脊柱孤立性浆细胞瘤伴淀粉样变性
2017-03-29 06:39:38孙翠云于士柱
中国现代神经疾病杂志 2017年1期
孙翠云 于士柱
·临床病理报告·
脊柱孤立性浆细胞瘤伴淀粉样变性
孙翠云 于士柱
目的报告1例脊柱孤立性浆细胞瘤伴淀粉样变性患者的诊断与治疗过程,结合文献探讨其组织病理学特征。方法与结果女性患者,46岁,临床主要表现为双下肢无力,行走不稳伴脚趾麻木感。头部MRI显示,T5~7水平脊髓后方硬脊膜外和T6~7水平附件内不规则占位性病变,增强扫描呈不均匀明显强化,边界清晰,硬脊膜受压向前移位。术中可见T5~7棘突和椎板以及部分T5、T7棘突和椎板被侵蚀,骨皮质呈“虫蚀”样改变;病变位于椎管内硬脊膜外,血供丰富,呈疏松骨样结构,硬脊膜完整。组织学形态观察,肿瘤细胞以密集排列的小细胞为主,可见灶性浆细胞样细胞分化,其间可见片状粉染物质沉积,并多见人工裂纹和散在分布的多核巨细胞。免疫组织化学染色,肿瘤细胞胞质CD138、CD38和波形蛋白弥漫性阳性;白细胞共同抗原散在阳性;免疫球蛋白κ轻链和λ轻链、CD99、S-100蛋白、广谱细胞角蛋白、上皮膜抗原、黑色素瘤相关抗原HMB45和CD34阴性;Ki-67抗原标记指数约1.25%。特殊染色,粉染物质刚果红染色呈棕红色。原位杂交显示免疫球蛋白κ轻链DNA含量高于λ轻链。最终病理诊断为(脊柱)孤立性浆细胞瘤伴淀粉样变性。术后辅以药物化疗。随访18个月肿瘤无复发和转移。结论脊柱孤立性浆细胞瘤伴淀粉样变性临床罕见,影像学检查对诊断有一定提示意义,明确诊断仍依靠特异性组织形态学、免疫表型、特殊染色和原位杂交检测。
浆细胞瘤;淀粉样变性;脊柱;免疫组织化学;原位杂交;病理学
This study was supported by the National Natural Science Foundation of China(No.81402050, 81502166),Key Projects of Tianjin Application Foundation and Advanced Technology Research Project (No.15JCZDJC34600,15JCYBJC49900),the National Natural Science Foundation of Tianjin(No. 16JCQNJC13400),Foundation of Tianjin Medical University for Young Scientists(No.2015KYZQ11),and Tianjin Medical University General Hospital Youth Incubation Fund(No.ZYYFY2014038, ZYYFY2015032).
孤立性浆细胞瘤(SP)是浆细胞单克隆性增生导致的恶性肿瘤,可发生于骨骼或髓外组织,发病部位局限,骨髓无异常改变。发生于脊柱者平均发病年龄约55岁,男女比例为2∶1,主要累及椎体,临床主要表现为进行性加重的病变椎体周围疼痛。孤立性浆细胞瘤伴淀粉样变性临床罕见,主要由于免疫球蛋白轻链与多糖复合物沉积于组织器官所致,受累组织器官较广泛,包括舌、腮腺、皮肤、心脏、胃肠道、周围神经、肝、脾、肺等。明确诊断依靠组织病理学检查,刚果红染色呈棕红色。本文回顾研究1例脊柱孤立性浆细胞瘤伴淀粉样变性患者的诊断与治疗过程,结合相关文献对此类疾病的临床病理学特征进行分析,以期提高疾病的诊断与鉴别诊断能力。
病历摘要
患者女性,46岁,主因双下肢无力、行走不稳伴脚趾麻木感20 d余,于2016年6月4日入院。患者20 d前无明显诱因出现双下肢无力、行走不稳伴脚趾麻木感,未见其他伴随症状。门诊行脊椎MRI检查显示,T5~7水平硬脊膜外和T6~7水平附件区占位性病变。门诊以“脊柱占位性病变”收入院。患者自发病以来,精神、饮食佳,睡眠尚可,大小便正常,体重无明显变化。
既往史、个人史及家族史均无特殊。
体格检查患者体温36.2℃,心率67次/min,呼吸18次/min,血压125/80 mm Hg(1 mm Hg= 0.133 k Pa)。神志清楚,语言流利;双侧瞳孔等大、等圆,直径约为3 mm,对光反射灵敏,眼球各向活动自如;双上肢肌力5级、左下肢3级、右下肢4级,四肢肌张力均正常;双上肢腱反射正常,双下肢强阳性,双侧Babinski征阳性;双侧T8水平以下浅感觉减退,双侧髂前上棘以下音叉振动觉减退,四肢共济运动稳准。
