
Traditional Chinese Medicine and its protective function over braininjured patients
2018-07-26 09:59:48AdringelInchauspe
Journal of Acute Disease 2018年3期
Adrián Á ngel Inchauspe
Hospital "Dr. Alejandro", Melchor Remero-La Plata, Province de Buenos, Argentina
Keywords:KI- 1 Yongquan maneuver CPR rescue Vascular acute brain injury Post-stroke neurological recovery
ABSTRACT Acupuncture is actually convoked for supporting Western Medicine. Its “Golden Points”can undoubtedly help patients during its neurological recovery. After almost thirty years of experience in saving patients at impending death situations and having made numerous contributions on the field, the author herein provides a reasoned survival bio-energetic circuit based on a detailed methodological and functional analysis of the Main Channels and the Wondrous Vessels (Qi jing ba mai) participating in it. K-1 Yongquan complementary resuscitation maneuver, systematized since 1987, has been consistently performed in sudden death and cardiac arrest conditions as a final resource in both basic and advanced CPR failure. Experimental analytical studies identify the prevention, control and assessment of treatments set up as well as the determination of their efficiency. Acupuncture K-1 Yongquan Resuscitation Maneuver is presented not only as a complementary CPR rescuer but as a protective aid for both traumatic and vascular acute brain injury. Current indications of KI-1 Yongquan are not limited to actuarial results in cardiac arrest resuscitations, but it functions as a brain protector in both traumatic and vascular brain injury situations should be included. Although many acupuncturists indicate only standard techniques for bio-energetic rehabilitation, it has not been noticed that they insist with greater emphasis in those specific points to stimulate the“Sea of Marrow” (encephalon). Divulgation of K-1 emergency therapeutic possibilities look for its inclusion into Critical Care Protocols, in order to upgrade survival rates in both cardiac arrest and stroke victims. Traditional Chinese Medical balancing effect principle can improve cognitive, intellectual and psycho-motor patterns after even severe brain injuries. Beyond the scientific methodology that supports it the efficiency of the maneuver derives mainly from the sustained increase in survival rates presented in the successive statistics published in renowned scientific journals since its application.
1. Introduction
