
Rehabilitation of vulnerable groups in emergencies and disasters: A systematic review
2017-12-15 09:08HojjatSheikhbardsiriMohammadYarmohammadianFatemehRezaeiMohammadRezaMaracy
Hojjat Sheikhbardsiri, Mohammad H. Yarmohammadian, Fatemeh Rezaei, Mohammad Reza Maracy
1 Department of Emergency Operation Center (EOC), Disasters and Emergencies Management Center, Kerman University of Medical Sciences, Kerman, Iran
2 Health Management and Economics Research Center, Faculty of Management and Medical Informatics, Isfahan University of Medical Sciences, Isfahan, Iran
3 Department of Epidemiology & Biostatistics, School of Public Health, Isfahan University of Medical Sciences, Isfahan, Iran
Review Article
Rehabilitation of vulnerable groups in emergencies and disasters: A systematic review
Hojjat Sheikhbardsiri1, Mohammad H. Yarmohammadian2, Fatemeh Rezaei2, Mohammad Reza Maracy3
1Department of Emergency Operation Center (EOC), Disasters and Emergencies Management Center, Kerman University of Medical Sciences, Kerman, Iran
2Health Management and Economics Research Center, Faculty of Management and Medical Informatics, Isfahan University of Medical Sciences, Isfahan, Iran
3Department of Epidemiology & Biostatistics, School of Public Health, Isfahan University of Medical Sciences, Isfahan, Iran
Rehabilitation; Vulnerable group; Emergencies; Disasters
INTRODUCTION
World Health Organization (WHO) defines disasters as a situation that causes inconsistency in social or community performance resulting in extensive humanitarian, economic or environmental damages.[1]Disaster management consists of four phases including prevention and mitigation,preparedness, response and rehabilitation.[2]Rehabilitation is defined as performing health care with the goal of restoring, maintaining or improving routine life skills of individuals with disabilities caused due to disease,accidents or incidents.[3]In disaster situations categories of rehabilitation could be physical, psychological, social,spiritual, and economic.[4]
In general, women, children, elderly and disabled people are more vulnerable when compared with adult men, resulting in a lower capacity of adaptation and survival in emergencies and disasters.[5]National Disaster Response Force (NDRF) reported elderly, children and disable people and emphasized rehabilitation immediately after disasters.[6]When coping with disasters or emergencies conditions, vulnerable people can face several additional problems, which increase their risk for symptoms such as abrupt onset of intense fear, vertigo,insomnia or even psychoses. Therefore, it is necessary for authorities to establish psychological consult clinics to help with adaptation and encourage them to cope with these symptoms.[7]
After emergencies and disasters, the most important economic rehabilitation action will restore vulnerable groups and improve family's livelihoods.[8]Studies conducted years after occurrence of disasters typically show that the society's progress is affected at a largescale, but significant issues are often ignored in relation to vulnerable groups in society.[9]The aim of the study was to perform a systematic review of rehabilitation activities for vulnerable groups during emergencies and disasters, including economical, physical, spiritual,psychological and social activities. The results of the current study may help health field managers better implement standard rehabilitation plans for vulnerable groups.
METHODS
The present study was a systematic review of publications relating to rehabilitation of vulnerable groups in emergencies and disasters. The study performed based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.[10]
Search strategy
This study conducted during November 2015 reviewed published English papers in the field of vulnerable group's rehabilitation in emergencies and disasters. For this purpose, we studied database including ISI Web of Science, PubMed, Scopus, Science Direct,Ovid, ProQuest, Wiley and Google Scholar from January 1, 2000 to October 22, 2015. The search key words included "recovery", "rehabilitation", "reconstruction","transformation", "transition", "emergency", "disaster","crisis", "hazard", "catastrophe", "tragedy", "mass casualty incident", "women", "female", "children", "pediatric","disable", "handicap", "elder", "old" and "vulnerable".Using OR and AND, key words were combined and written in search box of databases included [(recovery OR rehabilitation OR reconstruction OR transformation OR transition) AND (emergency OR disaster OR crisis OR hazard OR catastrophe OR tragedy OR mass casualty incident) AND (women OR female OR children OR pediatric OR disable OR handicap OR elder OR old OR vulnerable)]. All synonyms of the key words were included using MESH strategies.
Selection of articles and document
Independent reviewers (HS and FR) screened abstracts and titles for eligibility. When the reviewers felt that the abstract or title was potentially useful, full copies of the article were retrieved and considered for eligibility by both reviewers. If discrepancies occurred between reviewers, the reasons were identified and a final decision was made based on third reviewer (MM).Two authors (HS and MY) assessed the methodology quality and grade of evidence of included studies with the Critical Appraisal Skills Program (CASP) tools.[11,12]The CASP tools uses a systematic approach to appraise different study designs from the following domains:study validity, methodology quality, presentation of results, and external validity and each of the items from the checklists were judged with yes (low risk of bias,score 1), no (high risk of bias), or cannot tell (unclear or unknown risk of bias, score 0). Total scores were used to grade the methodologic quality of each study.[11,12]
Inclusion and exclusion criteria
We included papers that had at least one of the rehabilitation categories, at least one the vulnerable groups, and published paper in years of 2000 and after.
