
Education in cardiopulmonary resuscitation in Russia:A systematic review of the available evidence
2017-12-15 09:08AlexeiBirkunMaksimGlotov
Alexei Birkun, Maksim Glotov
Department of Anaesthesiology, Resuscitation and Emergency Medicine, Medical Academy named after S. I. Georgievsky of V. I. Vernadsky Crimean Federal University, Simferopol 295051, Russian Federation
Review Article
Education in cardiopulmonary resuscitation in Russia:A systematic review of the available evidence
Alexei Birkun, Maksim Glotov
Department of Anaesthesiology, Resuscitation and Emergency Medicine, Medical Academy named after S. I. Georgievsky of V. I. Vernadsky Crimean Federal University, Simferopol 295051, Russian Federation
Cardiac arrest; Cardiopulmonary resuscitation; Education; Training; Russia
INTRODUCTION
Being the largest country in the world by surface area, the Russian Federation has a population of over 143 million people.[1]Globally, this country holds one of the leading positions in cardiovascular mortality (1 462 deaths per 100 000 inhabitants a year), and about 200 000–250 000 people die each year following sudden cardiac arrest.[2]A recent study showed an incidence rate of out of hospital cardiac arrest with attempted cardiopulmonary resuscitation (CPR) to be 58 per 100 000 population, with only 27% cases where resuscitation was initiated by a bystander.[3]High incidence of cardiac arrest and low prevalence of bystander CPR emphasize urgent demand in improving both rate and efficiency of resuscitation efforts.
It is currently recognized that optimal survival rate from cardiac arrest is dependent on high-quality science,well-functioning chain of survival and CPR education.[4]In order to improve poor acquisition and retention of CPR skills,[5–7]existing teaching strategies should be evaluated by identifying and reviewing national scientific data on resuscitation education.
So far, there is no integrated nationwide system of CPR education, nor the unified standards for CPR curriculum and training in the Russian Federation.[8]Compulsory CPR training is currently provided to healthcare students,medical professionals and employees of emergency services (i.e. firefighters, rescuers, police officers), whereas educational opportunities for the population are basically limited to mandatory CPR training during driver's license acquisition and occasional CPR courses.[8–10]At the same time, published information on CPR education in Russia seems to be scarce and scattered, limiting an opportunity to draw firm conclusions on the problem.
The objective of this study was to systematically review, summarise and appraise cumulative published scientific evidence relevant to CPR education in Russia.
METHODS
Protocol and registration
We have performed a systematic review of published experimental and nonexperimental studies pertaining to scientific research in the field of CPR education in Russia. The review was carried out in accordance with PRISMA statement and conducted following a pre-defined protocol.[11]The review protocol was not preregistered or published.
Eligibility
All studies pertaining to the field of CPR education published after 1991 (year of formation of the Russian Federation) were eligible for inclusion, if they (1)examined resuscitation training or existing CPR knowledge/skills in healthcare professionals or nonmedical individuals; (2) were initiated and executed by Russian researchers/institutions, and/or (3) investigated the topic of interest for Russia/Russian population. There was no limitation based on publication language or study design. Studies published as abstracts or dissertations/theses were considered as eligible along with original articles. Review articles, expert opinion, commentary,correspondence and editorials were excluded. However bibliographies of review articles were thoroughly screened to identify potentially relevant studies.
Search strategy
We have conducted a search in Medline, Scopus,Science Direct and Russian Science Citation Index (RSCI)from December 1991 to December 2016. Where applicable,initially selected free text search terms were supplemented with database-specific MeSH or MeSH-like terms relevant to the concepts of CPR and cardiac arrest. The CPR and cardiac arrest terms were all combined with Boolean "OR".The resulting set of terms was then combined with country/language terms "Russia" or "Russian" with Boolean "AND".In addition to the electronic database search, reference lists of included publications and contents pages of relevant Russian journals available online [Anesteziologiia i reanimatologiia(2003–2016), General reanimatology (2005–2016),Messenger of anesthesiology and resuscitation (2009–2016), Intensive care herald (2002–2016)] were manually searched for potentially relevant studies. Google Scholar was used for grey literature searching.
Study selection
The list of citations from relevant sources was generated using Zotero 4.0 (Roy Rosenzweig Center for History and New Media, USA). Following duplicate removal, title,abstract, key words and author affiliation were initially screened for relevance by both reviewers, and obviously irrelevant publications were excluded. Then, full manuscripts were obtained for all potentially relevant studies, and reviewed for eligibility independently in an unblinded standardized manner by two reviewers with disagreements concerning inclusion decisions resolved by consensus. The study selection diagram is presented in Figure 1.
