and loss of viability during specimen collection and/or transport[19,20]. This results is in agreement with Avila-Camposet al[14], Urban and his colleagues[11]and Riggioet al[18]. In the present study, sensitivity and specificity of PCRvs.culture were 90.9% and 100.0%, whereas, Avila-Camposet alwas reported that the sensitivity and specificity of PCR versus culture were 93% and 95% respectively[14]. In this study directed by Avila-Camposet al, 6% samples were infected withA.actinomycetemcomitansby culture method but not 16S rRNA PCR assay. The PCR false-negative results may be due to the presence of inhibitors of Taq DNA polymerase, traces of blood, antibiotics,sequence variability and genome degradation.
Analysis of PCR amplification products by restriction enzymes indicated that all bacterial species belonged to one type (data are not shown). Furthermore, no sequence divergence has been detected in all the PCR-amplified products. Therefore, targeting the 16S rRNA gene forAggregatibacterPCR detection has proven to be a specific as well as a conserved target for laboratory probing ofA. actinomycetemcomitans. Riggioet al[18] described that PCR is a powerful investigative tool that can identify low numbers of periodontal pathogens in subgingival plaque specimens. It is quick,not time consuming, inexpensive and not laborious than conventional culture base methods. It can also determine a large number of pathogens in a reaction. They declare that PCR is a “gold standard”for detection of main periodontal pathogens in subgingival plaque samples.
Generally, the study results showed that the prevalence of theA. actinomycetemcomitansin the patient group is higher than the healthy group. In other words, the bacterium exists in a low concentration at the dental plaques in healthy individuals, but in a various condition, such as poor dental hygiene and dental surgery,this opportunistic organism can grow and multiply as a dangerous bacterium. So, rapid detection ofA. actinomycetemcomitansmight be of great benefit since chair-side identification could inform patients of the existence of this pathogenic microorganism.
Conflict of interest statement
The authors report no conflict of interest.
 Journal of Acute Disease2018年3期
Journal of Acute Disease2018年3期
- Journal of Acute Disease的其它文章
- Traumatic optic neuropathy secondary to acupuncture treatment for glaucoma: A case report
- Cost analysis and characteristics of the patients admitted to emergency service with poisoning
- Scoring systems in prediciting mortality rate of patients applying emergency department
- Earthquake planning and crisis management with an emphasis on the facilities, utilities, and services of the health care centers of Tiran and Karvan County, Isfahan Province, Iran: A case study
- A survey on the epidemiology of trauma and China trauma care training in subtropical regions of Hainan Province
- Traditional Chinese Medicine and its protective function over braininjured patients