Database search
The initial electronic database search of the literature resulted in a total of 11 928 documents. At the next step,duplicated, books, dissertations, presentations were excluded and the number of documents decreased to 632 articles.Based on systematic screening, at the first stage we reviewed the titles and abstracts to find those related to rehabilitation of vulnerable groups in emergencies and disasters and we extracted 63 eligible articles. In the next step, all 63 selected full text papers were considered and finally 25 papers (6 qualitative, 16 cross-sectional and 3 randomized controlled trial studies) which reported rehabilitation of vulnerable groups in emergencies and disasters were selected. Figure 1 shows the search strategy and the selected articles in accordance with the PRISMA guidelines.[10]
Study quality assessment
Quality assessment of the included studies were done using the (CASP) tools.[11,12]The score of qualitative and quantitative studies ranged from 3 to 8 and 2 to 7 respectively. Studies did not report any rehabilitation programs duration after disasters. The majority of quantitative studies did not provide any ethical statement,study design, sampling and reflexivity related to research process. In the cross-sectional studies, only five out of sixteen articles[19,22,26,27,34]used appropriate methods.The majority of them also did not consider important confounding factors. None of the randomized controlled trial articles reported blinding of participants or assessors and two studies[35,36]lacked a control group. More details have shown in Table 1.
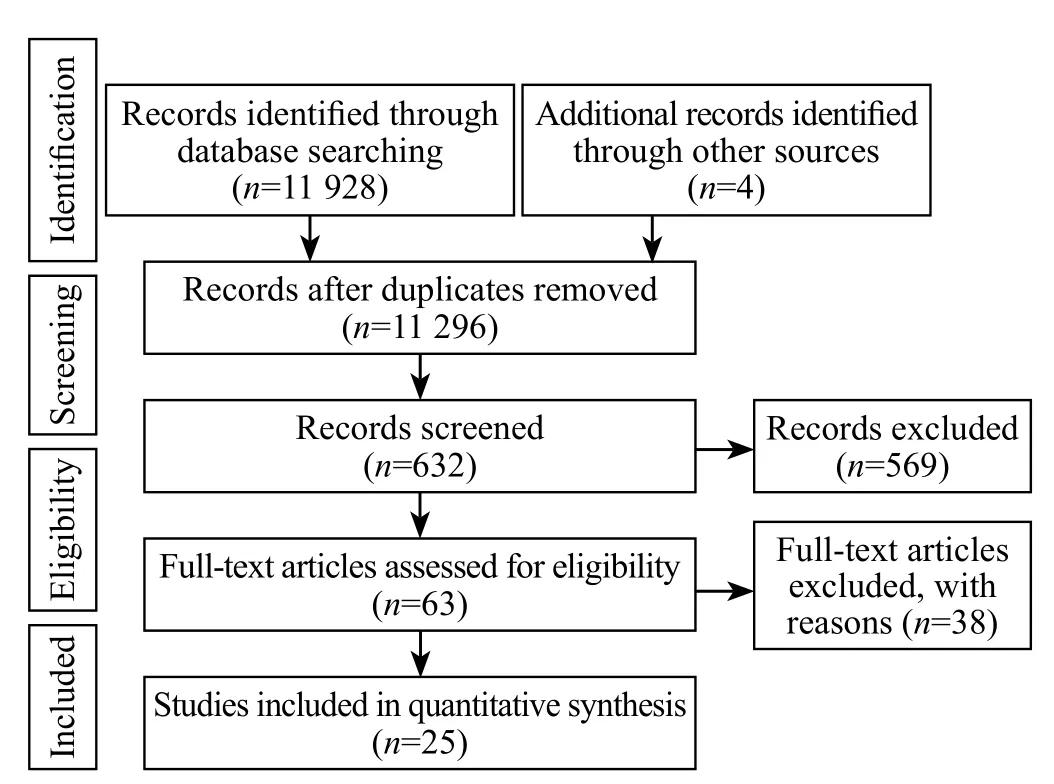
Figure 1. Flow diagram showing selection of articles reviewed, in accordance with the PRISMA Guidelines 10.
RESULTS
Demographics
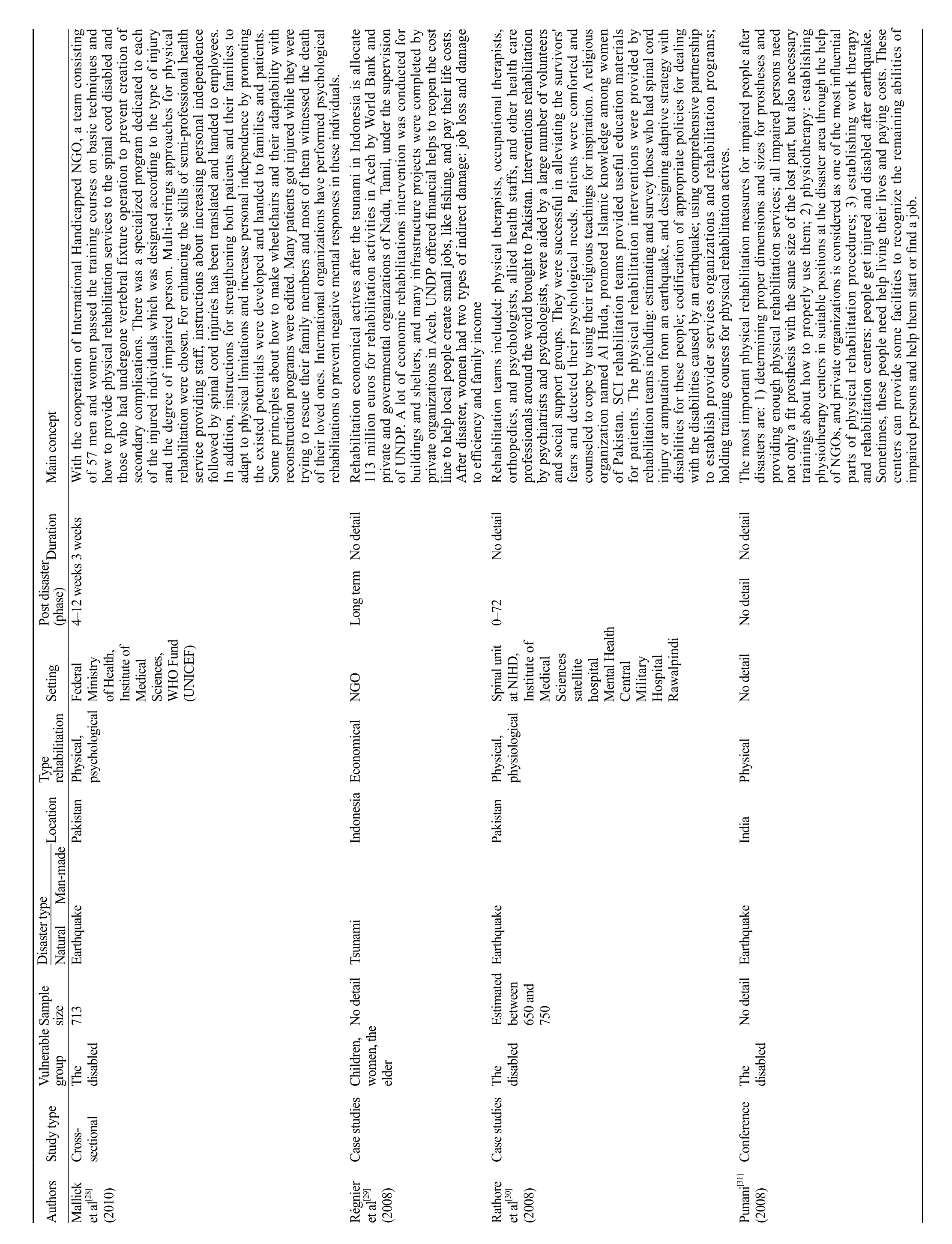
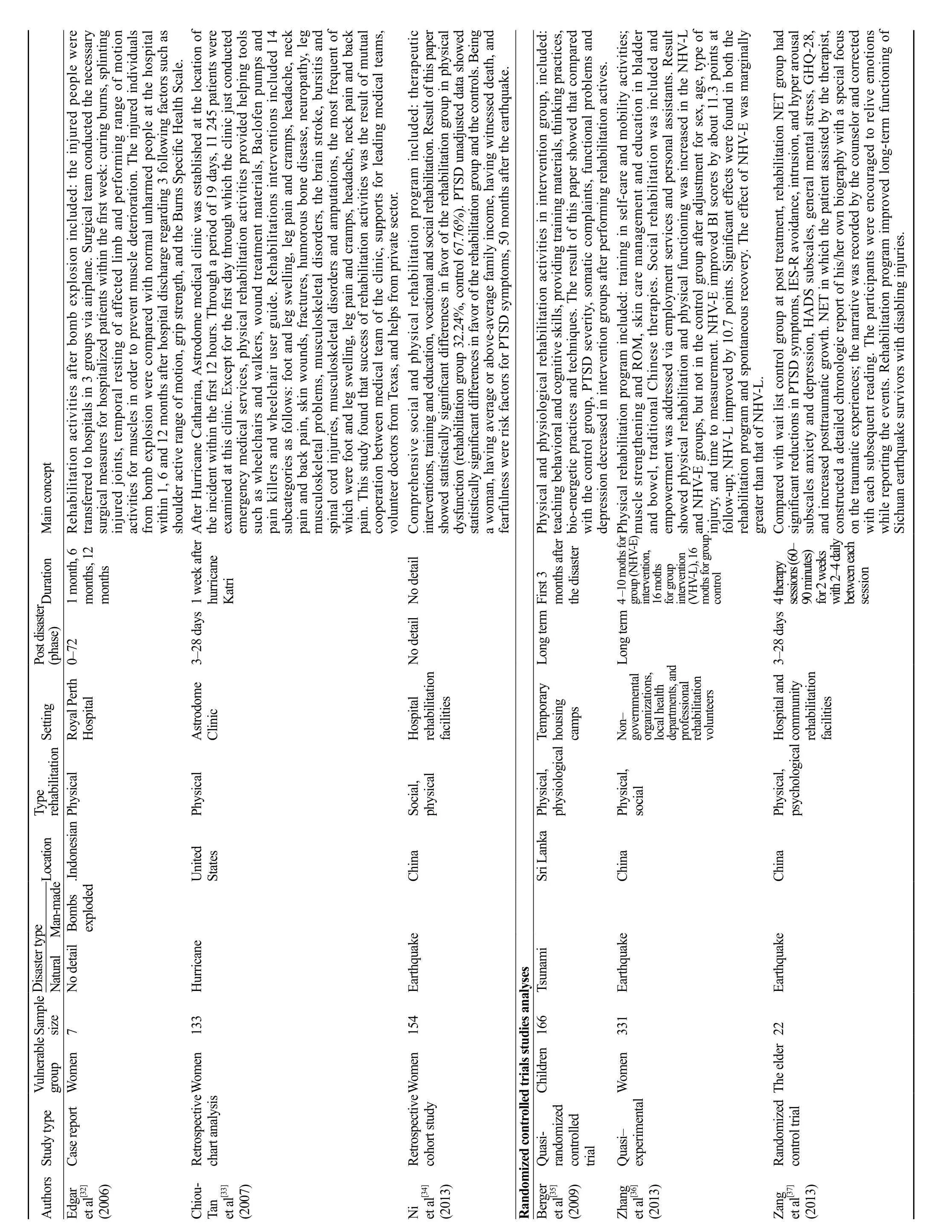
Number of participants of these twenty-five studies were 3 879 in total, which consist of 1 347 females, 145 children, 217 the elderly and 1 517 the disabled. Details of each study and their special features were reported regarding authors, year, study type, vulnerable group,sample size, type of rehabilitation, setting and duration of rehabilitation, disaster type, and main concepts. The studies were mainly conducted in Asian countries and United States, including India,[15,19,20,25–27,31]China,[18,22,23,34,36,37]Pakistan,[16,28,30]Iran,[13,17,21]Indonesia,[29,32]Sri Lanka[35]and United States.[14,24,33]The results of the studies showed that 56% of the studies are about rehabilitation programs for women, 32% is for children, 24% is for elderly, and 16%is for disabled people. Each study included more than onevulnerable group. The mean of the period of physical,psychological, social, and economic rehabilitation programs was about 7.3 months varying from 1 week to 50 months, which were based on the type of the disaster and the countries where the disaster occurred. For instance,psychological rehabilitation period after hurricane Katrina in the USA was about 1 week, and physical and psychological rehabilitation period after an earthquake in China was about 50 months.