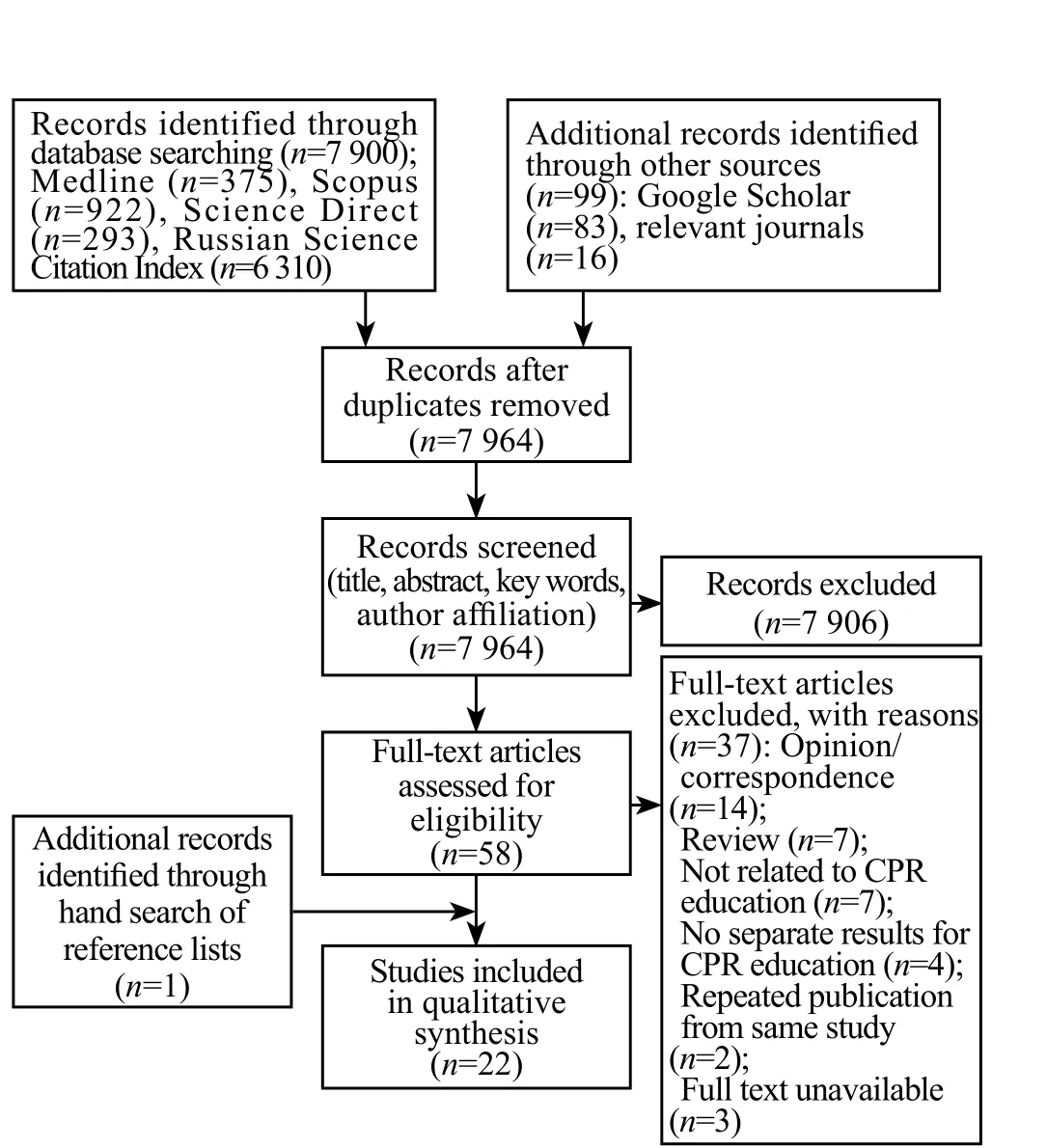
Figure 1. Flow diagram of the study selection process.
Data extraction
For all eligible studies, the following information was extracted and tabulated by one reviewer and checked by second reviewer: authors, publication year, publication type, language, study type, aim and objectives, population,number of participants, educational intervention, study methods and measures, main findings, and quality of the study. Any disagreements between reviewers were resolved through discussion.
Quality appraisal
The methodological quality was assessed independently by two reviewers using the Mixed Methods Appraisal Tool(MMAT) – Version 2011.[12]This tool allows for concomitant appraisal of studies employing different methodologies(qualitative, quantitative and mixed methods studies). Each study was initially assessed by two screening questions to determine the feasibility of further appraisal. If positive, the study was categorized within its methodological domain using the MMAT scoring metrics descriptors to produce overall quality score varying from 25% (* – one criterion met) to 100%(**** – all criteria met). Any disagreements were settled by consensus. No studies were excluded based on the low quality.
