
Cardiopulmonary resuscitation knowledge and attitude among general dentists in Kuwait
2017-02-10 10:46SarahAlkandariLolwaAlyahyaMohammedAbdulwahab
Sarah A. Alkandari,Lolwa Alyahya,Mohammed Abdulwahab
1Dental Division, Farwaniya Health District, Ministry of Health, Kuwait
2Department of Surgical Sciences, Faculty of Dentistry, Kuwait University, Safat, Kuwait
Cardiopulmonary resuscitation knowledge and attitude among general dentists in Kuwait
Sarah A. Alkandari,1Lolwa Alyahya,1Mohammed Abdulwahab2
1Dental Division, Farwaniya Health District, Ministry of Health, Kuwait
2Department of Surgical Sciences, Faculty of Dentistry, Kuwait University, Safat, Kuwait
BACKGROUND: Dentists as health care providers should maintain a competence in resuscitation. This cannot be overemphasized by the fact that the population in our country is living longer with an increasing proportion of medically compromised persons in the general population. This preliminary study aimed to assess the knowledge and attitude of general dentists towards cardiopulmonary resuscitation (CPR).
METHODS: A cross-sectional study was carried out among 250 licensed general dental practitioners working in ministry of health. Data were obtained through electronic self-administered questionnaire consisting of demographic data of general dentists, and their experience, attitude and knowledge about CPR based on the 2010 American Heart Association guidelines update for CPR.
RESULTS: Totally 208 general dentists took part in the present study giving a response rate of 83.2%. Only 36% of the participants demonstrated high knowledge on CPR, while 64% demonstrated low knowledge. Participants' age, gender, nationality, years of experience, career hierarchy, and formal CPR training were associated significantly with CPR knowledge. Almost all the participants (99%) felt that dentists needed to be competent in basic resuscitation skills and showed a positive attitude towards attending continuing dental educational programs on CPR.
CONCLUSION: This study showed that majority of general dental practitioners in Kuwait had inadequate knowledge on CPR. It was also found that CPR training signif cantly inf uenced the CPR knowledge of the participants. Therefore, training courses on CPR should be regularly provided to general dentists in the country.
Cardiopulmonary resuscitation; Knowledge; Attitude; General dentists
INTRODUCTION
Heart disease is one of the most common diseases worldwide causing high morbidity rate and high healthcare expense.[1–3]Cardiac arrest is a common etiology of mortality in developed countries.[4]According to the American heart association (AHA), Cardiac arrest is defined as: "the cessation of cardiac mechanical activity, conf rmed by the absence of a detectable pulse, unresponsiveness, and apnea".[5]Most individuals suffering from cardiac arrest die before reaching the hospital.[6]Thus, immediate intervention in terms of performing cardiopulmonary resuscitation (CPR) is critical for increasing chances of patient's survival until emergency personnel arrive.[6]Cardiac arrest patients who are resuscitated immediately have higher survival rate compared to those who did not receive immediate CPR (8.2% vs. 2.5% respectively).[7]CPR is an "emergency procedure performed as an attempt to restore spontaneous circulation by performing chest compressions with or without ventilations".[8]
Though uncommon, incidence of cardiac arrest in dental clinics have been reported.[9–12]In 1991, Hunter[9]published the f rst report of such emergency in the dental surgery. Another study,[10]which was conducted in 2001, demonstrated that the incidence of cardiac arrest for every 133 physicians' and dentists' practices in the United States was ranging between 0.008 to 1 cardiac arrest per year. A similar study[11]showed that the annual incidence of cardiac arrest per dentist in UK was 0.002. Moreover, Champman[12]estimated that approximately 1 in 7 Australian dentists will encounter a resuscitation emergency in his or her career.