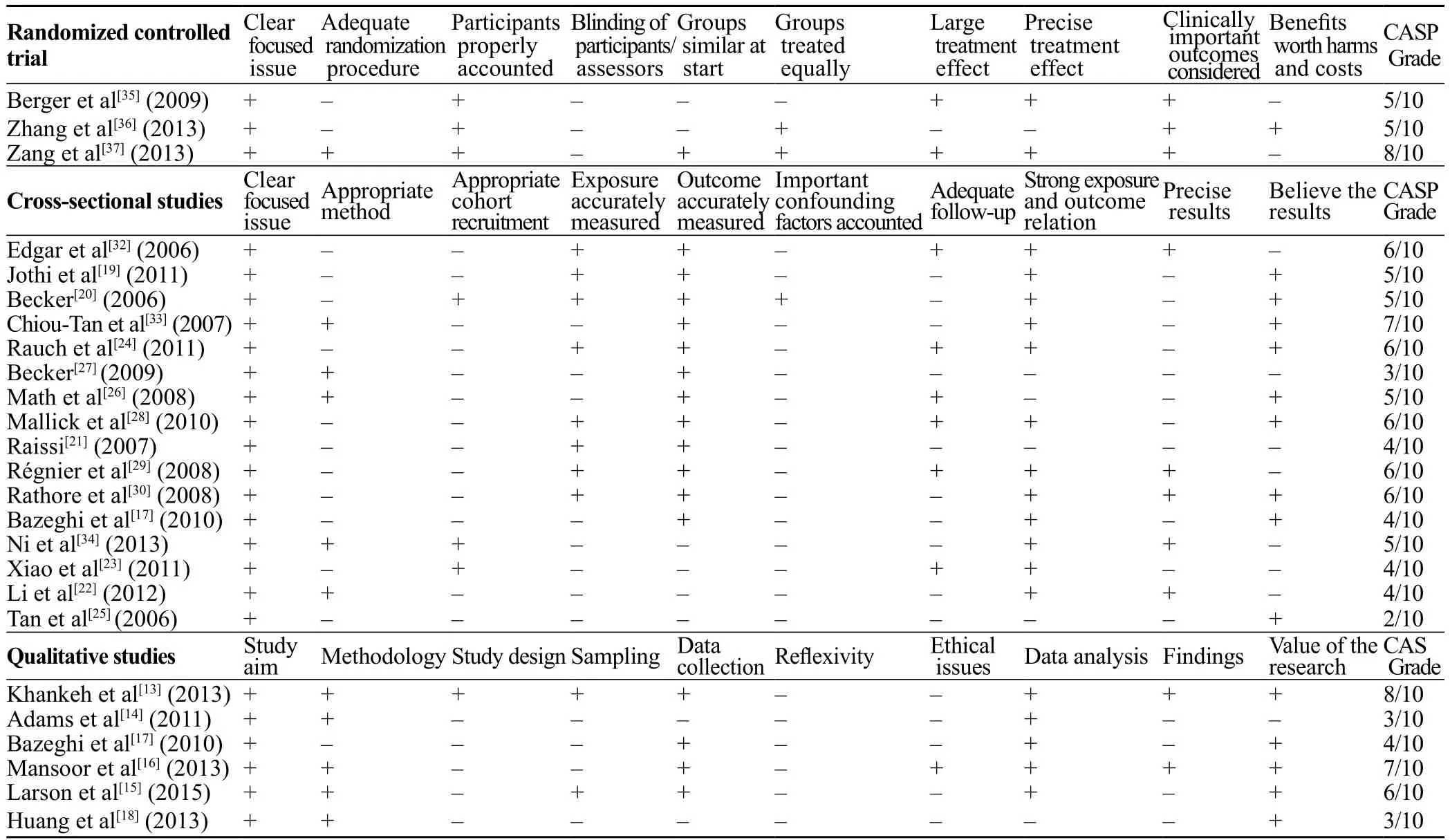
Table 1. The quality of the final extracted articles using Critical Appraisal Skills Program (CASP)[11,12]
Among all rehabilitation programs implemented after the disaster, 52% of them were for physical rehabilitation,48% were for psychological rehabilitation, 52% were for social rehabilitation, and 12% of them were for economic rehabilitation. That means each study had more than one type of rehabilitation program. The results of the studies also showed that the countries implemented a wide range of rehabilitation programs for vulnerable groups after the onset of the disasters, but the exact starting time of the programs were not declared. Rehabilitation activities were conducted at different locations such as hospitals,clinics, schools, temporary camps by rehabilitation teams from local (84%) and international (16%) governmental and non-governmental organizations including UNICEF,WHO, and World Bank (IBRD).
Main results
Studies showed no difference between the nature of the implementation of rehabilitation programs and activities based on the type of the disaster and different vulnerable groups. The most important common strategy for vulnerable groups for physical rehabilitation include immediate and early implementation of physical rehabilitation immediately after the response stage and to continue these actions in the society after victims discharge from health centers. Important strategies for psychological rehabilitation include early medical intervention and consultation for all vulnerable groups,focusing on a cooperation approach of the vulnerable groups with the same sex and the same age in order to remove the negative experience and tension especially in women and children.