Data synthesis
The heterogeneity of research designs, educational interventions and outcome measures prevented data synthesis using meta-analysis, and results are described in a narrative synthesis.
RESULTS
Study selection
Initial search provided 7 999 citations, of which 7 964 were unique. The majority of these (7 906) were excluded during the process of relevance screening. Fifty eight were considered as relevant based on the title, abstract,key words and/or author affiliation, and included in the eligibility assessment. After reviewing the full papers,37 were excluded. One additional study was identified through a hand search of reference lists of potentially eligible articles. Consequently, 22 studies were included in the final analysis. A flow diagram of the study selection process is presented in Figure 1.
It is worthy of note that the majority of initial search citations (79%) came from the RSCI database, eventually yielding only 24 potentially eligible articles, thus suggesting low sensitivity of the database search.
Study characteristics
Of the 22 publications included in the review, there were 11 full-text articles, 10 conference abstracts and 1 dissertation. The majority of the studies were published in the Russian language (91%). One publication was in English (conference abstract), and one full-text article was bilingual (Russian/English). Distribution of the publications over the 25-year period (1991–2016) is shown in Figure 2.
Table 1 shows the percentage distribution of investigated populations. Healthcare professionals and medical students represent the most commonly studied population categories (63% and 20% study populations,respectively). Non-medical individuals constituted 17% of the investigated populations. This category was represented by first aid instructors (2 studies), cadets of the fire and rescue service academy (2 studies) and pedestrians/drivers (1 study). Sample size ranged from 26 to 2 000 participants, and was not reported in 4 studies.
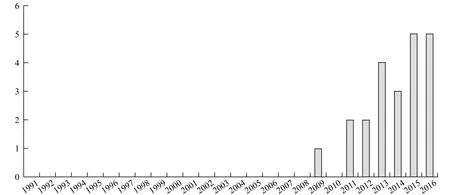
Figure 2. Distribution of the publications per year.
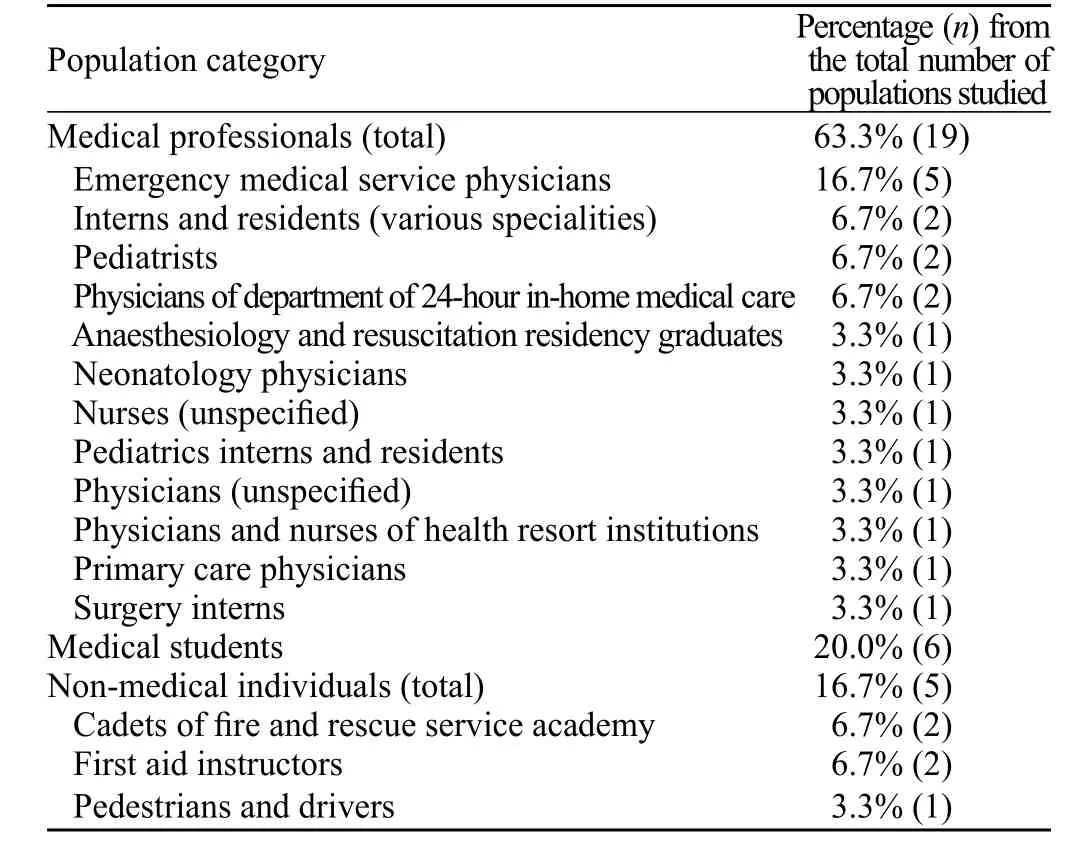
Table 1. Percentage distribution of populations studied
Three of the included studies were quantitative randomized controlled, one – qualitative, ten – quantitative non-randomized and the remainder (n=8) were quantitative descriptive studies in terms of the MMAT assessment.The overall quality score indicated low (quality score –25%;n=1), moderate low (50%;n=3) and moderate high(75%;n=2) methodological quality of full-text articles;low (n=1) and moderate low (n=5) quality of conference abstracts; and moderate low quality of dissertation. Nine studies failed to pass the quality screening.
