
Factors behind not using child restrain(t) among hospital employees and general population:A case control study
2017-12-15 09:08EmadSiddiquiBadarAfzalGhazalaKaziAsherFerozRubabaNaeemTarabMansoorAhreenAllanaSaifSiddiquiZainSiddiqui
Emad Siddiqui, Badar Afzal, Ghazala Kazi, Asher Feroz, Rubaba Naeem, Tarab Mansoor, Ahreen Allana, Saif Siddiqui, Zain Siddiqui
Department of Emergency Medicine, Aga Khan University Hospital, Karachi, Pakistan
Original Article
Factors behind not using child restrain(t) among hospital employees and general population:A case control study
Emad Siddiqui, Badar Afzal, Ghazala Kazi, Asher Feroz, Rubaba Naeem, Tarab Mansoor, Ahreen Allana, Saif Siddiqui, Zain Siddiqui
Department of Emergency Medicine, Aga Khan University Hospital, Karachi, Pakistan
Child restrain; Seat belt; Injury; Pakistan
INTRODUCTION
Injury has been recognized as a major public health concern in today's world and motor vehicles continue to claim a huge number of children's lives annually. Most of these unintentional injuries occur in developing countries,with South East Asia being a major contributor.[1]Injury related deaths are estimated to rise from 5.1 million to 8.4 million by 2030 and will be the third major cause of disability adjusted life years (DALYs) by then.[2]
Road traffic injury (RTI) is the most important cause of unintentional injury related mortality and morbidity in children between 1 to 14 years of age in high income countries (HIC) and has been shown to be responsible for 23% of deaths in this age group.[3]In the USA, there were 1 538 deaths in children less than 14 years with motor vehicle crashes (MVC) in 2009.[4]
A rising trend of RTI related morbidity and mortality has also been observed in low and middle income countries(LMIC), with a 600% rise in Mexico, 450% increase in Thailand, 250% in Venezuela and 210% in Chile,[5,6]while in South East Asia, there was 231 000 MVC related deaths during 2008, and would be expected to raise to 500 000(with 117% rise) in children under 14 year age.[2]
According to Hertz et al[7]and Rice et al,[8]the use of child restrain (CR) can minimize the mortality and morbidity associated with motor vehicle injuries by 71% and 73% in infants and 59% and 76% in toddlers respectively. In South Korea, the use of CR brought about a decline in mortality from 809 to 202 during 1995 to 2007 and in the USA, CR accounted for a 71% reduction in motor vehicle associated deaths in children.[9–12]
The use of child restraint and seat belts is highly popular in developed countries like Australia (92%) and Canada (91%).[11]However, in low income countries the rates are relatively low, with data from Mexico and Nigeria reporting a 17.4% and 18.6% usage respectively.[12]On the contrary, in developed countries of Asia, the rates are still lower compared to the Western world. Research has found CR usage in South Korea and Japan to be 22.4% and 47%respectively.
Pakistan with only 18 vehicles (cars)/1 000 population,[13,14]belongs to LMIC (with GDP of $ 243.6 billion in 2014), with total population of >185 million,while 64 million (34.5%) children below 14 years.[13]The country's expenditure on the health sector accounts for only 2.5% of total GDP.[15]The total number of car accidents in 2010 was reported to be 9 747 with more than 5 000 deaths and more than 11 000 injuries.[16]As far as motor vehicle related injuries in children are concerned,previous studies from Pakistan have shown that MV related injury was the commonest cause of all pediatric injuries (80%),[17]though most MVC injuries were under reported or missed. Despite such a high rate of mortality associated with motor vehicles, CR use was observed to be 29%.[18]This study was conducted amongst the well educated population of the country where traffic safety rules are circulated from time to time and we hypothesize that learned and educated population of the study center are more aware of the safetyness of child restrain seat belts. The objective of this study was to determine the rate of CR usage in both the educated and uneducated population of the country. We also tried to assess the attitude of Pakistani drivers towards the use of CR and the factors that promote or limit CR usage. This study will provide the background for launching policy initiatives in Pakistan and will contribute to increasing the awareness of the masses with regards to safety measures and their role in injury control and prevention.