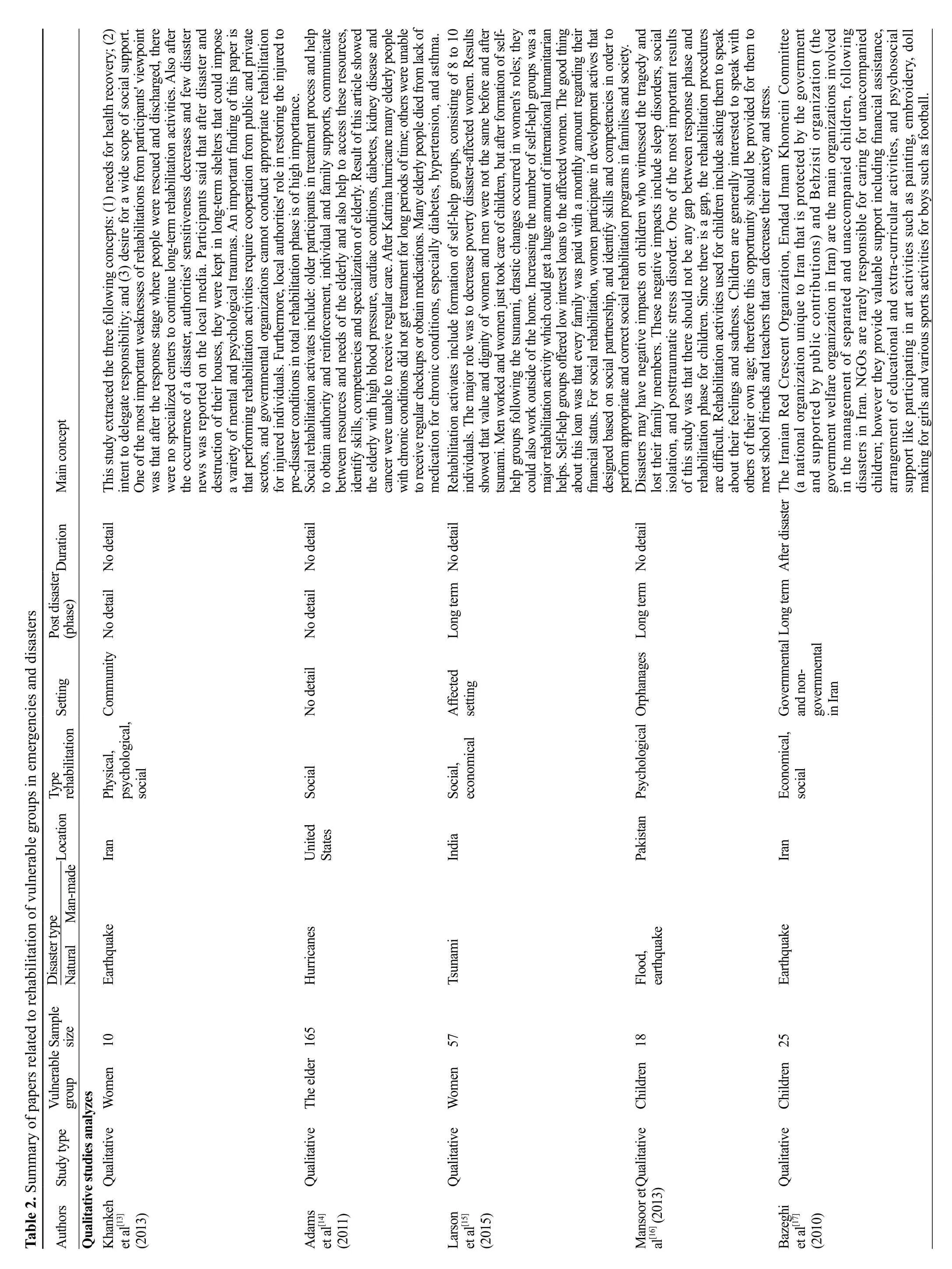
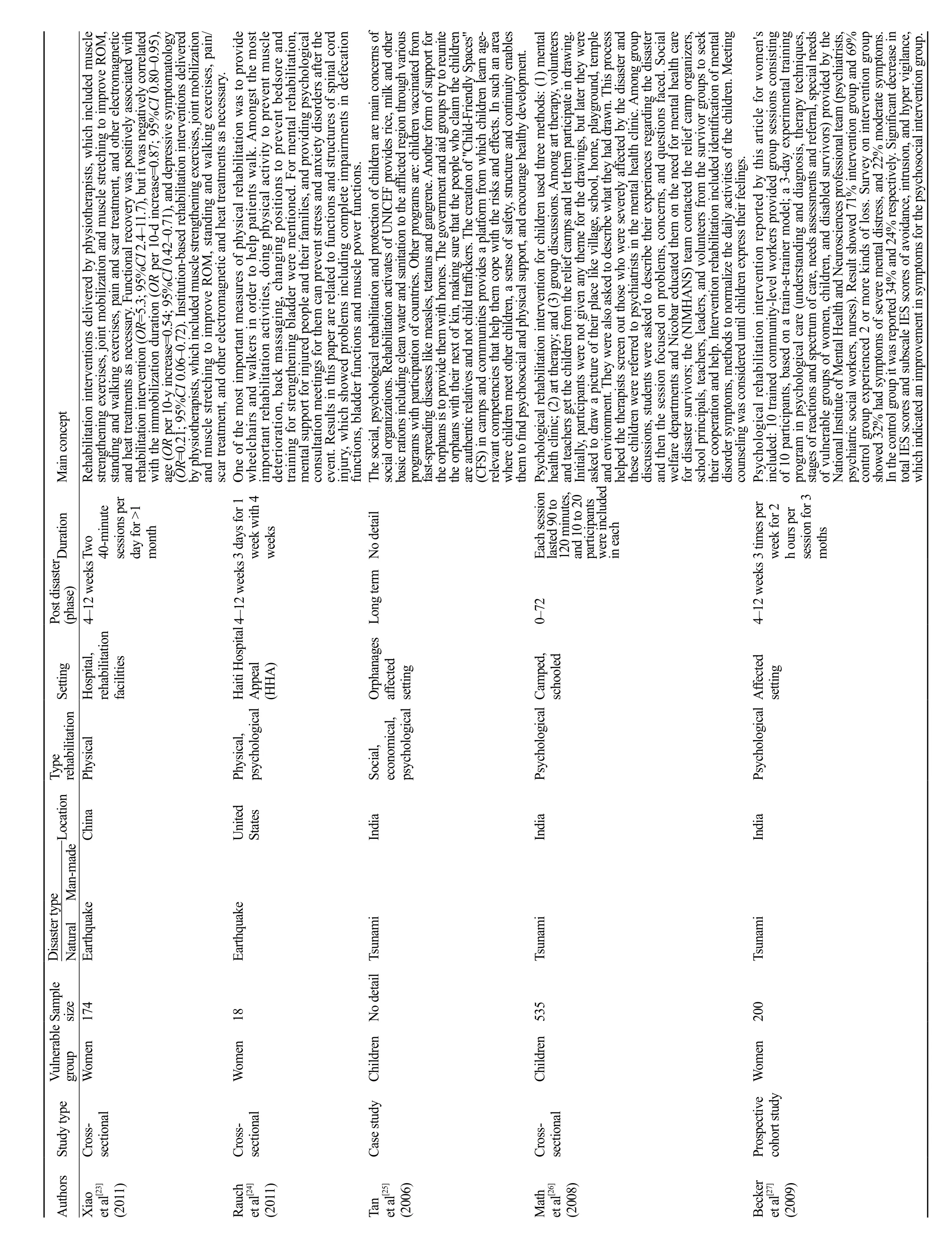
Strategies for social rehabilitation include emphasis on the participation of the vulnerable groups in the planning and implementation of services and activities from the day after the disaster. These strategies are based on holding proper training courses by local and international organizations especially local media in order to increase the capacity and potency of the people and the society. Strategies for economic rehabilitation include emphasizing the importance of women's role as a financial source in the family by providing them with small businesses, providing families with low-interest loans by international organizations, and providing societies with local businesses based on the culture of the damaged society by the World Bank. Moreover,the summaries of each paper related to rehabilitation of vulnerable groups in emergencies and disasters are shown in Table 2.
DISCUSSION
This systematic review provides an overview of various type of rehabilitation for vulnerable group in emergencies and disasters. This review includes 25 studies (6 qualitative, 16 cross-sectional and 3 randomized controlled trial). Most interventions evaluated in these studies were complex and included more than one active rehabilitation component. The most common kinds of rehabilitation intervention for vulnerable group were physical, social, and psychological activities.
The studies showed that the duration of the implementation of the rehabilitation programs after the onset of the disaster ranged from 1 week to 50 months and the mean of this period is about 7 months. The studies also showed that local public and private organizations performed 84% of the rehabilitation interventions, and international organizations performed 16% of these interventions.These findings are in line with the WHO guideline, which states that the success of the rehabilitation programs after the disaster depends on potential of the damaged area in meeting their needs independent of external aids and supports of non-local organizations.[40]The disaster management experts believe both natural disasters and human-made disasters lead to physical, economic, and social damages,[13,19]and there was no difference in the nature and implementation of rehabilitation programs based on vulnerable groups.
The important result shows physical and psychological rehabilitation programs started immediately after the response phase, which would better preserve function of body organs and cause less psychological signs and symptoms.[36,37]Disaster management experts believe that physical and physiological rehabilitation should be immediately started after response phase to disaster and it should continue in the community over the long term in order to improve and restore function of vulnerable peoples.[13,38,39]