辅助检查实验室检查各项指标均于正常值范围。影像学检查:脊椎MRI显示,T5~7水平脊髓后方硬脊膜外团块状T1WI等信号和T2WI稍低信号影,T6~7水平附件区T1WI稍短信号和T2WI异常信号影,增强扫描病灶呈不均匀明显强化,与周围组织界限清晰,硬脊膜受压向前移位(图1)。18F-脱氧葡萄糖(18F-FDG)PET显示,T6~7骨质破坏,葡萄糖代谢异常增高。
诊断与治疗经过临床诊断为脊柱占位性病变。遂于全身麻醉下行胸椎占位性病变切除术。术中可见T6棘突和椎板以及部分T5、T7棘突和椎板被侵蚀,骨皮质呈虫蚀样改变,病变位于椎管内硬脊膜外,血供丰富,呈骨疏松样结构,浸润T6棘突和椎板、部分T5棘突和椎板、T7上部椎板,硬脊膜完整。手术全切除肿瘤及邻近骨组织,切除标本行组织病理学检查。(1)大体标本观察:手术切除组织包括灰白色破碎组织1块,大小约为25 mm×20 mm× 10 mm,质地中等,血供丰富;灰白色骨组织数块,大小约为70 mm×30 mm×15 mm,质地较硬。经体积分数10%的中性甲醛溶液固定,常规脱水、石蜡包埋,制备5 μm层厚组织切片,行HE染色和免疫组织化学染色。(2)HE染色:肿瘤细胞以密集排列的小细胞为主,呈灶性浆细胞样细胞分化,其间可见片状粉染物质沉积,并多见人工裂纹和散在分布的多核巨细胞(图2)。(3)免疫组织化学染色:采用ABC三步法,检测用试剂盒购自丹麦Dako公司;检测用抗体包括CD138、CD38、波形蛋白(Vim)、白细胞共同抗原(LCA)、免疫球蛋白κ轻链和λ轻链、CD99、S-100蛋白(S-100)、广谱细胞角蛋白(PCK)、上皮膜抗原(EMA)、黑色素瘤相关抗原HMB45、CD34和Ki-67抗原购自丹麦Dako公司(均为即用型抗体)。结果显示,肿瘤细胞胞质CD138(图3a)、CD38(图3b)和Vim(图3c)呈弥漫性阳性,LCA呈散在阳性,免疫球蛋白κ轻链和λ轻链、CD99、S-100、 PCK、EMA、HMB45、CD34均呈阴性,Ki-67抗原标记指数约为1.25%(图3d)。(4)特殊染色:肿瘤细胞间片状粉染物质刚果红染色呈棕红色(图4)。(5)原位杂交检测:免疫球蛋白κ轻链DNA含量高于λ轻链。最终病理诊断为(脊柱)浆细胞瘤伴淀粉样变性。患者共住院25 d,出院后于外院辅助术后药物化疗(具体方案不详),定期复查脊椎MRI,未见肿瘤复发或转移。
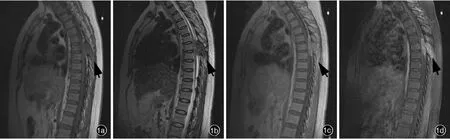
图1 脊椎MRI检查所见1a矢状位T1WI显示,T5~7水平脊髓后方硬脊膜外团块状等信号影,T6~7水平附件内等信号影(箭头所示)1b矢状位T2WI显示,T5~7水平脊髓后方硬脊膜外团块状低信号影,T6~7水平附件内稍低信号影(箭头所示)1c矢状位增强T1WI显示,肿瘤呈不均匀明显强化(箭头所示),边界清楚,硬脊膜受压向前移位1d矢状位抑脂增强T1WI显示,肿瘤呈不均匀明显强化,病变范围更清晰(箭头所示)Figure 1 Spinal MRI findings Sagittal T1WI showed iso-intensity signal of an irregular mass behind the spinal cord at T5-7level and within T6-7vertebral body accessory(arrow indicates,Panel 1a).Sagittal T2WI showed low-intensity signal of an irregular mass behind the spinal cord at T5-7level and within T6-7vertebral body accessory(arrow indicates,Panel 1b).Sagittal enhanced T1WI revealed obvious heterogeneous enhancement(arrow indicates).The border was clear and spinal dura mater was compressed to shift forward (Panel 1c).Sagittal enhanced fat-suppressed T1WI revealed irregular enhancement and the lesion was clearer(arrow indicates,Panel 1d).