METHODS
This was a case control study with controls from the Aga Khan University and cases from the general population (GP) in a 1:3 ratio. The controls were AKU employees who were assumed to be more educated and aware of CR usage. The data collection was done from 2009 to 2010.
After institutional approval, data was collected from all five districts of Karachi. A questionnaire was developed and tested. It consisted of parameters like gender, education, awareness, presence and frequency of usage of CR and seat belts (SB), number of children in the family, attitudes towards CR usage and reasons for not using it. Data collectors were trained by the PI. After taking informed consent, the data collectors explained the participants the purpose of the study and the difference between adult seat belts and CR. The questionnaire was made in both English and Urdu language and was distributed amongst parents/drivers of both genders and all ethnic and socioeconomic groups who drove with children under 14 years of age. Drivers who owned vehicles other than cars and those without children in the family were excluded.
The controls were educated volunteers from the Aga Khan University who were requested to fill out the questionnaire while for the cases, data was collected from drivers at shopping malls, cinemas, restaurants, highways and offices. A total of 1 046 drivers were approached out of which 848 (81%) responded. The study population was heterogeneous with respect to education, ethnicity and socioeconomic background.
Questionnaire
We used a 36-item data collection tool which was pretested and translated into Urdu for better understanding of the participants. The questionnaire consisted of close ended questions that were used to gather information regarding the participants'demographic details, occupation and economic status,number of children, awareness regarding CR and SB,availability and usage of CR and the reasons behind nonusage. The questionnaire also inquired the type of SB and CR that the participants were using, validity of the drivers' license and parental knowledge and awareness about CR usage. The source of awareness about the use of CR was also determined. Any misfortunate incident involving children that might have altered the parents' practices and their attitude towards CR usage was determined. Outcome variables were calculated by scoring together 3 items comprising of questions on frequency and importance of usage and source of information regarding CR and SB use. Overall, there were 18 questions on the usage trends of SB and CR.This was to ensure that the participants appreciated the difference between the two and also helped reduce information bias. The direct benefit of the study to the participants was that it helped provide them insight about their practices which might be putting their children at risk and increase awareness about CR usage.
Statistical analysis
The data was entered and analyzed using SPSS v.20 and frequencies and percentages were tabulated. Chi-square test was used for categorical variables with the dependent variable being the presence of CR in the participant's car to identify factors influencing CR usage. Crude ORs were obtained using 95%CI. Multivariate logistic regression was used to explore associations between risk factors and outcomes, and results were tabulated in terms of adjusted ORs with 95%CI.P≤0.25 was considered to be adequate for the multivariate model. Multi-co-linearity and interaction was also determined. All predictors and covariates were first examined at the univariate level and kept for multivariate model if found significant. Alpha was taken as 0.05, with a Confidence Level of 95%.
RESULTS
The data was collected from 848 participants with a response rate of 81%. Out of the total car users (n=848)included in the survey, 212 participants were from AKU while 636 belonged to the GP. Among the 212 participants from AKU, 59.4% were male compared to the GP group which had 69.8% male drivers (P=0.005). Questions on the education status of the participants revealed that in AKU, the majority of the subjects (i.e., 96.7%) had atleast acquired a bachelors degree, while less than half (42.6%)of those from the general population were graduate or above (P<0.001). However, driving license possession was found to have no significant difference between both the two groups (Table 1).
One of the primary reasons for not using child restraint is lack of awareness and therefore, we aimed to determine the level of awareness of CR among our study population.A statistically significant difference was found between the two groups with drivers from AKU being generally more aware about CR and its usage. 81.1% of the group from AKU compared to 59.7% from the general population were found to be aware of child restraint use (P<0.001).
In addition to being aware of CR usage, it was integral to identify the source of information regarding CR use. Amongst the AKU employees, 40.6% claimed to have acquired information through the media, while another 23.6% reported other sources and 18.9% weresimply uninformed. Media was found to be the biggest source of information for the general population group as well with 24.1% of people reporting it to be their primary source of information and the remaining attributing their knowledge to friends and family and other sources. In this group, 40.3% of people had no information regarding CR use (P<0.001).