One of the studies emphasized social rehabilitation of vulnerable groups in order to ensure the participation of vulnerable groups in the planning and implementation of services and activities from the day after the onset of the disaster based on the equal time and opportunity to governmental authorities and aid agencies. The strategies that can increase the participation of the vulnerable groups in meeting their needs include: (1) providing services with the cooperation of the people based on the capacity and potency; and (2) dependency of the vulnerable groups to the external services that should be gradually decreased. Reciprocally the use of social sources of the damaged area may be increased.[14,15,18,21,25,28,34]
Studies also emphasized the activity of vulnerable groups especially women in the economic rehabilitation activities in order to meet financial needs by starting small businesses. Supporting the social activity of women leads to ability to direct and organize many active and potent individuals. The most important obstacle for the cooperation of the women in economic rehabilitation activities is the focus of international and local organizations on men as the head of the family and the provider of the financial needs of the family.[15,17,29]Studies also showed that one of the most important approaches in implementation of the rehabilitation processes is the use of local media especially television and radio to provide vital information about rehabilitation procedures such as training courses for the vulnerable groups. Audiovisual tools play an important role in gathering social sources to provide rehabilitation services.[19]
The main barriers for implementing rehabilitations programs reported in some of the studies were lack of detailed information of affected population, lack of trained personnel, structural and non-structural destruction caused by emergencies and disasters, shortage of trained rehabilitation professionals and medical workforce, lack of coordination with other responsible agencies and private volunteer organizations, reduced sensitivity of authorities after a few days from disaster, and lack of comprehensive management plans for disabilities persons after occurrence emergencies and disasters.[13,14,21,28]We did not find any programs related to spiritual rehabilitation for vulnerable groups after emergencies and disasters. Some of reviewed articles did not specify details regarding the duration of rehabilitation period, which was recognized as one of the studies weaknesses.
