
创伤性脾破裂患者不同病情及不同时间外周血肌酸激酶的变化
2017-07-31 16:38:51杨晓曦
湖南师范大学学报(医学版) 2017年4期
任 琴 ,杨晓曦
(四川省雅安市中医医院检验科,雅安 625000)
创伤性脾破裂患者不同病情及不同时间外周血肌酸激酶的变化
任 琴 ,杨晓曦
(四川省雅安市中医医院检验科,雅安 625000)
目的:研究创伤性脾破裂患者不同病情及不同时间外周血肌酸激酶的变化。方法:选择2013年1月~2015年12月在我院进行诊治的60例创伤性脾破裂患者为脾破裂组,60例非脾破裂的腹部外伤患者为腹部外伤组,40例体检健康者为对照组,对照组在体检当日检测心肌酶谱,另外两组分别于术前、术后2 h、术后12 h、术后1d、术后3 d及术后7 d检测心肌酶谱,比较三组心肌酶谱的检测结果。结果:脾破裂组和腹部外伤组患者经过手术治疗后,全部痊愈出院,在住院期间及术后随访半年内均未发生心肌梗死;与对照组相比,脾破裂组和腹部外伤组术前酸激酶与其同工酶均明显升高,与腹部外伤组组相比,脾破裂组在不同时间的酸激酶与其同工酶均明显升高;Ⅲ、Ⅳ级脾破裂患者在不同时间外周血肌酸激酶均高于I、Ⅱ级患者,但差异均无统计学意义,Ⅲ、Ⅳ级患者在T0、T1、T2、T3,外周血肌酸激酶同工酶均明显高于I、Ⅱ级患者。结论:创伤性脾破裂患者早期外周血肌酸激酶及其同工酶均升高,且肌酸激酶同工酶的变化与脾破裂损伤程度呈正相关,提示创伤性脾破裂早期可能发生了心肌损伤,应尽早检测并关注患者心肌酶谱的变化。
创伤性脾破裂;心肌损伤;肌酸激酶;肌酸激酶同工酶
脾作为一个质脆而血供丰富的实质性器官,是最容易遭受外力创伤造成破裂失血的腹部脏器之一[1]。创伤性脾破裂在腹部损伤中较为常见,如果不给予及时有效的抢救治疗,就有可能引发失血性休克,并发多器官功能衰竭,造成患者死亡[2]。创伤性脾破裂患者常会出现一过性的心肌酶水平升高,有研究表明,钝性创伤性胸部损伤可能导致心脏损伤,引发急性心肌梗死[3]。血肌酸激酶与其同工酶是反映心肌损伤的主要指标[4]。本文主要研究了研究创伤性脾破裂患者不同病情及不同时间外周血肌酸激酶的变化,以探讨创伤性脾破裂对心肌的影响。
1 资料与方法
1.1 一般资料选择2013年1月~2015年12月在我院进行诊治的60例创伤性脾破裂患者为脾破裂组,男36例,女24例;年龄28~52岁,平均(41.56±9.78)岁;根据损伤程度进行分级:I、Ⅱ级23例,Ⅲ、Ⅳ级37例;60例非脾破裂的腹部外伤患者为腹部外伤组,男35例,女25例;年龄29~53岁,平均(42.37±10.15)岁;肝损伤12例,肠系膜损伤14例,胰腺挫伤9例,肠管破裂25例;40例体检健康者为对照组,男23例,女17例;年龄26~51岁,平均(40.35±9.36)岁。本研究获得我院伦理委员会的批准,所有研究对象均签署知情同意书。
1.2 方法患者入院后立刻建立静脉通道,补充血容量。进行全身麻醉后,对脾破裂组的患者行全脾切除术,腹部外伤组按照患者的具体情况与术中探查结果采取相对应的手术治疗方式。
对照组在体检当日采集外周静脉血,采用日本7180型全自动生化分析仪用速率法检测心肌酶谱,另外两组分别于T0(术前)、T1(术后2 h)、T2(术后12 h)、T3(术后1d)、T4(术后3 d)及T5(术后7 d)检测心肌酶谱,比较三组心肌酶谱的检测结果。