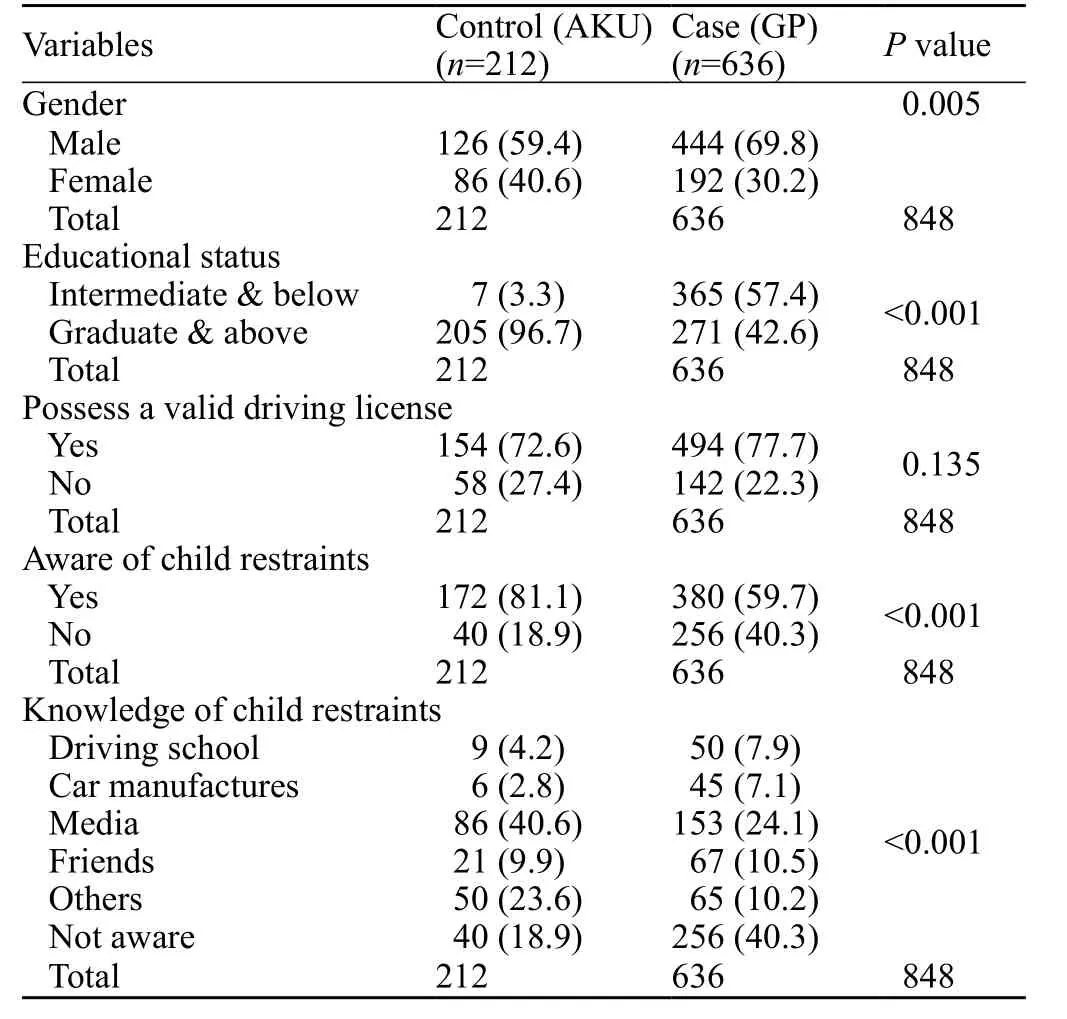
Table 1. Demography and awareness about CR, n (%)
Comparison of CR usage
When questioned about the availability of CR in their cars, 30.7% of the participants from AKU compared to 9.9% of those from the GP answered in the affirmative(P<0.001). However, there was no significant difference in the functional status of CR between the two groups(AKU 95.4% vs. GP 90.5%) (Table 2).
Table 2 describes the types of CRs. Interestingly,out of the participants who possessed a working CR, we found that 75.4% of those from AKU compared to 90%from the GP group were actually using it (P<0.001).The frequency of CR usage was also found to be higher(61.3%) in the GP group compared to AKU where it was reported to be 51.7%. A statistically significant difference was found between the two groups when inquired about who took care of the child while driving (P<0.001).26.4% of children of drivers from the AKU group left their children unattended while restrained, while a significantly higher number (89.8%) of those from the GP stated that they left their children unattended while retrained.