Divulgation was not limited to actuarial results in cardiac arrest resuscitations, but KI-1 Yongquan function as a brain protector in both traumatic and vascular brain injury situations through the“Survival Axis” (Figure 1) should be included.
Although many acupuncture ´s attended to this Congress, only standard techniques for bio-energetic improvement were shown[1-3]without emphasis in those specific points to stimulate the “Sea of Marrow”.
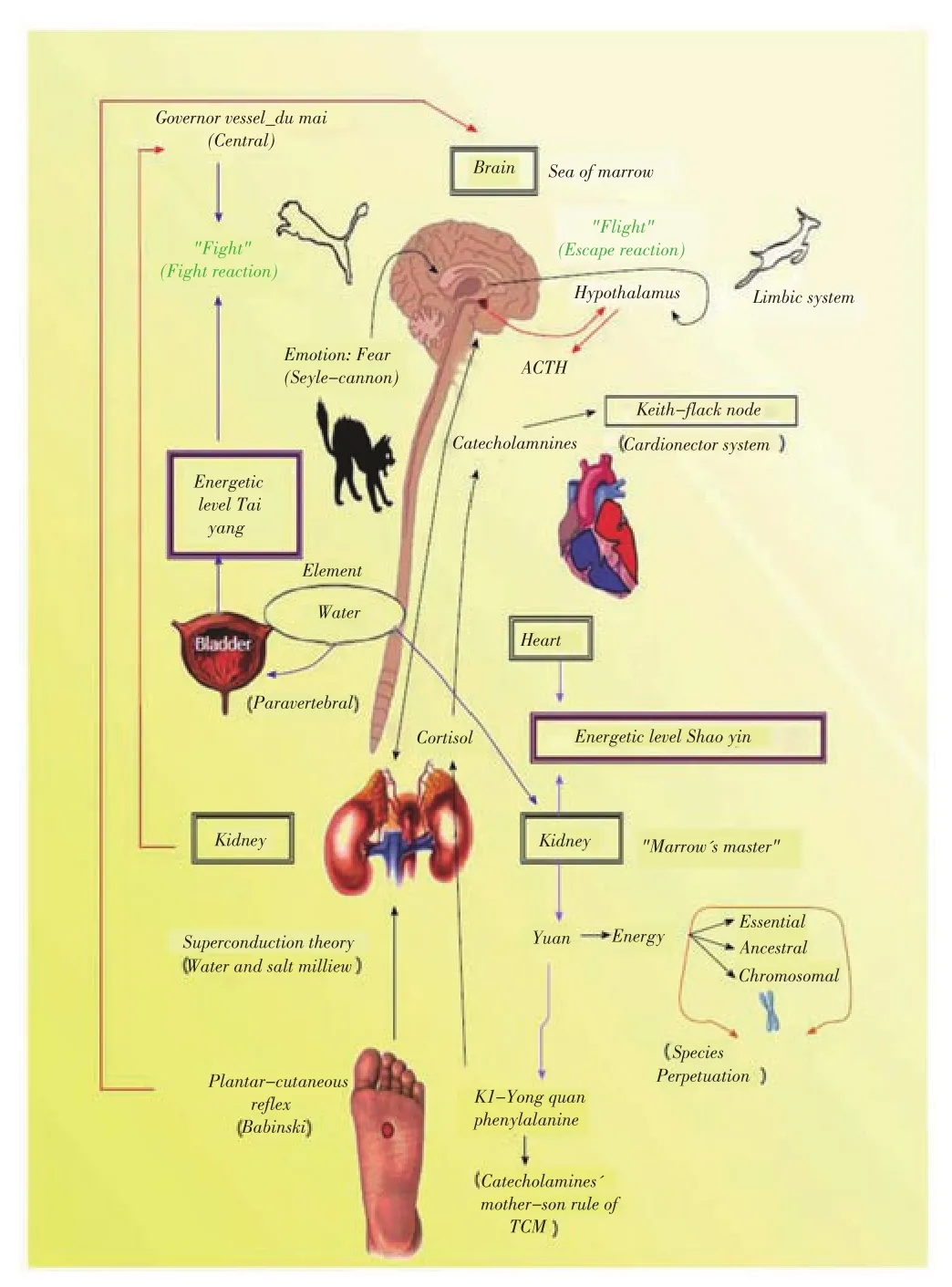
Figure 1. Survival axis.
Acupuncture is actually convoked for supporting Western Medicine. Its “Golden Points” can undoubtedly help patients during its neurological recovery. Traditional Chinese Medical Qi‘s balancing effect principle can improve cognitive, intellectual and psycho-motor patterns after even severe brain injuries.
Reported benefits of specific therapy over the “Sea of Marrow” can considerably aid in this situations.
In December 2011, fifty-one cardiac arrest victims with only 9 deaths were presented in In Tech´s “Recent Advances in Theories and Practice in Chinese Medicine”[4].
Currently, these numbers climb up to 89 patients with only 14 deaths. All of them underwent both basic and advanced CPR protocol failure before Yongquan pressing point application, with a Glasgow score of 3.
Recent WHO statistics positioned cardiac arrest and stroke as the two most frequent of overall causes of death: 1stcause is cardiovascular diseases, accounting for 23%; the 2ndcause is vascular brain injury, accounting for 7%. The joint percentage is 30%.
In order to reveal how extreme the K-1 resuscitation maneuver is,four particular cases are introduced showing clinical severe brain damage that completely reverted the situation. The third case it is shown as an example of the transcendence of the original Qi as the essential energy is the only able to provide the necessary power to restore vital signs if there exists renal indemnity.
2. K-1 maneuver application
2.1. Case 1: G.L.
Female, 47; admitted in Dr. Alejandro Korn Hospital in July, 2005 for gigantic eventration. After pre-surgical pneumoperitoneum, she underwent a vasovagal reaction with severe hypotension followed by cardiac arrest (11 a.m.). Due to failure of the basic and advanced CPR, K-1 maneuver was performed until her beats, cardiac activity and hemodynamic condition returned to normal. After reaching controlled haemodynamic stability, neurological tests were performed by on-duty neurosurgeon, that formally confirmed right hemiplegia.