Synthesis of results
All studies included in the review were grouped into the following thematic categories: (1) studies assessing effects of CPR educational intervention; (2) studies assessing only existing CPR skills and/or theoretical knowledge; (3) other studies, which did not fall into the categories above.
Studies assessing effects of CPR educational intervention
Fourteen (64%) out of 22 publications eligible for the review, including 7 full-text articles,[13–19]6 conference abstracts[10,20–24]and 1 dissertation,[25]describe effects of various educational interventions aimed to improve CPR theoretical knowledge and/or skills. Three studies were randomized controlled,[10,24,25]9– quantitative nonrandomized,[13,14,16,17,19–23]1– quantitative descriptive,[18]1–qualitative.[15]
Study participants included emergency medical service physicians,[13–16,25]physicians of other specialities,[16,17,20–22,25]interns/residents,[18,19,23,25]medical students,[19,25]nurses[22]and cadets of the fire and rescue service academy.[10,24]Sample size varied from 26[13]to 621.[25]
Basic life support (BLS) teaching was provided in 11 studies,[10,13,16,18–25]advanced life support (ALS) in 3 studies.[15,17,25]The type of CPR algorithm taught (BLS or ALS) was not clear for one study.[14]There was only one study describing the use of an automated external defibrillator (AED) as a component of the educational program.[18]
Information on the structure of the educational intervention has been provided in 10 publications.[10,15–19,21,23–25]Most commonly, CPR education comprised a theoretical part (lecture) followed by a session of skill training.[16–19,21,25]Bazanov et al[24]compared 5 different forms of education:(1) theoretical training using lecture, text and photo slides; (2) lecture and training videos; (3) interactive program with graphical presentations and videos; (4)lecture and skills demonstration on manikins; and (5)self-education using hard copy of CPR guidelines.Another study carried out by the same group of authors examined effects of theoretical CPR training using multimedia presentations.[10]The duration of educational interventions was indicated in 7 publications, ranging from 2 to 72 hours.[10,15,17,18,21,22,24]
The efficiency of CPR education was evaluated based on the trainee's practical skills alone in 5 studies,[13,14,17,20,23]based only on theoretical knowledge in 4 studies,[10,19,22,24]and based on a combination of theoretical knowledge and practical skills in 3 studies.[16,21,25]An evaluation criteria for practical skills assessment were typically represented by the characteristics of separate CPR algorithm components,[13,14,16,17,20–23]in many cases – not more than chest compression, airway opening and/or ventilation parameters.[13,14,16,20,23]There was only one study providing integrated skills assessment, ensuring a complete coverage of basic and advanced CPR algorithms.[25]
CPR knowledge and/or skills improvement following the education has been shown in 9 studies.[10,13–17,20,21,24]Two studies investigated trainee's opinion on completed educational interventions.[15,18]Three publications presented results on optimal retraining interval.[10,22,25]
Six (43%) of the 14 studies from this thematic category failed to pass MMAT quality screening for the following reasons: no clear research questions (objectives)defined,[14,16,18]collected data do not allow to address the research question (objective).[17,20,23]
All three studies declared as randomized have passed the quality screening, and their overall MMAT quality scores were 50% (moderate low quality)[24,25]and 25%(low quality).[10]The corresponding publications did not provide any information on the randomization procedure,allocation concealment or blinding.[10,24,25]Additionally,there was no description of the evaluation criteria for the assessment of the efficiency of education in two studies.[10,24]
The only qualitative study had an overall MMAT score of 50%.[15]Moderate low quality of the study results from the lack of information on the qualitative data analysis process and no consideration given to how the obtained findings relate to the potential researchers'influence through their interactions with participants.[15]
The non-randomized quantitative studies were of moderate low[13,21,22]and moderate high quality.[19]Based on MMAT appraisal, the methodological flaws of these studies were related to the study sample recruitment,[13,21,22]evaluation criteria/measurements utilized,[19,21]differences between groups being compared,[22]and completeness of the outcome data presented.[13]
Further, it is important to point out the following serious quality defects of the publications from this thematic category: three papers are missing sufficient information on the structure and content of educational intervention,[14,20,22]two publications contain no wordings of study aims or objectives,[14,16]and three papers have no data on sample size.[14,16,20]
Studies assessing existing CPR skills and/or theoretical knowledge
Five (23%) out of 22 publications included in the review– 3 full-text articles[26–28]and 2 conference abstracts,[29,30]describe the studies evaluating existing CPR skills and/or theoretical knowledge. All studies were quantitative descriptive. Four of them examined CPR theoretical knowledge using questionnaire survey,[26,27,29,30]and one study assessed BLS practical skills by means of the objective structured clinical examination.[28]
Study populations were represented by anaesthesiology and resuscitation residency graduates,[28]medical students,[26,27,29]as well as pedestrians and drivers.[30]Sample size varied from 200[30]to 2000.[26,27,29]It is worthy of note that three studies were carried out on the same population of medical students.[26,27,29]However,considering the different study aims and results presented in these publications, all three studies were included in the analysis independent of each other.