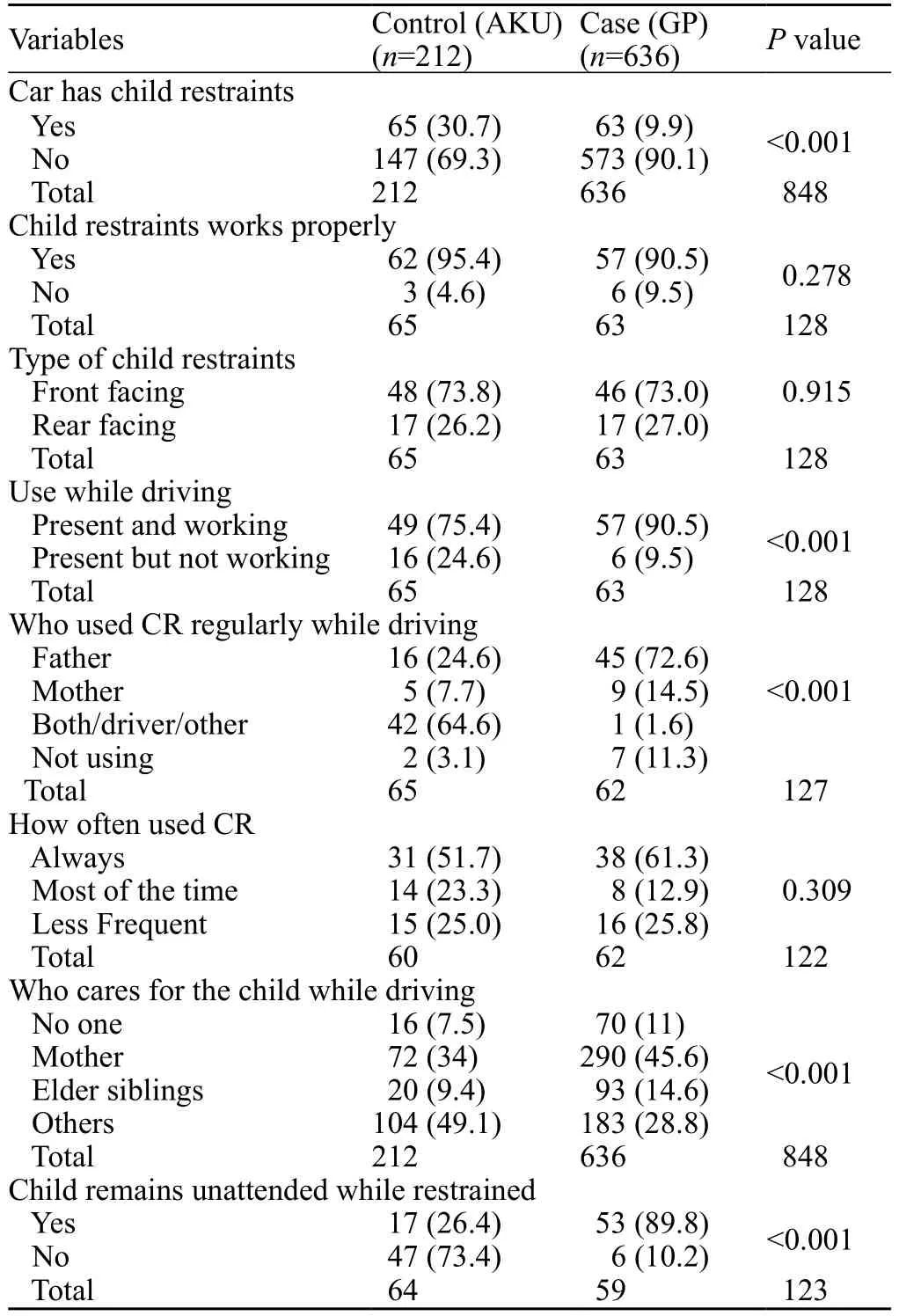
Table 2. Availability of child restraints, n (%)
Table 3 summarizes information regarding availability and use of seatbelts as well as the type of seatbelts and the usual speed limit while driving. With respect to availability of functional seat belts, AKU car users fared better than those from the GP. 72.2% of the AKU group claimed to have this facility in their cars as opposed to 30.7% from the GP (Pvalue <0.001). However, when questioned about regular usage, only 17.7% of those from AKU compared with 38.8% of those from the GP answered in the affirmative while 43.6% from the AKU group and 25.8% from the GP reported that they did not use seatbelts regularly (P<0.001). Types of seat belts and speed limits are further elaborated in Table 3.