The specialist found the patient suddenly impaired in her censorious, with hemodynamic instability. It was noticed a left conjugate eye deviation and general flaccidity, without response to painful stimuli.
Through KI-1 Yongquan continuous stimulation, her general flaccidity gradually reverted (3-4 min.). While coming back to consciousness, she began to move the left side of her body–the right one was still paralyzed until she recovered all her body´s mobility.The previous impaired condition reversed progressively from hemiplegia to right hemiparesia without any motor focus or kind of sequel to normal state (1:10 p.m.), allowing the patient to go to the bathroom on her own.
2.2. Case 2: G.M.
Male, 3 years old; admitted in Dr. Alejandro Korn Hospital Duty. Brought to pediatric shock room (11:25 a.m.) with loss of consciousness, pale, hypotonic, and was found in such condition by parents 15 min before arrival to Medical Duty. Pulse absence was confirmed with patient in apnea, bilateral mydriasis and sphincter relaxation. Duty doctors began the rescue with endotracheal intubation, chest compression and drug treatment: adrenalin via endotracheal tube; atropine and bicarbonate at pediatric usual doses.Hidrocortisone was also indicated for neural protection. After 15 minutes of reanimation, ICU cooperation was required; and ECG evidenced 118/min rhythm when electric activity without pulse was diagnosed. Vital support was maintained for 60 min. Interpreting outlined ECG as an automatic rhythm, ICU doctors left the place.
On consulting with surgeons for an alternative venous access,bilateral plantar pressure K-1 point maneuver was performed,with recovery of normal heartbeats (12:45 p.m.)(Figure 2). Urgent transfer to La Plata Children´s Hospital was accepted, with arrival time 1:55 p.m. We were informed about the child´s extubation 36 h later, personally verifying his awakening.

Figure 2. Case 1. pedriatic case rescued at Alejandro Korn & Sor María Ludovica Hospitals- La Plata, Argentina.
2.3. Case 3
Woman, 56 years old, admitted to a private clinic. Antecedents of congenital pathologies: Aneurysms of the Polygon of Willis.
She has congenital giant polycystic kidney disease and was subjected to bilateral nephrectomy and renal transplant, previous to cerebral vascular injury.
She was admitted for haemorrhagic ACV post-rupture of aneurysm in polygon of Willis.
She had decompressive craniotomy and PIC screening; but the next week she repeated the bleeding for a second aneurysm.
Reintervention and intensive treatment with pharmacological sedation for a month. After this period, hypno-analgesia is removed in order to evaluate its neurological status. When no answer was obtained, the application of Maneuver on the KI-1 Yongquan point was suggested and agreed upon.
Reaction obtained from an “attempt to awaken and incorporate”,with an unsuccessful return to wakefulness.
The previously mentioned ablation of the kidneys made irreversible her lack of essential renal energy, making it impossible to recover her from coma.
2.4. Case 4
Premature 700 g baby was attended in the Sbarra Hospital and then transferred to Sor María Ludovica Interzonal Hospital. Admitted flaccid, without pupillary reaction and generalized arreflexia(Figure 3).
Considered stillborn (not actually birth, because he had absence of vital signs); he suffered empyema in right eye; generalized petechial rush and an acute suppurative meningitis (suspected septic abortion consequences).
KI-1 Yongquan plant massage was intensively applied in both soles. Recovery of vital signs was immediately positive and vital signs completely restored.

Figure 3. Case 4: premature 700 g baby rescued by KI-1 Yongquan Resuscitation Maneuver.
3. Discussion
Quoted alternate and bilateral plantar pressure, firmly applied over Yongquan acupuncture point under any body posture and circumstance was briefly published in 2010[5].
In 89 patients in impending death situations for stroke or cardiac arrests, even in extreme critical impairment (skull fracture)[6], KI-1 helped vital organs and consciousness to recovery but failed to modify natural evolution in 14 cases(Figure 4).
The other 75 cases kept with a remarkable longstanding outcome.Matching with actuarial survival rates–less than 5%[7] in extrahospital rescues and 19% in best Emergency Units–K-1 application results quite over this average(84.27%)[8].