1.3 统计学分析采用SPSS15.00软件,采用SNK-q检验进行两两比较,采用重复测量数据的方差分析进行多个时间点数据间的比较,以P<0.05表明差异有统计学意义。
2 结果
2.1 两组手术治疗结果脾破裂组和腹部外伤组患者经过手术治疗后,全部痊愈出院,在住院期间及术后随访半年内均未发生心肌梗死。
2.2 三组肌酸激酶与其同工酶的比较与对照组相比,脾破裂组和腹部外伤组术前酸激酶与其同工酶均明显升高(P<0.05),与腹部外伤组组相比,脾破裂组在不同时间的酸激酶与其同工酶均明显升高(P<0.05),见表1。
2.3 脾破裂组不同损伤程度患者不同时间肌酸激酶与其同工酶的比较Ⅲ、Ⅳ级脾破裂患者在不同时间外周血肌酸激酶均高于I、Ⅱ级患者,但差异均无统计学意义(P>0.05),Ⅲ、Ⅳ级患者在T0、T1、T2、T3,外周血肌酸激酶同工酶均明显高于I、Ⅱ级患者(P<0.05),见表2。
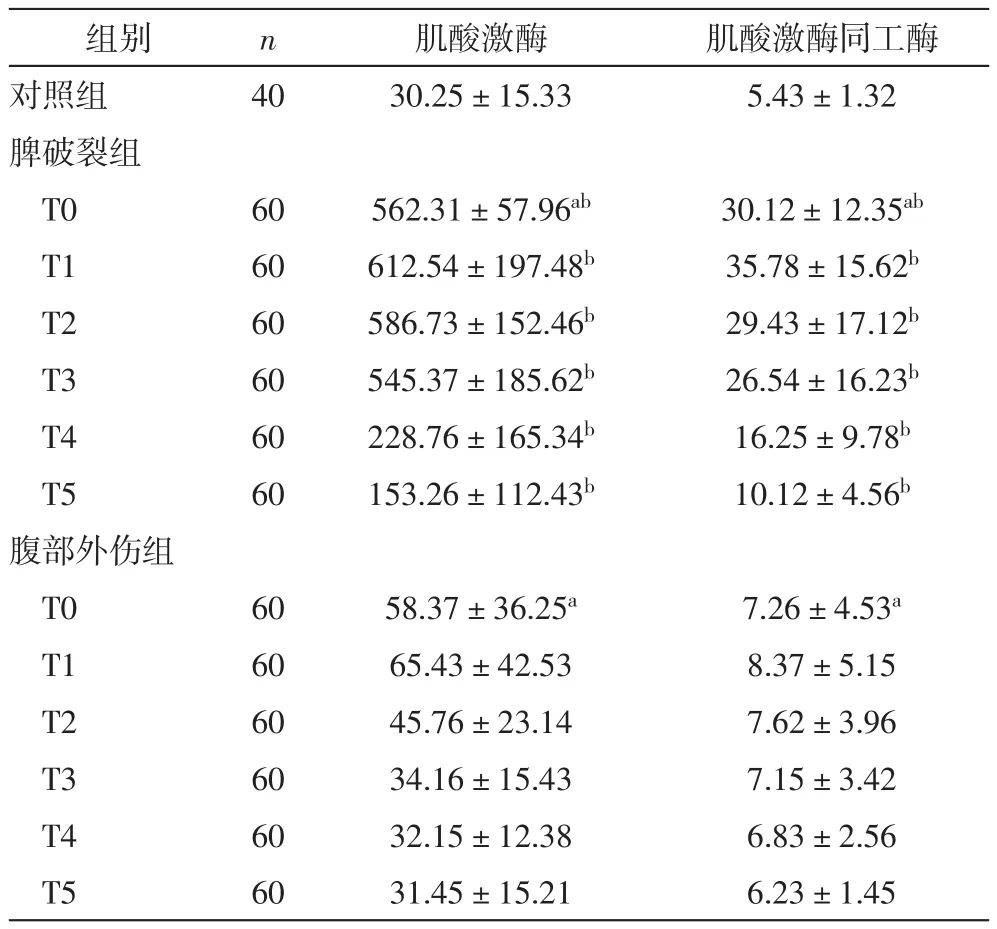
表1 三组肌酸激酶与其同工酶的比较(U/L)
表2 脾破裂组不同损伤程度患_者不同时间肌酸激酶与其同工酶的比较(±s,U/L)
与Ⅲ、Ⅳ级相比,cP<0.05
分级 n 肌酸激酶 肌酸激酶同工酶I、Ⅱ级T0 23 556.12±163.45 26.32±17.42cT1 23 625.13±216.78 31.56±16.45cT2 23 534.26±179.46 26.33±15.78cT3 23 527.45±176.32 23.62±17.96cT4 23 196.25±123.46 14.58±9.72 T5 23 125.56±82.45 9.56±5.33Ⅲ、Ⅳ级T0 37 562.36±172.43 38.96±12.13 T1 37 635.13±223.45 43.56±14.92 T2 37 553.18±179.26 35.78±16.12 T3 37 545.41±152.68 29.12±18.96 T4 37 213.48±156.72 16.53±9.24 T5 37 136.42±89.75 10.12±5.35
3 讨论
脾脏作为人体最大的淋巴器官,具有造血、滤过血液、储血,增强免疫等功能[5]。因质地脆弱且柔软,位置固定且表浅,是腹腔内最易受到损伤并引发腹腔内大出血的脏器,脾破裂居腹部实质性脏器闭合性损伤的第一位[6-7]。脾破裂可分为中央型脾破裂、真性脾破裂和包膜下脾破裂,其主要临床表现包括血液对腹膜引起的刺激和内出血[8-9]。脾损伤程度可分为四级,Ⅰ、Ⅱ级病情程度相对较轻,损伤未累及到脾门,Ⅲ、Ⅳ级可伤及脾叶及脾门血管动静脉主干,脾发生广泛破裂[10]。
由于脾破裂患者受到原发机械性损伤和继发性的水肿、出血等引起的缺氧和缺血的影响,使得细胞的能量供应转变成无氧酵解型,造成细胞膜通透性增大,功能受到损伤[11]。另一方面,因为脾破裂患者血小板一般会出现明显的升高,血液黏稠度增加,造成心肌相对供血不足,加重心肌损伤程度,从而机体会释放大量心肌酶入血[12]。Probst等[13]研究发现,血液动力学发生的改变会对心脏功能产生严重影响,外伤能对患者的心肌功能造成损伤。但目前国内外关于脾破裂是否会引起心肌损伤的报道较为少见。鉴于此,文主要研究了创伤性脾破裂患者早期外周血肌酸激酶与其同工酶的变化和意义。