Attitudes of participants about accident and driving attitude by AKU and GP group
Table 4 sheds light on the number of car accidents amongst the people of the two groups and the attitudes of the participants towards the use of CR and seatbelts as well as the reasons for not using them. We found a similar proportion of car accidents in the two groups(P=0.114). The driver involved in majority of the car accidents among the AKU population was the mother(50.8%) compared with the GP where the fathers were involved in most of the accidents (83.9%) (P<0.001).About 62.3% and 48.9% of the drivers from AKU and GP were belted at the time of the accident. There was a significant difference between the two groups in terms of use of child restraint at the time of the accident which was reported to be 66.7% in the AKU drivers and 11.1%in the GP (P=0.015). It is interesting to note that only 23.7% of those from AKU and 2.1% of those from the GP realized the importance of child restraint and started using it after the accidents (P<0.001). The most common reason for not using CR amongst the GP was not knowing how to use it (P=0.001).
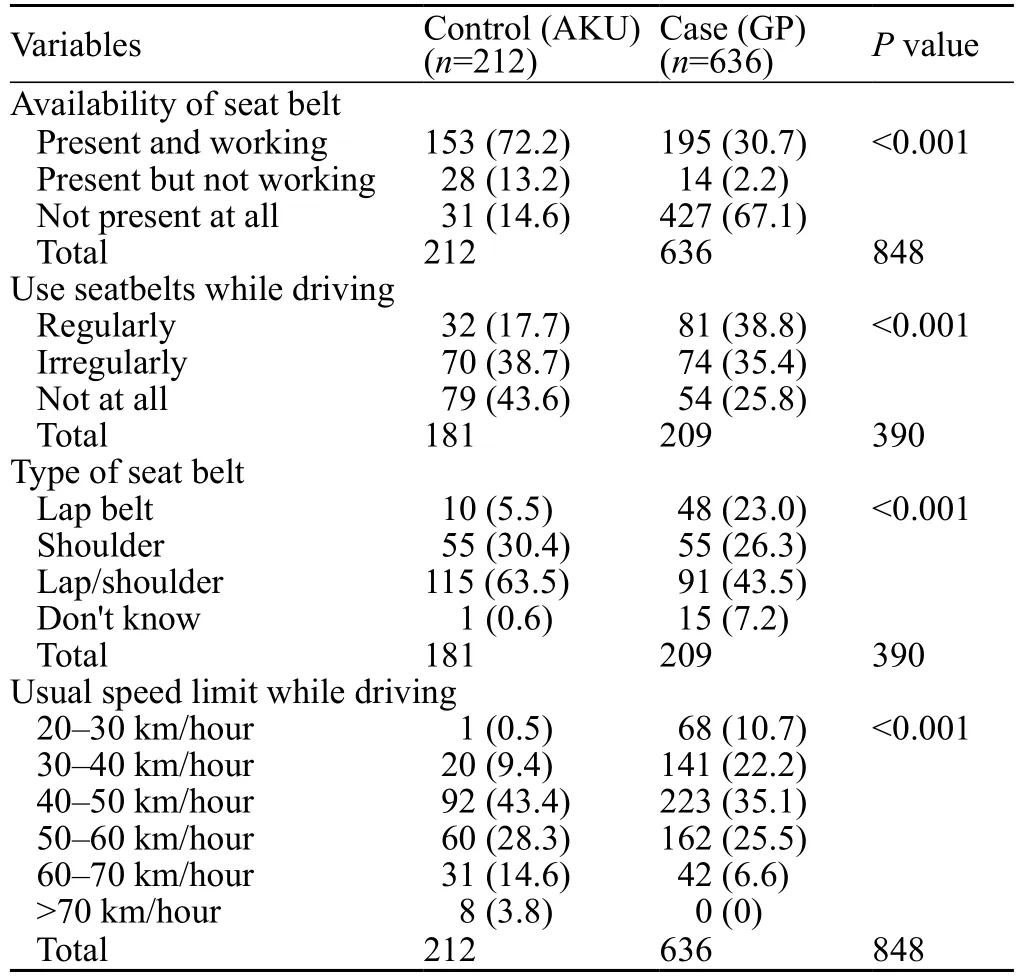
Table 3. Availability and use of seat belt, n (%)

Table 4. Car accident and driving attitude, n (%)

Table 5. Multivariate Logistic Regression Model based on outcome of presence of CR in car (n=128)
Multivariate logistic regression model
Table 5 describes the multivariate logistic regression analysis which shows the impact of various factors on the presence of child restraint in cars. Availability of child restraint was found in 128 (15.1%) of car users, and different covariates examined independently using the univariate analysis. Education level and type of user were both found to be associated with availability of child restraint (P<0.05). Likewise, three other variables, which included gender of the driver, frequency of commuting and use of sticker of 'child on board' had a significant association with presence of child restraint (P<0.10).