Notably, for all studies assessing theoretical knowledge, the evaluation criteria and, thus, study results were answering to the study aim only partially.[26,27,29,30]For example, Churkina et al[29]used the single evaluation criterion "correct hand position for chest compressions",when the study aim was "to assess the medical student's knowledge of CPR provision".
Two of 5 studies from this thematic category failed to pass quality screening.[27,29]For one study, the collected data do not allow to address the research questions.[29]For another study, further quality appraisal was considered to be unfeasible as a result of special circumstances not covered by the MMAT screening questions: the correct answers to the multiple-choice questions in the questionnaire were based on fundamentally erroneous statements.[27]In particular, the statement reading"artificial lung ventilation is prohibited in case of cervical spine fracture" is regarded as a correct answer to the question of contraindications for artificial ventilation.[27]
For the studies which passed the screening, the overall quality was determined to be low,[28]moderate low[30]and moderate high.[26]According to the MMAT assessment, the methodological limitations of these studies were related to the following: relevance of the sampling strategy to address the research question,[28,30]representativeness of the sample for the population under study,[28,30]appropriateness of the measurements utilized,[26]and the acceptable response rate.[28]Additionally, the sample size data were lacking for one study.[28]
Other studies
The conference abstract by Moroz et al[9]describes the results of the quantitative descriptive study aimed to analyze the real-life efficacy of the European Resuscitation Council BLS/AED courses in Russia. The study was carried out using online questionnaire survey in the mixed population of medical doctors, nurses and first aid instructors who previously passed the training(n=126). Moderate low overall ММАТ quality score is attributable to the disadvantages pertaining to the sample representativeness and appropriateness of the evaluation criteria to address the research question. Presented results are answering the study aim partially, describing the statistics of CPR provision in real-life settings (incidence of CPR cases, extent of provided CPR, incidence of return of spontaneous circulation), but not assessing the efficiency of the courses directly.[9]
Il'icheva et al[31]conducted the questionnaire survey in order to investigate the demand in CPR knowledge and skills learning amongst students of the medical university.This study was carried out in the same population of medical students as in 3 studies assessing CPR theoretical knowledge described above.[26,27,29]Overall MMAT score of 50% is explained by the methodological flaws related to the relevance of sampling strategy to the study aim and sample representativeness for the population being investigated. For instance, it doesn't seem reasonable to pose a question on the need in increasing the amount of time dedicated to CPR theoretical learning to the 2nd year students, who had no previous CPR education at all.[31]
The quantitative non-randomized study by Bazanov[32]investigated the objectiveness of chest compression quality assessments done by first aid instructors. For this purpose,the results of first aid instructors' assessments were compared with chest compression parameters calculated by the computer program. When the author concludes about subjectiveness, low specificity, sensitivity and accuracy of the instructors' assessment, the publication contains no results to support the conclusion. For this reason, the publication has failed to pass the MMAT quality screening.[32]
DISCUSSION
To the best of our knowledge, this is the first systematic review summarising and appraising the cumulative published scientific evidence relevant to the CPR education in the Russian Federation.
For the period from 1991 to 2016, the search revealed 22 eligible studies pertaining to this area of resuscitation science. All of them were carried out by Russian researchers, and published mostly in Russian. With low overall quantity of the studies included in the review and complete lack of eligible publications for the period from 1991 to 2008, there is a general trend for increased number of studies by the year of 2016.
