
血清CA125联合超声评分对卵巢良恶性肿瘤的鉴别价值
2017-03-08 11:00:44刘爱华
实用癌症杂志 2017年2期
刘爱华
血清CA125联合超声评分对卵巢良恶性肿瘤的鉴别价值
刘爱华
目的 研究血清CA125联合超声评分鉴别卵巢良恶性肿瘤的价值。方法 选择卵巢肿瘤患者200例,108例卵巢良性肿瘤患者为良性组,92例卵巢恶性肿瘤患者为恶性组,于术前一周行腹部超声联合阴道超声检查,进行Finkler超声评分,同时空腹抽取静脉血检测血清CA125水平。结果 恶性组的Finkler评分和阳性率均明显高于良性组(P<0.05);恶性组的CA125水平和阳性率均明显高于良性组(P<0.05);Finkler评分联合CA125的特异度、敏感度、阴性预测值和阳性预测值均高于单一检测(P<0.05);Finkler评分联合CA125对Ⅰ~Ⅱ期卵巢癌的诊断阳性率明显高于单一检测方法(P<0.05),而对Ⅲ~Ⅳ期的诊断阳性率无明显差异(P>0.05)。结论 血清CA125联合超声评分鉴别卵巢良恶性肿瘤具有较高的特异度和敏感度,优于单一检测方法,且对Ⅰ~Ⅱ期即早期卵巢癌具有更高的诊断价值。
CA125;超声评分;卵巢肿瘤
(ThePracticalJournalofCancer,2017,32:324~326)
卵巢肿瘤是常见的女性生殖系统肿瘤,在妇科卵巢癌的发病率仅次于乳腺癌,其死亡率甚至高于宫颈癌和子宫内膜癌[1]。CA125作为临床常用的肿瘤标志物,是国际上一致公认的卵巢癌主要相关抗原,但近年来众多研究发现,在多种良恶性肿瘤中CA125水平也会有所升高[2-3]。超声检查凭借其无创、费用低、简单方便的优势,逐渐成为卵巢肿瘤的常规鉴别诊断方法[4]。本研究主要探讨了血清CA125联合超声评分鉴别卵巢良恶性肿瘤的价值,以寻求1种特异性和敏感性均高的诊断方法,提高术前诊断水平。
1 资料与方法
1.1 一般资料
200例卵巢肿瘤患者来自我院2012年2月至2015年12月,108例卵巢良性肿瘤患者为良性组,年龄19~72岁,平均(37.92±6.43)岁;黏液性囊腺瘤61例,浆液性囊腺瘤47例;92例卵巢恶性肿瘤患者为恶性组,年龄22~76岁,平均(45.12±5.63)岁;黏液性囊腺癌9例,浆液性囊腺癌58例,透明细胞癌8例,子宫内膜样癌17例;病理分期Ⅰ~Ⅱ期(早期)58例,Ⅲ~Ⅳ期(晚期)34例。本研究获得我院伦理委员会的批准,所有患者均签署知情同意书。
1.2 方法
应用美国ATL超 9型超声诊断仪进行盆腔彩色超声检查,阴道超声的探头频率为7.5 MHz,腹部超声的探头频率为3.5 MHz。观察肿瘤的大小、形态、血流、边界、内部回声、有无腹腔积液和转移、包膜情况。Finkler超声评分:① 1分:无回声,肿瘤边界清楚,结节性囊或肿纤维瘤;② 2分:低回声或无回声,边界稍微不规则;③3分:低回声,边界不规则,无结节;④ 4~6分:中等回声,实性卵巢增大,边界不规则;⑤ 7~9分:肿瘤为不规则或多分隔的囊性肿物;⑥10分:上述特征均出现并伴有腹腔积液。Finkler评分≥7分为阳性界定值标准,即卵巢良性肿瘤Finkler评分<7分,卵巢恶性肿瘤 Finkler评分≥7分。
空腹抽取3 mL静脉血,采用化学发光法检测血清CA125水平,把 CA125≥35 IU/ml为阳性界定值标准,即卵巢良性肿瘤CA125<35 IU/ml,卵巢恶性肿瘤CA125≥35 IU/ml。
1.3 统计学分析
2 结果
2.1 两组Finkler评分和检出阳性率对比