图2 光学显微镜观察所见HE染色2a肿瘤细胞以密集排列的小细胞为主,其间可见片状粉染物质沉积× 100 2b粉染物质区域多见人工裂纹和散在分布的多核巨细胞×200 2c肿瘤细胞密度增加,有一定异型性,可见灶性浆细胞样细胞分化×400Figure 2 Optical microscopy findings HE staining Tumor cells were composed of intensive small cells.Flake pink staining substance was among them(Panel 2a).× 100 Artificial cracks were common and multinuclear giant tumor cells were scatteredly distributed in the pink staining substance area(Panel 2b).×200 Tumor cells showed increased density and atypia,and plasmacytoid cells were seen in some area(Panel 2c).×400





图3 光学显微镜观察所见免疫组织化学染色(ABC三步法)×400 3a肿瘤细胞胞质弥漫性表达CD138 3b肿瘤细胞胞质弥漫性表达CD38 3c肿瘤细胞胞质弥漫性表达Vim 3d肿瘤细胞Ki-67抗原标记指数约为1.25%图4光学显微镜观察显示,粉染物质呈棕红色刚果红染色×200Figure 3 Optical microscopy findings Immunohistochemical staining(ABC)×400 Cytoplasm of tumor cells were diffusely positive for CD138(Panel 3a). Cytoplasm of tumor cells were diffusely positive for CD38 (Panel 3b).Cytoplasm of tumor cells were diffusely positive for Vim(Panel 3c).Ki-67 labeling index of tumor cells was 1.25%(Panel 3d).Figure 4 Optical microscopy showed the pink staining substance was brownish red.Congo red staining×200
讨论
孤立性浆细胞瘤起源于骨骼,好发于中轴骨,或骨外组织如头颈部。有25%~70%的孤立性浆细胞瘤患者血清或尿液中可以检出免疫球蛋白M(IgM),而在髓外呈低表达,但可以通过检测免疫球蛋白游离轻链以提高其阳性检出率。脊柱孤立性浆细胞瘤的平均发病年龄约为55岁,男女比例2∶1,多累及椎体,临床主要表现为逐渐加重的病变椎体周围疼痛,如果压迫神经,则可出现神经受累症状与体征[1-4]。因此,对于脊椎及其周围疼痛,应重视早期检查,特别是脊椎MRI检查,有助于早期诊断,防止严重的脊柱脊髓损害。
淀粉样变性系β片层结构的淀粉样纤维沉积于细胞外导致的疾病,此类物质与碘和硫酸接触后发生颜色反应与淀粉相似,故命名为淀粉样变性并沿用至今[5]。淀粉样变性可发生于全身多器官和组织,发病率较低,可以存在单独的病理改变,也可以伴恶性淋巴瘤、浆细胞肉芽肿等全身淀粉样变性的一部分。淀粉样变性多继发于多发性骨髓瘤,而其他B细胞肿瘤如淋巴瘤、白血病等均可并发淀粉样变性,此类疾病可发生异常分泌性免疫球蛋白重链或轻链沉积,从而导致淀粉样变性[6]。组织活检时淀粉样变性组织有一定硬度。大体标本观察,肿瘤组织大小不等,呈均匀致密排列,半透明,无包膜。组织学形态观察,粉染物质呈无细胞,同质,均匀,红色,片状、团块状或网格状弥漫性分布于细胞外基质(ECM)。特异性诊断依据组织活检术以及粉染物质免疫组织化学染色和特殊染色。其中,特殊染色粉染物质刚果红染色呈棕红色,是诊断淀粉样变性经典的特异性标记[5]。