Although resuscitation emergencies are relatively unusual in dental practice, dentists, as health care providers, should be competent in performing CPR if required. Only few publications[13–15]about the competence of dentists to deal with such medical emergency are available, and none has been published in Kuwait. One study,[14]which was conducted in 2015, concluded that only 3.75% of general dentists in Iran were able to perform CPR correctly. Another study[13]showed that almost two-thirds of Australian dentists felt they were competent in performing CPR, although less than two-thirds had received practical training in CPR since graduation. Furthermore, in 2003 Gonzaga et al[15]found that half of dental practitioners in Brazil believed themselves able to perform CPR, however, none of them referred to have undertaken resuscitation training.
The objectives of the present preliminary crosssectional study are to assess the level of knowledge and attitude towards CPR among general dentists in Kuwait, and to ascertain any relationship with subjects' demographic characteristics. After this study, we hope that formal training courses on CPR will be planned and regularly provided in order to improve and standardize all aspects of CPR skills among general dental practitioners in the country.
METHODS
Study design
A cross sectional survey was carried out from November 2015 to February 2016 in 5 health districts in Kuwait (all health districts in Kuwait at the time of the study).
Study participants
General dental practitioners who have a valid dental license and work in ministry of health were included in this study. Those who were on leave or unwilling to participate were excluded from the study.
Study instrument
A self-administered, structured questionnaire was prepared by the authors. The questionnaire consisted of 23 questions about the following independent variables: (1) demographic data such as age, gender, nationality, health district, years of dental practice and career hierarchy; (2) CPR training and attitude; and (3) knowledge and experience about cardiac arrest and CPR. The latest American Heart Association (AHA) update for CPR guidelines has been published in 2015. Though, for the purpose of this research, the dentists' knowledge was assessed by means of the information which are presented in the 2010 update. A pilot survey was conducted among 15 general dental practitioners to determine the validity of the questionnaire. Subjects in the pilot study were excluded from the main study sample.
Ethical considerations
This study was approved by the ethical committee of the ministry of health in Kuwait (research project number: 264/2015), and has been carried out in full accordance with the World Medical Association Declaration of Helsinki. The permission to conduct the study was obtained from the head of the dental services unit of each health district. Neither the name nor the contact information of the dentists were involved in the questionnaire, thus the participants' confidentiality was maintained. All participants received written information about the nature and purposes of the study and an electronic written informed consent was obtained from each subject upon their approval to participate.
Data collection
A total of 250 electronic copies of the study questionnaire were sent, through text massages, to a random sample of general dental practitioners in Kuwait. Dentists' contact information was obtained from the head of the dental services unit of each health district. Completed surveys only were permitted to be submitted and each participant was allowed to submit his/her response once only.
Data analysis
Statistical Package for Social Sciences Software (SPSS), version 22, was used for data analysis. Descriptive statistics were presented using frequency, percentage, mean±standard deviation (SD), and range. Regarding the knowledge score, each positive response was assigned as a score of '1' and each negative response was given a score of '0'. The individual scores were summed upto yield a total score with a possible maximum score of '8', where a score of 0–3 indicates a low knowledge and a score of 4–8 was considered as a high knowledge. Also, Pearson's Chi-square test was used to assess the association of different demographic characteristics with dentists' knowledge. A critical probability value (Pvalue) of <0.05 was used as the cut-off level for statistical signif cance.
RESULTS
Participants
Totally 208 general dental practitioners completed the survey, with a response rate of 83.2%. Demographic data of the participants are demonstrated in Table 1. Dentists' mean age was 32.8 years, ranging between 23 to 64 years. Among all the participants, 123 (59.1%) were males and 85 (40.9%) were females. Most of the participants were Kuwaitis (73.1%). In addition, majority of the dentists (26.0%) were working in Hawalli health district, while the minority (14.4%) was working in Jahra health district. The duration of clinical experience was divided into less than 5 years, 5–10 years and more than 10 years, which comprised of 110 (52.9%), 63 (30.3%) and 35 (16.8%) participants respectively. Most general dentists in this study were assistant registrars (52.4%).