恶性组的Finkler评分和检出阳性率均明显高于良性组(P<0.05),见表1。
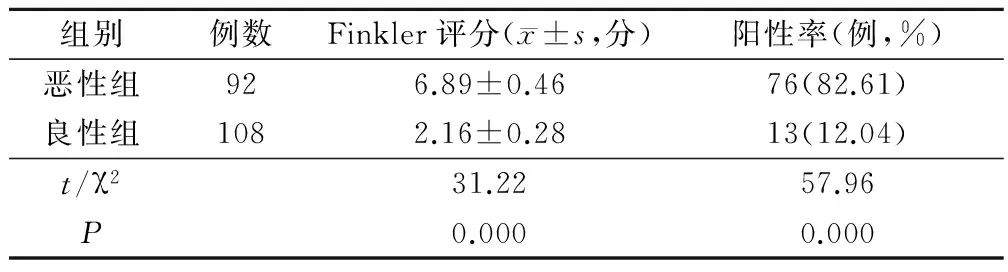
表1 两组Finkler评分和检出阳性率对比
2.2 两组CA125水平和检出阳性率对比
恶性组的CA125水平和检出阳性率均明显高于良性组(P<0.05),见表2。

表2 两组CA125水平和检出阳性率对比
2.3 Finkler评分联合CA125的诊断价值
以病理检查结果(108例良性暖巢囊肿和92例恶性暖巢囊肿)为金标准,经统计分析得出,Finkler评分联合CA125的特异度、敏感度、阴性预测值和阳性预测值均高于单一检测(P<0.05),见表3。

表3 Finkler评分联合CA125的诊断价值/%
2.4 Finkler评分联合CA125对不同病理分期卵巢癌的诊断阳性情况比较
Finkler评分联合CA125对Ⅰ~Ⅱ期卵巢癌的诊断阳性率明显高于单一检测方法(P<0.05),而对Ⅲ~Ⅳ期患者的诊断阳性率无明显差异(P>0.05),见表4。

表4 Finkler评分联合CA125对不同病理分期 卵巢癌患者的诊断情况比较(例,%)
3 讨论
卵巢肿瘤是妇科常见病,由于卵巢位于子宫底的后外侧,处于盆腔深部,且早期症状较为隐匿,缺乏特异性症状,这就加大了鉴别其良恶性的难度,大部分卵巢癌患者就诊时已经到了晚期,使治疗效果并不理想,晚期卵巢癌患者的5年生存率仅为20%~30%[5-6]。因此,早期诊断是提高治疗效果,改善预后,提高生存率的关键。CA125是食品药品监督管理局批准的首个卵巢癌生物标记物[7]。但单一肿瘤标记物的器官特异性尚有限,CA125 水平的升高并不是卵巢恶性肿瘤所特有,如卵巢过度刺激综合征、子宫内膜异位囊肿、盆腔炎、妊娠等非卵巢恶性肿瘤也会出现假性升高,单独检查CA125并不能用于卵巢癌的早期筛查和早期诊断[8-9]。超声是检查卵巢肿瘤血供情况最为常用的检测手段,能显示出肿瘤内部的血流方向、血管分布情况和血流速度等信息[10]。由于恶性肿瘤生长速度快,新生血管较良性肿瘤多,在肿瘤实质内或其周围会显示出更为广泛、高流速的血流信号,以此作为鉴别诊断卵巢良恶性肿瘤的根据[11]。
本研究主要探讨了血清CA125联合超声评分鉴别卵巢良恶性肿瘤的价值,结果发现, Finkler评分联合CA125的特异度、敏感度、阴性预测值和阳性预测值均高于单一检测(P<0.05);Burak等[12]研究发现,应用年龄联合超声检查和CA125进行术前评估能准确地鉴别卵巢良性和恶性肿瘤,与本文结果相一致。提示超声联合血清肿瘤标志物CA125检测可提高卵巢良恶性肿瘤鉴别诊断的特异度和敏感度,可为临床早期干预争取时间,这对于手术方式的选择和手术效果的估计有重要的临床意义。虽然临床上已有关于超声联合血清肿瘤标志物诊断卵巢良恶性肿瘤的相关报道,但尚未见联合检测对卵巢癌不同病理分期诊断价值的报道。本研究发现,Finkler评分联合CA125对Ⅰ~Ⅱ期卵巢癌的诊断阳性率明显高于单一检测方法(P<0.05),而对Ⅲ~Ⅳ期的诊断阳性率无明显差异(P>0.05);提示联合检测对Ⅰ~Ⅱ期即早期卵巢癌具有较高的诊断价值,可为初诊卵巢疾病患者提供重要的临床依据。
综上所述,血清CA125联合超声评分鉴别卵巢良恶性肿瘤具有较高的特异度和敏感度,优于单一检测方法,且对Ⅰ~Ⅱ期即早期卵巢癌具有更高的诊断价值。
[1] 胡春秀.青少年卵巢肿瘤47例临床诊治分析〔J〕.安徽医学,2011,32(5):596-598.