脊柱孤立性浆细胞瘤伴淀粉样变性的明确诊断仍依靠组织病理学检查,结合组织学形态和免疫表型不难作出诊断。鉴别诊断包括:(1)骨肉瘤。肿瘤细胞和肿瘤性成骨可资鉴别。(2)脊柱转移瘤。根据组织学形态、免疫表型和PET-CT显像可以排除诊断。(3)大细胞淋巴瘤。组织学形态和免疫表型可资鉴别。
孤立性浆细胞瘤患者中位生存期为7.50~12.00年,发生于脊柱者的生存期尚未见文献报道。何妙侠等[7]报告13例脊柱孤立性浆细胞瘤患者,认为其预后影响因素包括年龄、肿瘤部位和大小、肿瘤细胞分化程度、手术时机、局部手术范围是否彻底和病灶处理方法等,长期随访观察尤为重要。但此方面的随访资料目前较少见诸文献报道,尚待大样本的临床研究进行长期观察总结。
[1]Mirzashahi B,Mazoochy H,Jamnani RK,Farzan A.Contribution of surgery in solitary plasmacytoma of spine:a case report.Arch Bone Jt Surg,2014,2:121-125.
[2]Tsutsumi S,Yasumoto Y,Ito M.Solitary spinal extradural plasmacytoma:a case report and literature review.Clin Neuroradiol,2013,23:5-9.
[3]Soutar R,Lucraft H,Jackson G,Reece A,Bird J,Low E,Samson D;Guidelines Working Group of the UK Myeloma Forum;British Committee for Standards in Haematology;British Society for Haematology.Guidelines on the diagnosis and management of solitary plasmacytoma of bone and solitary extramedullary plasmacytoma.Br J Haematol,2004,124:717-726.
[4]Knobel D,Zouhair A,Tsang RW,Poortmans P,Belkacémi Y, Bolla M,Oner FD,Landmann C,Castelain B,Ozsahin M;Rare Cancer Network.Prognostic factors in solitary plasmacytoma of the bone:a multicenter Rare Cancer Network study.BMC Cancer, 2006,6:118.
[5]Jaffe ES,Harris NL,Stein H,Vardiman JW.WHO classification of tumours:pathology and genetics of tumours of hematopoietic and lymphoid tissues.Lyon:IARC Press,2001:148-150.
[6]Lavatelli F,Vrana JA.Proteomic typing of amyloid deposits in systemic amyloidoses.Amyloid,2011,18:177-182.
[7]He MX,Zhu MH,Zhang YM,Fu QG,Wu LL.Solitary plasmacytoma of spine:a clinical,radiologic and pathologic study of 13 cases.Zhonghua Bing Li Xue Za Zhi,2009,38:307-311[.何妙侠,朱明华,张亚明,傅青格,吴丽莉.脊柱孤立性浆细胞瘤的临床病理分析.中华病理学杂志,2009,38:307-311.]