Interestingly, with multivariate analysis, some of the variables that showed significant associations with the bivariate model were no longer significant after controlling for the effect of other variables.
The main predictor, i.e. type of car user showed a significant association with the outcome using the multivariate analysis (OR4.20 with 95%CI2.43–7.26),establishing the fact that the odds of having child restraint in cars was 4.2 times higher in the control group as compared to those who were in the general population.Car users who regularly used the highways were 1.83 times more likely to have child restraint in their cars than those who did not (OR1.83 with 95%CI1.09–3.07).
Similarly, the car users who possessed a driving license had greater odds of having child restraint in their cars compared to those without a driving license(OR2.05 with 95%CI1.0– 4.18). The number of people who used 'child on board' stickers were also found to be significantly associated with child restraint availability(OR2.46 with 95%CI1.0–6.10) (Table 5).
DISCUSSION
This study is in continuation of a similar study published in the recent past, in which we assessed the attitude of the educated population towards child restraint(CR) and seat belt usage,[18]and the findings of the study were not generalizable to the entire population. However,in this study we included participants from a mixed educational, cultural and socioeconomic stratum so that their attitudes towards CR and the reasons for not using them could be clearly understood and compared. This not only allows a fair comparison but also makes our findings easy to generalize to the entire population of the country.
We did not find an association between the level of educational and driving license possession. The study also demonstrated that the educated population was not just more aware but also had working seat belts (P<0.001) and child restraints (P<0.001) to a significantly greater degree than the cases and this shows the importance of the principles of 3 E's for road safety, Engineering, Education and Enforcement. All E's are included in SB and CR usage.[19]This was similar to previously published literature.[20]
Though a large number of drivers did not have a valid driving license, its validity had no correlation with CR use. In a similar study by Trevino-Siller et al,[21]it was found that educated participants from both groups had a higher utilization rate and higher availability of CR and SB. Media plays an important role in attaining knowledge of CR. Difficulty of use or not knowing how to use CR were the two most common reasons for not using CR.
Drivers across the world have to follow certain driving rules which include proper use of seat belts and CR. Not being belted properly is considered an offense in most parts of the world.[22]
Media was identified as the largest source of information about child restraint in both groups. This highlights the need for more awareness campaigns on the importance of child restraint through the media. Driving schools and car manufacturers were shown to have the least contribution in providing awareness about CR use. This stems from the fact that in Pakistan, there is a dearth of standardized driving institutes that provide proper training to drivers.Lack of awareness and enforcement of traffic laws in the country also contributes to the inadequate use of safety equipment in motor vehicles. Car manufacturers only introduced rear adult seat belts and buckling sockets for CR in cars in the last decade. Thus, it is not surprising that the use of CR in the country is still limited and knowledge about its use is least likely to come from car manufacturers.