Methodologically, the most common types of studies were quantitative non-randomized (45%) and quantitative descriptive (36%). Randomized controlled studies represent less than 14% out of the total number of studies included in the review. There was one eligible qualitative study.
Healthcare professionals were predominant among the populations investigated. Most commonly, those study participants were physicians of various specialities,less often –interns/residents or nurses. Medical students constituted the second most frequently studied category of participants. However, it is of note that the same population was investigated in 4 of 6 eligible studies involving medical students.[26,27,29,31]Non-medical individuals were participating in the studies much less commonly, covering only three population categories:first aid instructors, cadets of the fire and rescue service academy and pedestrians/drivers.
In most instances the studies were evaluating effects of various educational interventions designed to improve theoretical knowledge and/or skills of BLS CPR not involving AED. Less frequently, existing CPR theoretical knowledge and/or skills were evaluated. Individual studies investigated the demand in CPR education, objectiveness of resuscitation skills assessments by instructors, real-life implementation of CPR algorithms after completion of the training. The studies were significantly heterogeneous with regards to methodological approaches, structure and duration of educational interventions, evaluation methods and criteria being used.
The results of the studies assessing effects of CPR educational interventions are generally suggestive of the beneficial influence of the training conducted. Alongside this, the assessments were usually based on a few evaluation criteria characterizing separate resuscitation algorithm components rather than providing integral assessment of the CPR performance.
The studies included in the review were mostly of low methodological quality. More than 40% of the publications have not passed the quality screening, particularly due to the absence of clear research questions or study objectives defined, or since the collected data do not allow to address the research questions. The overall quality, as assessed using the MMAT, was categorised as low or moderate low for 50% of the studies. Only 2 (9%) of 22 eligible studies met the criteria of moderate high quality.
None of the publications describing the randomized studies provided any details on the randomization procedure. Further, these papers contain no information on allocation concealment or blinding.
Methodological limitations of the quantitative nonrandomized and quantitative descriptive studies were most commonly related to the study sample recruitment(no explanation for inclusion and exclusion criteria, no sample size justification, questionable representativeness of the sample for the population under study) and the applicability of the evaluation criteria/measurements utilized (criteria/measurements are not clearly defined or inappropriate for answering the research question).
Additional serious quality defects of particular studies included the absence of any statements in regard to the study aims and objectives or sample size not indicated.
Low number, high heterogeneity and poor quality of the studies, as well as rare involvement of nonmedical populations and scant evidence of AED use are all suggesting the strategic need for developing and introducing a foundational nationwide regulatory system in order to ensure high quality science and effective CPR education of lay people and healthcare professionals in the Russian Federation.
Limitations
In addition to the international database search, we have searched the major Russian scientific database and archives of the relevant field-specific Russian journals available online. However, it cannot be ruled out that some potentially eligible publications may have been omitted due to limitations in the search strategy. In particular, it may concern those studies published in hard copy but not converted to the electronic form or indexed in the electronic databases.
CONCLUSIONS
The results of the systematic review suggest the paucity, low population coverage, high thematic and methodological heterogeneity and low quality of the studies addressing CPR education, which were carried out in the Russian Federation. There is a critical need in conducting methodologically consistent, large-scale,randomized, controlled studies evaluating and comparing the efficiency of educational interventions for teaching CPR in different population categories of Russia.
ACKNOWLEDGEMENTS
The authors would like to thank Dantanarayana Visith Risira for editing the text in English language.
Funding: This systematic review did not receive any funding.
Ethical approval: Not needed.
Conflicts of interest: The authors declare that they have no competing interests.
Contributors: AB determined the concept of the review and was a major contributor to the study design, article search, data collection,data analysis and manuscript production. MG assisted in data collection and analysis, in writing the manuscript and revising the article. All authors read and approved the final manuscript.
1 United Nations Department of Economic and Social Affairs.World Statistics Pocketbook 2016 edition. New York: United Nations; 2016: 251.
2 Bockeria OL, Biniashvili MB. Sudden cardiac death and ischemic heart disease. 2013;10(2):69–79.
3 Birkun AA, Glotov MA. Epidemiological features of out-ofhospital cardiac arrest: evidence from particular administrative centre in russian federation. Anesteziol Reanimatol.2017;62(2):113–7. Russian.
4 Finn JC, Bhanji F, Lockey A, Monsieurs K, Frengley R, Iwami T,et al. Education, Implementation, Teams Chapter Collaborators.Part 8: Education, implementation, and teams: 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations.Resuscitation. 2015;95:e203–24.