From them, 52 cases suffered stroke after severe hyper or hypotension episodes–among another kind of brain injuries(trauma)–meaning only 15.73% of overall deaths left of this trial.In China, Dr. Zheng L[9] referred in his “Acupuncture treatment for persistent vegetative state after operation of acute subdural hematoma”, the KI-1 use for coma due to this pathological condition.
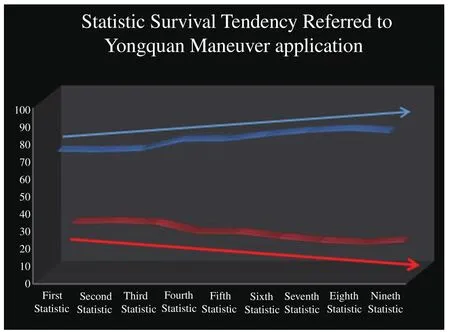
Figure 4. Statistical Tendencies of KI-1 Yongquan maneuver´s survival rates.
Either to recover facial paralysis (personal experience) for treating persistent or intractable hiccups (singultus) in post-stroke lateral medullary syndromes[10] (that highly impedes normal breathing) cases with or for post-stroke urinary retention[11]; or post-stroke motor aphasia[12], KI-1 Yongquan point has been also used as a valuable rehabilitation aid for post-stroke complications.
In both situations of motor aphasia and singultus; KI-1 Yongquan has been principally combined with PC-8 Lao Gung. This suggestion of Fei, Cai and Xu[12]. It is absolutely coincident with the hypothesis presented regarding the existence of the“Reconciliation Vessel”. A new marvelous channel discovered by the author in the ancient classics and endorsed in the I-Ching that involves the kidney, heart and pericardium meridians as a key component of Survival Axis.
Dr. Randall Benner, M.Ed., NREMT-P suggests the posterior rubbing chest massages and the rubbing plantar pressure (“Scrub planting”) in his work: “Childbirth and related emergencies”[13].Quoted maneuver has been recommended since 1999 by AHA[13].
Dr. Daniel Ceraso, President of Pan American and Iberian Federation of Critical Care Medicine and Intensive Care, remarked the relevance of non-pharmaceutical therapies in ICU. Specifically concerning to acupressure and foot massage, these patients were given a strong recommendation with light evidence (C-1) in the “Practical clinical guidelines based upon evidence for sedoanalgesia management in grown-up patients with critical illness”[14].
Actual prognosis of brain injury sequels[15] exposed during last 9thIBIA Congress includes new imaging as positron emission tomography[16]; and biomarkers as salivary cortisol[17] and S100B neuronal protein[18-20]. These tests can help to follow-up this critical patients, screening its recovery and evolution.As in case III, only in total absence of the organs carrying the Yuan (i.e., bilateral renal ablation) it will be impossible for KI-1 maneuver to fully comply with TCM resuscitation functions[21].
4. Conclusion
Babinski plantar cutaneous reflex and its utmost semiological value keeps out of discussion. The Babinski reflex or plantar skin reflex in the adult consists in performing a plantar stimulus with a blunt object, from the outer edge of the heel, following the path near the outer edge of the foot, and making an internal arch through the head of the metatarsals towards the big toe( Figure 5).
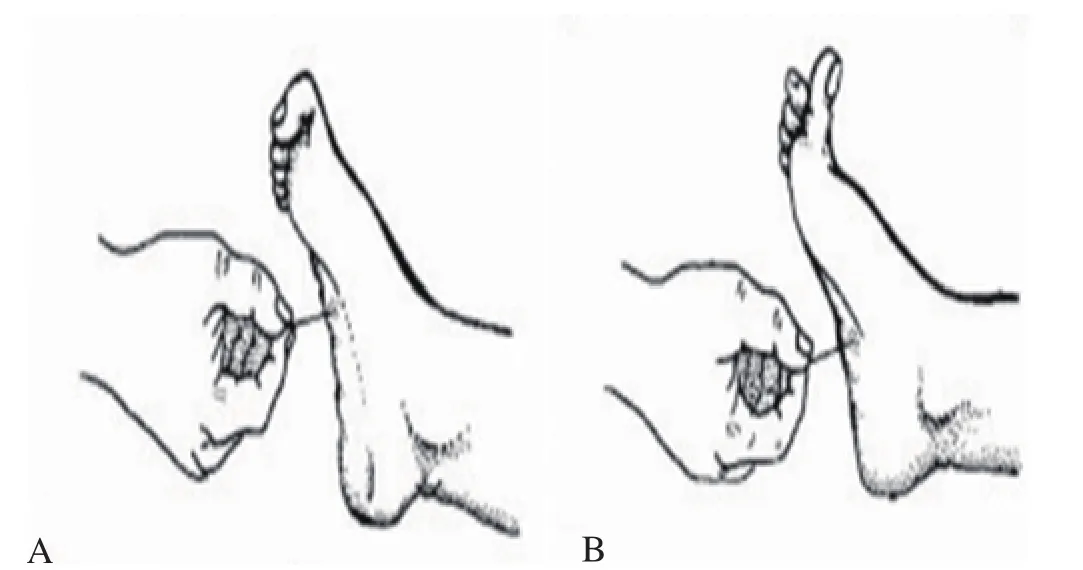
Figure 5. Babinski plantar cutaneous reflex.