The most common reason for not using CR was discomfort similar to a prior study.[13]The reasons however were significantly different for drivers from the control group who stated that the reason for not using CR was not knowing how to use it or finding it too expensive.This emphasizes the need to not just make the masses aware of the importance of child restraints in MVs but also teaching them how to do so. As far as the cost of CR in Pakistan is concerned, it comes to about $150–200 which is considered quite expensive by most people.Efforts should be made to cut down on the cost to make the use of CR more widespread in the country. As far as the rules and regulation of Federal Vehicle Safety Standards in Pakistan, there are some strict rules to follow for highways as mention in item # 36–38, which clearly delineate the use of CR seat belts, however the local data is deficient in describing the exact number of CR user and their reason of not using it.[23]
CONCLUSION
Injuries not only cause financial loss to the family but also have a tremendous burden on society economic resources. Pediatric injuries may shatter psychological and emotional relationships, often destroying families with a long lasting impact on the family.[24]
This would be driver's responsibility to use seat belt and CR seat belts, however availability and training part is the responsibility of vehicle manufactures and the motor vehicle safety regulation department. Therefore, following the road safety rules is an essential step in securing the safety of the child and other passenger.
For Love, Buckle campaign may change behavior and attitudes towards child safety on the road. Advocating for the implementation and enforcement of the seat-belt and child restraint law is just as essential as educating parents and providing guidance on effective seat-belt enforcement. A legal system working towards implementing these strategies will hopefully prevent child injuries on the road in the future.
Funding: None.
Ethical approval: This study was approved by the ethical committee of Aga Khan University Hospital, Karachi, Pakistan.
Conflicts of interest: Each author of this manuscript does not have any conflict of interest.
Contributors: EUS conceptualized the idea and critically reviewed the draft. BA contributed to the literature search and reviewed the document. GK contributed to the literature search and reviewed the document. AF cleaned and performed all statistical analysis of the data, developed tables and graphs. RN critically reviewed and modified the manuscript as submitted. TM contributed to the literature search, analyzed and interpreted the data and wrote the final draft of the manuscript. AA contributed to the literature search, analysed and interpreted the data, wrote the first draft of the discussion section and edited the manuscript. SS helped in writing the manuscript. ZS helped in writing the manuscript. This manuscript has been read and approved by all the authors and each author believes that the manuscript represents honest work.
1 Forjuoh SN, Gyebi-Ofosu E. Injury surveillance: should it be a concern to developing countries? J Public Health Policy. 1993;14(3):355–9.
2 WHO. Health statistics and health information systems–Projections of mortality and burden of disease to 2030 Geneva2006.Available from: http:// www. int/ healthinfo/ statistics/bodprojections20.
3 Vital Statistics, Mortality: summary list of causes. Ottawa,Canada: 1978.
4 Ma X, Layde P, Zhu S. Association between child restraint systems use and injury in motor vehicle crashes. Acad Emerg Med. 2012;19(8):916–23.
5 Mohan D, Bawa P. An analysis of road traffic fatalities in Delhi,India. Accid Anal Prev. 1985;17(1):33–45.
6 Manciaux M, Romer CJ. Accidents in children, adolescents and young adults: a major public health problem. World Health Stat Q. 1986;39(3):227–31.
7 Hertz E. Revised estimates of child restraint effectiveness.NHTSA Research Note. 1996.
8 Rice TM, Anderson CL. The effectiveness of child restraint systems for children aged 3 years or younger during motor vehicle collisions: 1996 to 2005. Am J Public Health. 2009;99(2):252–7.
9 Berg MD, Cook L, Corneli HM, Vernon DD, Dean JM. Effect of seating position and restraint use on injuries to children in motor vehicle crashes. Pediatrics. 2000;105(4):831–5.
10 Elliott MR, Kallan MJ, Durbin DR, Winston FK. Effectiveness of child safety seats vs seat belts in reducing risk for death in children in passenger vehicle crashes. Arch Pediatr Adolesc Med.2006;160(6):617–21.
11 Snowdon AW, Hussein A, Ahmed E, Kolga C, Howard A.Technical Report: Canadian National Survey on Child Restraint use 2010 Completed for Transport Canada, in partnership with AUTO21.
12 Pérez-Núñez R, Chandran A, Híjar M, Celis A, Carmona-Lozano MS, Lunnen JC, et al. The use of seatbelts and child restraints in three Mexican cities. Int J Inj Contr Saf Promot. 2013;20(4):385–93.