本结果发现,与对照组相比,脾破裂组和腹部外伤组术前酸激酶与其同工酶均明显升高,与腹部外伤组组相比,脾破裂组在不同时间的酸激酶与其同工酶均明显升高;提示检测血清心肌酶与其同工酶水平,对于观察脾破裂患者病情有一定的敏感性,可以为病情和预后的判断提供临床参考依据。Ⅲ、Ⅳ级脾破裂患者在不同时间外周血肌酸激酶均高于I、Ⅱ级患者,但差异均无统计学意义,Ⅲ、Ⅳ级患者在T0、T1、T2、T3,外周血肌酸激酶同工酶均明显高于I、Ⅱ级患者。分析其原因可能为不同脾破裂损伤程度的患者均会发生肌肉损伤,使外周血肌酸激酶升高,因此损伤程度不会对肌酸激酶产生明显影响;但患者如损伤程度较为严重,失血量的增多会更易引发心肌细胞缺血,导致肌酸激酶同工酶的明显升高,该结果提示肌酸激酶同工酶的变化与脾破裂损伤程度呈正相关,创伤性脾破裂早期可能发生了心肌损伤,要加强对脾破裂患者,尤其是有心脏基础疾病的患者的心脏监测。
综上所述,创伤性脾破裂患者早期外周血肌酸激酶及其同工酶均升高,且肌酸激酶同工酶的变化与脾破裂损伤程度呈正相关,提示创伤性脾破裂早期可能发生了心肌损伤,应尽早检测并关注患者心肌酶谱的变化。
[1] 冯以斌, 别玉坤, 杨成林, 等. 腹腔镜与开腹手术在脾切除术中的应用效果与术后感染发生的危险因素[J]. 湖南师范大学学报 (医学版), 2015, 12(3): 103-105.
[2] Chen T, Feng R, Weiyuan L V, et al. Analysis of the Clinical Emergency Treatment of 330 Cases of Traumatic Rupture of Spleen[J]. China & Foreign Medical Treatment, 2014, 51(1): 77-93.
[3] GoranAugustin M D. Spleen[J], Acute Abdomen During Pregnancy, 2014, 11(4): 44-45.
[4] Chih-Chun C, Ching-Biau L, Ming-Jang S, et al. Creatine Kinase (CK) -MB-to-Total-CK Ratio: a Laboratory Indicator for Primary Cancer Screening [J]. Asian Pacific Journal of Cancer Prevention Apjcp, 2015,16(15): 6599-6603.
[5] Melchionda F, Varani S, Carfagnini F, et al. Spleen nodules: a potential hallmark of Visceral Leishmaniasis in young children[J]. Bmc Infectious Diseases, 2014, 14(14): 620-623.