In the infant , Babinski’s reflex occurs when physician gently passes his hand down the sole of the foot (from the heel to the big toe). The expected response is to extend the fingers and turn the foot inward. Its normal estimated duration is between the first six months and two years of life[22].
After age 2, hallux extension results patognomonic of a cortexpyramidal lesion, testing only with a pin scratch in the sole of the foot. Babinski’s sign is an aseptic reflex that in the adult consists in a movement of extension (dorsiflexion) of the first toe in response to a stimulus in the plant thereof, due to the contraction of the extensor digitorum longus muscle, with or without separation of the the other fingers (“sign of the fan”). The plantar flexor response is the normal motor act expected before the stimulus. Therefore, in the adult the expected response consists of the flexion of the fingers. The pathological response, in front of an injury of the first motor neuron,consists of an extension of the fingers, with slight abduction of them and dorsiflexion of the foot .
Unlike adults, in the baby, the response with dorsiflexion is normal, due to the immature nature of the corticospinal tract, which is reached around 3 years approximately. If this sign persists after this period as stated before, it will be necessary to perform a deeper evaluation, since there would be a high probability that quoted route is damaged and we would be possibly facing a superior motor neuron syndrome.
As we can see in shown text and illustrations, there is an intimate topographical relationship between the course of the“scratching” of Babinski’s reflex and the corporal situation of KI-1 Yongquan acupuncture point(Figure 6). It is not strange then to understand how this site results linked to possible conditions pathophysiological events that occur in the encephalon, making clear again the deep relationship between ancient knowledge and that of the modern era.
K-1 Yongquan is the only place where the Yin or Nurture Qi enters from the Earth through our body energy system before reaching the Lungs and Heart. In this way, the last organs will be able to elaborate Zheng Qi or Central (thoracic) energy for its vital priority of his active cardio-respiratory function. This is the key function of Reconciliation Vessel: to reset the activation of the“Survival Axis”, recovering cardio-respiratory activity, as well as quoted neuro-motor and neuropsychic functions.

Figure 6. Similarities between KI-1 resuscitation maneuver and Babinski plantar reflex.
There is proven experimental scientific evidence of the therapeutic possibilities of Acupuncture in brain-damage situations[23,24].Thus, the main objective of this work was to highlight the potential benefits that the stimulation of point KI-1 Yongquan can provide in brain-damaged patients.
Conflict of interest statement
The author reports no conflict of interest.
 Journal of Acute Disease2018年3期
Journal of Acute Disease2018年3期
- Journal of Acute Disease的其它文章
- Traumatic optic neuropathy secondary to acupuncture treatment for glaucoma: A case report
- Cost analysis and characteristics of the patients admitted to emergency service with poisoning
- A comparison of culture and PCR methods for identification of Aggregatibacter actinomycetemcomitans isolated from acute necrotizing ulcerative gingivitis
- Scoring systems in prediciting mortality rate of patients applying emergency department
- Earthquake planning and crisis management with an emphasis on the facilities, utilities, and services of the health care centers of Tiran and Karvan County, Isfahan Province, Iran: A case study
- A survey on the epidemiology of trauma and China trauma care training in subtropical regions of Hainan Province