5 Chamberlain D, Smith A, Woollard M, Colquhoun M, Handley AJ, Leaves S, et al. Trials of teaching methods in basic life support (3): comparison of simulated CPR performance after first training and at 6 months, with a note on the value of re-training.Resuscitation. 2002;53(2):179–87.
6 Madden C. Undergraduate nursing students' acquisition and retention of CPR knowledge and skills. Nurse Educ Today. 2006;26(3):218–27.
7 de Ruijter PA, Biersteker HA, Biert J, van Goor H, Tan EC. Retention of first aid and basic life support skills in undergraduate medical students. Med Educ Online. 2014;19(1):24841.
8 Lysenko KI, Dezhurniy LI, Baturin DI, Tishkov EA. [Issues of first aid and resuscitation training in non-physicians]. Anesteziol Reanimatol. 2011;5:76–8. Russian.
9 Moroz V, Kuzovlev A, Gerasimov L, Borisov K. Analysis of efficacy of the European Resuscitation Council BLS/AED courses in Russia. Resuscitation. 2013;84:S22.
10 Bazanov SV, Potapenko LV, Sharabanova IYu. Speed of decay of cardiopulmonary resuscitation theoretical knowledge among nonmedical trainees. International journal of applied and fundamental research. 2016;2:367. Russian.
11 Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC,Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. Ann Intern Med. 2009;151(4):W65–94.
12 Pace R, Pluye P, Bartlett G, Macaulay AC, Salsberg J, Jagosh J, et al. Testing the reliability and efficiency of the pilot Mixed Methods Appraisal Tool (MMAT) for systematic mixed studies review. Int J Nurs Stud. 2012;49(1):47–53.
13 Mishina TP, Klimantsev SA, Bojko VO, Mysaeva ZI. Evaluation of efficacy of cardio-pulmonary resustitation provided by physicians from prehosptal ambulance teams. Skoraya Meditsinskaya Pomoshch. 2009;4:30–2. Russian.
14 Blokhin BM, Gavryutina IV. Simulation as the innovative method of training pediatric emergency. Medical Education And Professional Development. 2011;3:112. Russian.
15 Khubutia MSh, Timerbaev VKh, Valetova VV, Zvereva NYu,Plavunov NF, Baratashvili VL, et al. The first experience of simulation-based education of emergency care physicians on cardiac and pulmonary resuscitation. Pul'monologiia. 2011;2:119–23. Russian.
16 Troitzkaya NB, Blokhin BM, Gavryutina IV, Ovcharenko EYu,Steshin VYu. Simulative technologies for perfecting urgent medical aid to children. Kremlevskaya Meditsina. Klinicheskiy Vestnik. 2012;1:30–3. Russian.
17 Delaru NV, Mandrikov VB, Zayachnikova TE. Simulation technologies in postgraduate training of neonatologists in intensive care. Journal of VolgSMU. 2015;53(1):32–4. Russian.
18 Ligatyuk PV, Perepelitsa SA, Kuzovlev AN, Ligatyuk DD.Simulation training at a medical institute: an integral part of the educational process. General Reanimatology. 2015;11(1):64–71.
19 Taptygina EV, Myagkova EG, Gritzan AI, Gazenkampf AA,Khinovker VV, Ermakov EI. The standartization of teaching practical skills in medical university. Anesteziol Reanimatol.2016;61(4):257–60.
20 Blokhin BM, Gavryutina IV, Ovcharenko EYu, Smirnova YuV. Simulation education for cardiopulmonary resuscitation provision in children. Medical Education and Professional Development. 2012;3:117. Russian.
21 Gorban' VV, Korol'chuk IS, Burba LV, Filipchenko EM, Karuna YuV. Efficiency of implementation of simulation method"Cardiopulmonary resuscitation" on the postgraduate education stage. International Journal of Experimental Education. 2013;4:89–91. Russian.
22 Pasechnik IN, Skobelev EI, Krylov VV, Rybintsev VYu, Volkova NN. Cardiopulmonary resuscitation education in medical personnel of health resorts. Proceedings of the 15th symposium of Moscow scientific society of anesthesiology-resuscitation physicians; 2014 Mar 28; Golitsyno, Russian Federation. 2014:32–3. Russian.
23 Avramenko EA, Pavlova AI, Semenov SA, Vakhitov MSh,Shiganov MYu. Simulation training with video recording in acquiring the skills of cardiopulmonary resuscitation. Zdorov'eosnova chelovecheskogo potentsiala: problemy i puti ikh resheniya. 2015;2:535–6. Russian.
24 Bazanov SV, Sharabanova IYu, Potapenko LV. Comparative analysis of different cardiopulmonary resuscitation teaching methods. International Journal of Experimental Education. 2015;12:672–3. Russian.