CONCLUSION
The review of the papers showed different programs of physical, physiological, economic and social rehabilitations for vulnerable groups after emergencies and disasters. These programs may help health field managers better implement correct and timely rehabilitation activities. This review emphasizes comprehensive participation of people affected in all stages of rehabilitation programs and also attention to cultural, social, economic and religious considerations during implementation of rehabilitation actives after emergencies and disasters. The majority of the papers emphasized that the rehabilitation process has different dimensions, in addition, implementation of each of them needs facilities, resources and special approaches that correlate to other domains. Occasionally there are overlaps between the activities related to all domains, so successful rehabilitation process from disasters requires a systemic and holistic viewpoint simultaneously with implementation of specific programs related to each domain.
Funding: None.
Ethical approval: The institutional ethics review board approved the study.
Conflicts of interest: No authors declare any actual or potential conflicts of interest.
Contributors: All authors carried out the design, SH and FR coordinated to the data base search. All authors prepared the manuscript, read and approved the content of the manuscript.
1 Organisation WH, Time G. Earthquake disaster in Bam,Iran Preliminary indication of urgent requirements for those responding to the health needs of the affected population. 2003;(December).
2 Guha Sapir D, Vos F, Below R, Ponserre S. Annual Disaster Statistical Review 2010: The Numbers and Trends; Centre for Research on the Epidemiology of Disasters (CRED), Université catholique de Louvain: Brussels, Belgium, 2011; 41.
3 Li XH, Hou SK, Zheng JC, Fan HJ, Song JQ. Post-disaster medical rescue strategy in tropical regions. World J Emerg Med.2012;3(1):23–8.
4 Jha A, Basu R, Basu A. Studying policy changes in disaster management in india: a tale of two cyclones. Disaster Med Public Health Prep. 2016;10(1):42–6.
5 National policy gudelie on vulnearable group in disaster published: may 2014. Available at: www.ndma.gov.pk/site/plans/gcc_policy
6 Kapucu N. Collaborative Governance and Disaster Recovery:The National Disaster Recovery Framework (NDRF) in the US.In: Disaster Recovery 2014;41–59.
7 Punani B. Natural Disasters, Role of Disability Development Organizations. International Conference on Disasters &Disability; 28th & 29th January 2008; Shanta Memorial,Rehabilitation Centre, Bhubaneswar, Orissa; 62–64.
8 Khatam A. The destruction of Bam and its reconstruction following the earthquake of December 2003. Cities. 2006; 23(6):462–4.
9 Abdi K, Arab M, Rashidian A, Kamali M, Khankeh HR, Farahani FK. Exploring barriers of the health system to rehabilitation services for people with disabilities in Iran: A Qualitative Study.Electronic physician. 2015;7(7):1476.
10 Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group.Preferred reporting items for systematic reviews and metaanalyses: the PRISMA statement. Ann Intern Med. 2009; 151(4):264–9, W64.
11 Critical Appraisal Skills Programme. 10 Questions to make sense of qualitative research [2006]. Available at: http://www.phru.nhs.uk/pages/phd/resources.htm. Accessed January 2008.
12 Critical Appraisal Skills Programme. CASP checklists. Available at: http://www.casp- tools-checklists/c18f8. Accessed September 20, 2014.
13 Khankeh H, Nakhaei M, Masoumi G, Hosseini M, Parsa-Yekta Z, KurlandL, et al. Life recovery after disasters: a qualitative study in the Iranian context. Prehosp Disaster Med. 2013; 28(6):573–9.
14 Adams V, Kaufman SR, Van Hattum T, Moody S. Aging disaster:mortality, vulnerability, and long-term recovery among Katrina survivors. Med Anthropol. 2011;30(3):247–70.
15 Larson G, Drolet J, Samuel M. The role of self-help groups in post-tsunami rehabilitation. International Social Work. 2015;58(5):732–42.
16 Mansoor T, Yaqoob T. Psychological impact of disaster and rehabilitation of children in orphanages. J Asian Dev Stud. 2013;2(3):6–17.
17 Bazeghi F, Baradaran HR. The role of non-governmental organisations in the management of separated and unaccompanied children, following disasters in Iran. BMC Res Notes. 2010;3:256.
18 Huang Y, Wong H. Effects of social group work with survivors of the Wenchuan earthquake in a transitional community. Heal Soc Care Community. 2013;21(3):327–37.
19 Jothi SP, Neelamalar M. The role of media in science and technology education,development and rehabilitation of women affected by the 2004 tsunami in the state of Tamilnadu. Science of Tsunami Hazards. 2011;30(2):108–25.
20 Becker SM. Psychosocial care for adult and child survivors of the 2004 tsunami disaster in India. Am J Public Health. 2006;96(8):1397–8.
21 Raissi GR. Earthquakes and rehabilitation needs: experiences from Bam, Iran. J Spinal Cord Med. 2007;30(4):369–72.
22 Li Y, Reinhardt JD, Gosney JE, Zhang X, Hu X, Chen S, et al.Evaluation of functional outcomes of physical rehabilitation and medical complications in spinal cord injury victims of the Sichuan earthquake. J Rehabil Med. 2012;44(7):534–40.
23 Xiao M, Li JA, Zhang X, Zhao ZE. Factors affecting functional outcome of Sichuan-earthquake survivors with tibial shaft fractures: a follow-up study. J Rehabil Med. 2011;43(6):515–20.
24 Rauch A, Baumberger M, Moise FG, von Elm E, Reinhardt JD.Rehabilitation needs assessment in persons with spinal cord injury following the 2010 earthquake in Haiti: a pilot study using an ICF-based tool. J Rehabil Med. 2011;43(11):969–75.