[6] André M S, Belisa Maria L M, Gisely C M, et al. Spleen rupture in a case of untreated Plasmodium vivax infection [J]. Plos Neglected Tropical Diseases, 2012, 6(12): 488-496.
[7]Baibars M, Ohrum P, Alraiyes AH, et al. Asymptomatic spleen rupture in patient with endocarditis[J]. American Journal of Medical Genetics Part A, 2015, 167A (3): 587-591.
[8] 谢海珊, 丛林, 朱文晖, 等. B超对外伤性脾破裂的诊断及临床应用[J]. 湖南师范大学学报 (医学版), 2006, 3(4): 23-25.
[9]Sanjeev K, Shefali G, Ravi P, et al. Simultaneous primary hydatid cysts of liver and spleen with spontaneous intraperitoneal rupture of liver cyst [J]. Southern Medical Journal, 2014, 8(11): 299-306.
[10] Yamamoto T, Kobayashi H, Sakamoto Y, et al. A Case of Splenic Angiosarcoma with Rupture of the Spleen[J]. Nihon RinshoGekaGakkaiZasshi, 2014, 75(75): 544-548.
[11] De Santis G C, Oliveira L C, Ramos A F, et al. Pathologic rupture of the spleen in a patient with acute myelogenous leukemia and leukostasis[J]. RevistaBrasileira De Hematologia E Hemoterapia, 2014, 36(4): 290-292.
[12] Geraci G, Picciurro A, Attard A, et al. A case of splenic rupture: a rare event after laparoscopic cholecystectomy [J]. Bmc Surgery, 2014, 14(14): 106-108.
[13] Probst C, Hildebrand F, Griensven MV, et al. Is dopexaminesuperior to dopamine in the treatment of multiple trauma patients: a prospective, double blind, randomised study[J]. Injurynt J Care Injured, 2010, 41(5): 499-505.
Change of peripheral blood creatine kinase in patients w ith traumatic splenic rupture in different conditions and different time
Ren Qin, Yang Xiao-xi
(Department of laboratory, Ya’an Hospital of Traditional Chinese Medicine, Ya’an 625000, China)
Objective Change of peripheral blood creatine kinase in patients with traumatic splenic rupture in different conditions and different time. M ethods Selected 60 cases of patients with traumatic splenic rupture who were treated in our hospital from January 2013 to December 2015 asrupture group, 60 cases of patients with abdominal trauma but non-rupture were admitted to abdominal trauma group, 40 healthy person were enrolled to healthy control group. The myocardial enzymes were detected at before operation (T0), 2 h after operation (T1), 12 h after operation (T2), 24 h after operation (T3), 3 d after operation (T4) and 7 d after operation (T5). Results After surgical treatment, the patients in rupture group and abdominal trauma were all cured, and did not happen postoperative myocardial infarction; compared with control group, the kinase isozymeof rupture group and abdominal trauma group were significantly increased, compared with abdominal trauma group, theacid kinase isozymein rupture group were significantly higher; the peripheral blood creatine kinase at different time in patients withⅢ, Ⅳgrade spleen rupture were higher than patients with I, Ⅱgrade spleen rupture, but there were no statistically significant difference, the blood creatine kinase isozyme in patients withⅢ, Ⅳ grade spleen rupture were significantly higher than patients with I,Ⅱgrade spleen rupture. Conclusion The creatine kinase and creatine kinase isoenzyme levels of patients with traumatic rupture appear elevated at early stage, the change of them are positively associated with the degree of injury, traumatic spleen rupture may prompt myocardial injury, it should be concerned myocardial enzymes changes as early as possible.
traumatic splenic rupture; myocardial injury; creatine kinase; creatine kinase isoenzyme
R541.7
A
1673-016X(2017)04-0055-04
2017-03-10
任琴,E-mail:renqin_198005@medicine360.net
猜你喜欢
遗传(2023年8期)2023-08-25 06:59:00
冰雪运动(2021年1期)2021-07-28 07:12:46
宁夏医学杂志(2020年3期)2021-01-21 08:23:38
安徽医专学报(2020年3期)2020-12-25 19:41:17
中国医药指南(2017年3期)2017-11-13 02:57:10
实用中医药杂志(2015年2期)2015-12-01 07:06:28
中国康复(2015年4期)2015-04-10 13:00:47
中国当代医药(2015年21期)2015-03-01 02:04:50
当代体育科技(2015年8期)2015-02-27 06:23:42
茶叶通讯(2014年2期)2014-02-27 07:55:39