25 Gavryutina IV. Simulation technologies as an instrument for optimization of emergency medical care provision to children[dissertation]. Moscow: Pirogov Russian National. Research Medical University; 2013. Russian.
26 Filatova AA, Chernyh MA, Churkina AS, Yakimec AA,Berseneva OV, Novikova VP, et al. Theoretical knowledge level of medical university students in CPR which were studied in different educational standards. Vestnik SMUS74. 2013;1:50–8.Russian.
27 Pirogova IA, Talanova VF, Chernyh MA, Vasil'eva TV,Nizamova VD, Vozhdaeva IV, et al. Investigation of specifics of artificial lung ventilation performance technique by higher medical educational institution students. SCI-ARTICLE.RU.2016;31:54–9. Russian.
28 Schegolev AV, Andreenko AA, Ershov EN, Lahin RE,Makarenko EP. Holding objective structured clinical examinations for anesthesiology and intensive care clinical residency in state graduates certification. Anesteziol Reanimatol.2016;61(1):71–4. Russian.
29 Churkina AS, Yakimets AA, Berseneva OV, Novikova VP,Samylov VV, Filatova AA, et al. Cardiopulmonary resuscitation:external cardiac massage as viewed by students. In: Artyukhov IP, Petrova MM, Vinnik YuS, Serova EV, Trukhin DV, editors.Proceedings of the 78th final students' research-to-practice conference with international participation dedicated to professor Yu. M. Lubenskiy 95th birthday anniversary; 2014 Apr 22–25;Krasnoyarsk, Russian Federation. Krasnoyarsk: KrasGMU;2014;716–7.
30 Mikhno VA, Kaurinа AV, Poroyskiy SV. Ready road users to first aid. International student scientific bulletin. 2015;2:180.Russian.
31 Il'icheva OE, Chukichev AV, Vozhdaeva IV, Peshikov OV.South Ural State Medical University students' opinion on the need to increase practical and theoretical studies to learn cardiopulmonary resuscitation. Optimization of higher medical and pharmaceutical education: quality management and innovations: Proceedings of the 2nd Russian nationwide research-to-practice conference dedicated to the Day of Russian science; 2014 Feb 7; Chelyabinsk, Russian Federation.Chelyabinsk: South Ural State Medical University; 2014:46–51.
32 Bazanov SV. Assessment of chest compression quality during cardiopulmonary resuscitation. International Journal of Experimental Education. 2016;5:193. Russian.
Alexei Birkun, Email: birkunalexei@gmail.com
BACKGROUND:To summarise and appraise cumulative published scientific evidence relevant to cardiopulmonary resuscitation (CPR) education in Russia.
DATA RESOURCES:We searched Medline, Scopus, Science Direct and Russian Science Citation Index databases from December 1991 to December 2016 to identify studies pertaining to the field of CPR education that were carried out by Russian researchers and/or investigated the topic of interest for Russia/Russian population. Reference lists of eligible publications, contents pages of relevant Russian journals and Google Scholar were also searched. There was no limitation based on publication language or study design.
RESULTS:Of 7 964 unique citations identified, 22 studies were included. All studies were published from 2009 to 2016, mainly in Russian. Only three studies were reported to be randomized controlled. Non-medical individuals constituted 17% of studied populations. Most of the studies aimed to assess effects of CPR educational interventions, generally suggesting positive influence of the training conducted. The studies were highly heterogeneous as for methodological approaches,structure and duration of educational interventions, evaluation methods and criteria being used.Methodological quality was generally poor, with >40% publications not passing quality screening and only 2 studies meeting the criteria of moderate high quality.
CONCLUSION:The results suggest paucity, low population coverage, high thematic and methodological heterogeneity and low quality of the studies addressing CPR education, which were carried out in the Russian Federation. There is a critical need in conducting methodologically consistent, large-scale, randomized, controlled studies evaluating and comparing efficiency of educational interventions for teaching CPR in different population categories of Russia.
World J Emerg Med 2017;8(4):245–252
10.5847/wjem.j.1920–8642.2017.04.001
April 26, 2017
Accepted after revision August 17, 2017
 World journal of emergency medicine2017年4期
World journal of emergency medicine2017年4期
- World journal of emergency medicine的其它文章
- Procedural simulation: medical student preference and value of three task trainers for ultrasound guided regional anesthesia
- Instructions for Authors
- Evaluation of a point of care ultrasound curriculum for Indonesian physicians taught by first-year medical students
- Rehabilitation of vulnerable groups in emergencies and disasters: A systematic review
- Paediatric-appropriate facilities in emergency departments of community hospitals in Ontario:A cross-sectional study
- Factors behind not using child restrain(t) among hospital employees and general population:A case control study