25 Tan NT. Impact of the Indian Ocean tsunami on the well-being of children. J Soc Work Disabil Rehabil. 2006;5(3–4):43–56.
26 Math SB, Tandon S, Girimaji SC, Benegal V, Kumar U, Hamza A, et al. Psychological impact of the tsunami on children and adolescents from the andaman and nicobar islands. Prim Care Companion J Clin Psychiatry. 2008;10(1):31–7.
27 Becker SM. Psychosocial care for women survivors of the tsunami disaster in India. Am J Public Health. 2009;99(4):654–8.
28 Mallick M, Aurakzai JK, Bile KM, Ahmed N. Large-scale physical disabilities and their management in the aftermath of the 2005 earthquake in Pakistan. East Mediterr Health J. 2010;16 Suppl:S98–105.
29 Régnier P, Neri B, Scuteri S, Miniati S. From emergency relief to livelihood recovery: lessons learned from post-tsunami experiences in Indonesia and India. Disaster Prev Manag. 2008;17(3):410–30.
30 Rathore FA, Farooq F, Muzammil S, New PW, Ahmad N, Haig AJ. Spinal cord injury management and rehabilitation: highlights and shortcomings from the 2005 earthquake in Pakistan. Arch Phys Med Rehabil. 2008;89(3):579–85.
31 Punani B. Natural disasters, role of disability development organizations. Int Conf Disasters Disabil. 2008;62–4.
32 Edgar DW, Wood F, Goodwin-Walters A. First response,rehabilitation, and outcomes of hand and upper limb function:survivors of the Bali bombing disaster. A case series report. J Hand Ther. 2006;19(3):283–97
33 Chiou-Tan FY, Bloodworth DM, Kass JS, Li X, Gavagan TF,Mattox K, et al. Physical medicine and rehabilitation conditions in the Astrodome clinic after hurricane Katrina. Am J Phys Med Rehabil. 2007;86(9):762–9.
34 Ni J, Reinhardt JD, Zhang X, Xiao M, Li L, Jin H, et al.Dysfunction and post-traumatic stress disorder in fracture victims 50 months after the Sichuan earthquake. PLoS One.2013;8(10):e77535.
35 Berger R, Gelkopf M. School-based intervention for the treatment of tsunami-related distress in children: a quasi-randomized controlled trial. Psychother Psychosom. 2009;78(6): 364–71.
36 Zhang X, Reinhardt JD, Gosney JE, Li J. The NHV Rehabilitation Services Program improves long-term physical functioning in survivors of the 2008 Sichuan earthquake: a longitudinal quasi experiment. PLoS One. 2013;8:e53995.
37 Zang Y, Hunt N, Cox T. A randomised controlled pilot study: the effectiveness of narrative exposure therapy with adult survivors of the Sichuan earthquake. BMC Psychiatry 2013;13:41.
38 Gosney J, Reinhardt JD, Haig AJ, Li J. Developing post-disaster physical rehabilitation: role of the World Health Organization Liaison Sub-Committee on Rehabilitation Disaster Relief of the International Society of Physical and Rehabilitation Medicine. J Rehabil Med. 2011;43(11):965–8.
39 Talati S, Bhatia P, Kumar A, Gupta AK, Ojha CD. Strategic planning and designing of a hospital disaster manual in a tertiary care, teaching, research and referral institute in India. World J Emerg Med. 2014;5(1):35–41.
40 World Health Organization. Community-based rehabilitation guidelines. Geneva: World Health Organization; 2010.
Mohammad Reza Maracy, Email: mrmaracy@yahoo.co.uk
BACKGROUND:Natural and man-made disasters, especially those occurring in large scales not only result in human mortality, but also cause physical, psychological, and social disabilities.Providing effective rehabilitation services in time can decrease the frequency of such disabilities. The aim of the current study was to perform a systematic review related to rehabilitation of vulnerable groups in emergencies and disasters.
METHODS:The systematic review was conducted according to the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines. The key words "recovery", "rehabilitation","reconstruction", "transformation", "transition", "emergency", "disaster", "crisis", "hazard", "catastrophe","tragedy", "mass casualty incident", "women", "female", "children", "pediatric", "disable", "handicap","elder", "old" and "vulnerable" were used in combination with Boolean operators OR and AND. ISI Web of Science, PubMed, Scopus, Science Direct, Ovid, ProQuest, Wiley, Google Scholar were searched.
RESULTS:In this study a total of 11 928 articles were considered and 25 articles were selected for final review of rehabilitation of vulnerable groups based on the objective of this study. Twenty-five studies including six qualitative, sixteen cross-sectional and three randomized controlled trials were reviewed for rehabilitation of vulnerable groups in emergencies and disasters. Out of the selected papers, 23 were studied based on rehabilitation after natural disasters and the remaining were man-made disasters.Most types of rehabilitation were physical, social, psychological and economic.
CONCLUSION:The review of the papers showed different programs of physical, physiological,economic and social rehabilitations for vulnerable groups after emergencies and disasters. It may help health field managers better implement standard rehabilitation activities for vulnerable groups.
World J Emerg Med 2017;8(4):253–263
10.5847/wjem.j.1920–8642.2017.04.002
December 12, 2016
Accepted after revision July 9, 2017
 World journal of emergency medicine2017年4期
World journal of emergency medicine2017年4期
- World journal of emergency medicine的其它文章
- Procedural simulation: medical student preference and value of three task trainers for ultrasound guided regional anesthesia
- Instructions for Authors
- Evaluation of a point of care ultrasound curriculum for Indonesian physicians taught by first-year medical students
- Education in cardiopulmonary resuscitation in Russia:A systematic review of the available evidence
- Paediatric-appropriate facilities in emergency departments of community hospitals in Ontario:A cross-sectional study
- Factors behind not using child restrain(t) among hospital employees and general population:A case control study