[2] Nakagawa N,Koda H,Nitta N,et al.Reactivity of CA19-9 and CA125 in histological subtypes of epithelial ovarian tumors and ovarian endometriosis〔J〕.Acta Medica Okayama,2015,69(4):227-35.
[3] 曹玉萍,张丽萍,刘学公,等.1716例健康体检者血清CA125结果分析〔J〕.安徽医学,2011,32(10):1710-1711.
[4] Kim JS,Park SN,Kim BR.Recurrent ovarian steroid cell tumor,not otherwise specified managed with debulking surgery,radiofrequency ablation,and adjuvant chemotherapy〔J〕.Obstet Gynecol Sci,2014,57(6):534-538.
[5] Sung PL,Chang YH,Chao KC,et al.Global distribution pattern of histological subtypes of epithelial ovarian cancer:a database analysis and systematic review〔J〕.Gynecol Oncol,2014,133(2):147-154.
[6] Brodsky AS,Fischer A,Miller DH,et al.Expression profiling of primary and metastatic ovarian tumors reveals differences indicative of aggressive disease〔J〕.Plos One,2014,9(4):e94476.
[7] Ritva N,Anne TM,Paula K,et al.Claudin-5 Is Associated with Elevated TATI and CA125 Levels in Mucinous Ovarian Borderline Tumors〔J〕.Anticancer Res,2015,35(2):973-976.
[8] Braicu EI,Gorp TV,Nassir M,et al.Preoperative HE4 and ROMA values do not improve the CA125 diagnostic value for borderline tumors of the ovary (BOT) -A study of the TOC Consortium〔J〕.J Ovarian Res,2014,7:49.
[10] Quiroz AN,Cadet MA,Doyle TE.High-frequency ultrasonic measurement of vascularization in phantoms and Avastin-treated mice with breast tumors〔J〕.J Acoust Soc Am,2014,135(4):2180.
[11] Wladis EJ,Kenning TJ.Cavitron ultrasonic surgical aspirator-assisted resection of combined orbital and intracranial tumors〔J〕.Orbit,2014,33(3):234-235.
[12] Burak K,Kocak M,Kayikcioglu F,et al.Risk for malignant and borderline ovarian neoplasms following basic preoperative evaluation by ultrasonography,ca125 level and age〔J〕.Asian Pac J Cancer Prev,2014,15(19):8489-8493.
(编辑:吴小红)
The Value of the Serum CA125 Combined with Ultrasound Scoring in the Differential Diagnosis of Benign and Malignant Ovary Tumor
LIUAihua.
Hai’anHospitalAffiliatedtoNantongUniversity,Nantong,226600
Objective To investigate the value of the serum CA125 combined with ultrasound scoring in the differential diagnosis of benign and malignant ovary tumor.Methods 200 cases of ovarian tumors were selected,including 108 cases of benign tumors (benign group),and 92 cases of malignant tumors(malignant group).All patients underwent abdominal ultrasound combined with transvaginal ultrasound.The contrast of Finkler ultrasound scores and serum CA125 level were made.Results The ultrasound scores and positive rate,serum CA125 level and positive rate of the malignant group were significantly higher than those of the benign group(P<0.05);Sensitivity,specificity,positive and negativepredictive values of Finkler ultrasound scores combined with serum CA125 were all significantly higher than single test (P<0.05);diagnostic positive rate of Finkler ultrasound scores combined with serum CA125 for stage Ⅰ~Ⅱovarian cancer were significantly higher than single test (P<0.05),but there had no significant difference for stageⅢ~Ⅳovarian cancer(P>0.05).Conclusion Ultrasound scores combined with serum CA125 in the differential diagnosis of benign and malignant ovary tumor have higher sensitivity and specificity,it is better than single test,and has higher diagnostic value in the diagnosis of stage Ⅰ~Ⅱovarian cancer.
CA125;Ultrasound scores;Ovary tumour
226600 南通大学附属海安医院
10.3969/j.issn.1001-5930.2017.02.046
R73-36
A
1001-5930(2017)02-0324-03
2016-04-01
2016-11-04)
猜你喜欢
中老年保健(2022年6期)2022-08-19 01:41:22
云南医药(2021年3期)2021-07-21 05:41:06
内蒙古林业(2021年6期)2021-06-26 10:42:32
家庭医学(下半月)(2020年2期)2020-05-11 02:07:26
中国临床医学影像杂志(2019年5期)2019-08-27 02:48:00
安徽医科大学学报(2016年12期)2017-01-15 14:21:54
中国卫生(2016年9期)2016-11-12 13:28:08
中国继续医学教育(2015年1期)2016-01-06 01:36:04
分子影像学杂志(2015年3期)2015-12-04 03:29:02
医学研究杂志(2015年4期)2015-06-10 06:42:43