13 Williams AF. Observed child restraint use in automobiles. Inj Prev. 1998;4(2):155–60.
14 Wikipedia, the free encyclopedia: List of countries by vehicles per capita. 2016.
15 WHO. Pakistan Statistics Summary. Global Health Observatory Data Repository 2012.
16 Pakistan Bureau of statistics - Government of Pakistan: Pakistan Statistical Year Book 2011 2011. Available from: http://www.pbs.gov.pk/content/pakistan-statistical-year-book-2011.
17 Razzak JA, Luby S, Laflamme L, Chotani H. Injuries among children in Karachi, Pakistan—what, where and how. Public Health. 2004;118(2):114–20.
18 Siddiqui E, Ejaz K, Waheed S, Kazi GI, Khursheed M. Attitudes towards child restrains and seat belts usage in the learned population of Karachi, Pakistan. World J Emerg Med. 2014;5(3):223.
19 Peden M, Scurfield R, Sleet D, Mohan D, Hyder AA, Jarawan E, et al. World report on road traffic injury prevention. World Health Organization Geneva; 2004.
20 Hassan HM, Abdel-Aty MA. Exploring the safety implications of young drivers' behavior, attitudes and perceptions. Accid Anal Prev. 2013;50:361–70.
21 Trevino-Siller S, Pacheco-Magana LE, Bonilla-Fernandez P,Rueda-Neria C, Arenas-Monreal L. An educational intervention in road safety among children and teenagers in Mexico. Traffic Inj Prev. 2016:1–7.
22 Handbook TDs. Your Road Safety Responsibilities South Australia: My Licence; 2016. Available from: http://mylicence.sa.gov.au/data/assets/pdf_file/0009/152874/MR200_p1-40_Mar_2016_v1.pdf.
23 National Highway & Motorway Police Pakistan Rules.downloaded on May 10, 2017 https://headfastco.wordpress.com/2011/03/24/national-highway-motorway-police-pakistan-rules
24 Ghaffar A, Hyder AA, Mastoor MI, Shaikh I. Injuries in Pakistan: directions for future health policy. Health Policy Plan.1999;14(1):11–7.
Emad Siddiqui, Email: emaduddin.siddiqui@aku.edu; emaduz@yahoo.com
BACKGROUND:Motor vehicle crash (MVC) related injury has been identified as a major public health concern. Child restrain (CR) seat belts can minimize the mortality and morbidity from MVC.The use for seat belts is substantially low in developing countries like Pakistan even though its use has been shown to decrease morbidity and mortality by a significant extent.
METHODS:This was a case control study with cases from the general population (GP) and controls from the Aga Khan University (AKU) employees in a 3:1 ratio. The study questionnaire was based on parameters like gender, education level, awareness and presence of CR and also assessed the frequency of usage, reasons for not using CR and the source of knowledge regarding CR use.
RESULTS:Out of 848 respondents, 212 were from AKU and 636 were from the GP. 96.7% from AKU had at least a bachelor's degree while less than half (42.6%) of those from the GP were graduate or above (P<0.001). A statistically significant difference was found between the two groups with drivers from AKU being generally more aware about CR and its use. 81.1% of the group from AKU compared to 59.7% from the general population were found to be aware of child restraint use (P<0.001). Media(40.6%) was found to be the most common source of information amongst the AKU employees.
CONCLUSION:Most motor vehicle related injuries in children can be prevented or their severity may be reduced by the use of appropriate child restraint seat belts.
World J Emerg Med 2017;8(4):269–275
10.5847/wjem.j.1920–8642.2017.04.004
March 10, 2017
Accepted after revision August 15, 2017
 World journal of emergency medicine2017年4期
World journal of emergency medicine2017年4期
- World journal of emergency medicine的其它文章
- Procedural simulation: medical student preference and value of three task trainers for ultrasound guided regional anesthesia
- Instructions for Authors
- Evaluation of a point of care ultrasound curriculum for Indonesian physicians taught by first-year medical students
- Education in cardiopulmonary resuscitation in Russia:A systematic review of the available evidence
- Rehabilitation of vulnerable groups in emergencies and disasters: A systematic review
- Paediatric-appropriate facilities in emergency departments of community hospitals in Ontario:A cross-sectional study