Solitary plasmacytoma of spine with amyloidosis
SUN Cui-yun,YU Shi-zhu
Tianjin Medical University General Hospital;Tianjin Neurological Institute;Tianjin Key Laboratory of Injury, Variation and Regeneration of Nervous System;Key Laboratory of Post-trauma Neuro-repair and Regeneration in Central Nervous System,Ministry of Education,Tianjin 300052,China
< class="emphasis_italic">Corresponding author:YU Shi
YU Shi-zhu(Email:tjyushizhu@yahoo.com)
ObjectiveTo report the diagnosis and treatment of one case of solitary plasmacytoma of spine with amyloidosis and investigate the clinicopathological features combined with literatures.Methods and ResultsThe patient was a 46-year-old woman.She suffered from weakness of both lower limbs,unsteady gait and numbness of toes for 20 d.MRI examination revealed an irregular mass behind the spinal cord at T5-7level and T6-7vertebral body accessory.The enhanced MRI showed obvious heterogeneous enhancement.The border was clear and spinal dura mater was compressed to shift forward. During operation,T5-7processus spinosus and vertebral laminae were eroded,and the cortex of bone showed "moth-eaten"erosion.The intraspinal and extradural lesion had rich blood supply,loose bone structure and intact spinal dura mater.Histologically,tumor cells were composed of intensive small cells,and focal plasmacytoid cells were seen.Flake pink staining substance was among them.Artificial cracks were common and multinuclear giant tumor cells were scatteredly distributed.Immunohistochemical analysis showed the cytoplasm of tumor cells were diffusely positive for CD138,CD38 and vimentin(Vim),scatteredly positive for leukocyte common antigen(LCA),and negative for immune globulin κ light chain (IgGκ)and λ light chain(IgGλ),CD99,S-100 protein(S-100),pan cytokeratin(PCK),epithelial membrane antigen(EMA),HMB45 and CD34.The Ki-67 labeling index was 1.25%.Congo red staining showed the pink staining substance was brownish red.Hybridization in situ examination showed the DNA content of Ig Gκ was more than that of Ig Gλ.The final pathological diagnosis was solitary plasmacytoma of spine with amyloidosis.The patient was treated with postoperative chemotherapy,and there was no recurrence or metastasis during 18-month follow-up period.ConclusionsSolitary plasmacytoma of spine with amyloidosis is a rare tumor.The imaging features can offer a few diagnostic cues.However,a clear diagnosis depends on specific histomorphology,immunophenotyping,special staining and hybridization in situ examination.
Plasmacytoma;Amyloidosis;Spine;Immunohistochemistry;In situ hybridization;Pathology
2016-12-09)
10.3969/j.issn.1672-6731.2017.01.010
国家自然科学基金资助项目(项目编号:81402050);国家自然科学基金资助项目(项目编号:81502166);天津市应用基础及前沿技术研究计划项目(项目编号:15JCZDJC34600);天津市应用基础及前沿技术研究计划项目(项目编号:15JCYBJC49900);天津市自然科学基金青年科学基金资助项目(项目编号:16JCQNJC13400);天津医科大学青年科学基金资助项目(项目编号:2015KYZQ11);天津医科大学总医院青年孵育基金资助项目(项目编号:ZYYFY2014038);天津医科大学总医院青年孵育基金资助项目(项目编号:ZYYFY2015032)
300052天津医科大学总医院天津市神经病学研究所天津市神经损伤变异与再生重点实验室教育部中枢创伤修复与再生重点实验室
于士柱(Email:tjyushizhu@yahoo.com)
猜你喜欢
安徽医科大学学报(2022年6期)2022-07-13 09:49:50
中国典型病例大全(2022年10期)2022-05-10 21:24:29
实用骨科杂志(2020年4期)2020-12-26 09:10:28
国际呼吸杂志(2019年4期)2019-03-12 01:07:54
国际呼吸杂志(2019年1期)2019-01-28 09:37:00
武警医学(2018年10期)2018-11-06 07:04:40
解剖学杂志(2018年4期)2018-10-11 06:51:04
医药前沿(2018年22期)2018-01-17 12:32:39
郑州大学学报(医学版)(2015年2期)2015-02-27 14:50:43
解放军医学杂志(2013年4期)2013-02-20 00:38:32