Descriptive f ndings
Table 2 summarizes the respondent dentists' experience and attitude towards CPR. More than halfof the dentists (57.2%) in the current study stated that they were competent in performing CPR. However, dentists who did not receive formal CPR training within the last 2 years (63.9%) significantly outnumber those who did (36.1%). Figure 1 demonstrates the types of CPR training respondents received. Moreover, majority of the subjects (97.6%) reported that they take and/ or update the medical history of their patients before starting the dental treatment and only 4.3% have seen patients suffering from cardiac arrest in their practice. Almost all the general dental practitioners (99%) in the present study felt that dentists should be competent in basic resuscitation skills and showed a positive response regarding attending continuing dental educational programs on CPR.
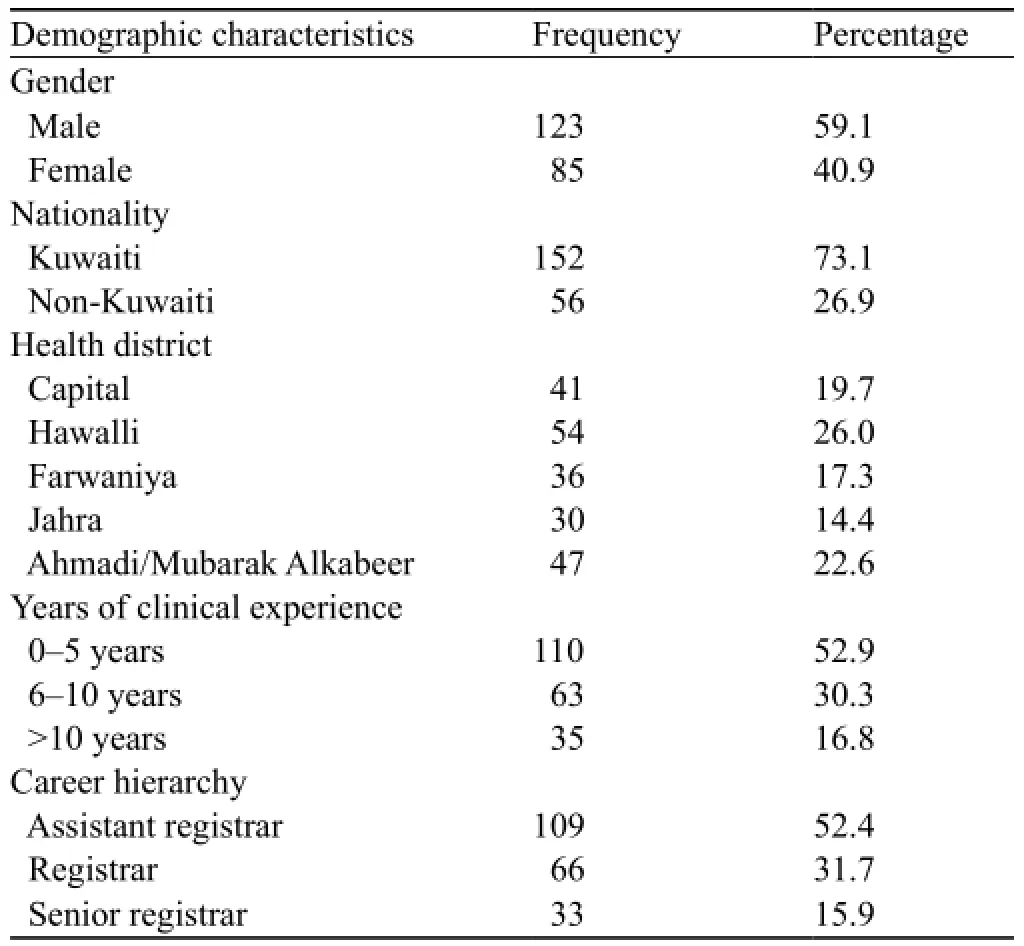
Table 1. Demographic characteristics of the participants
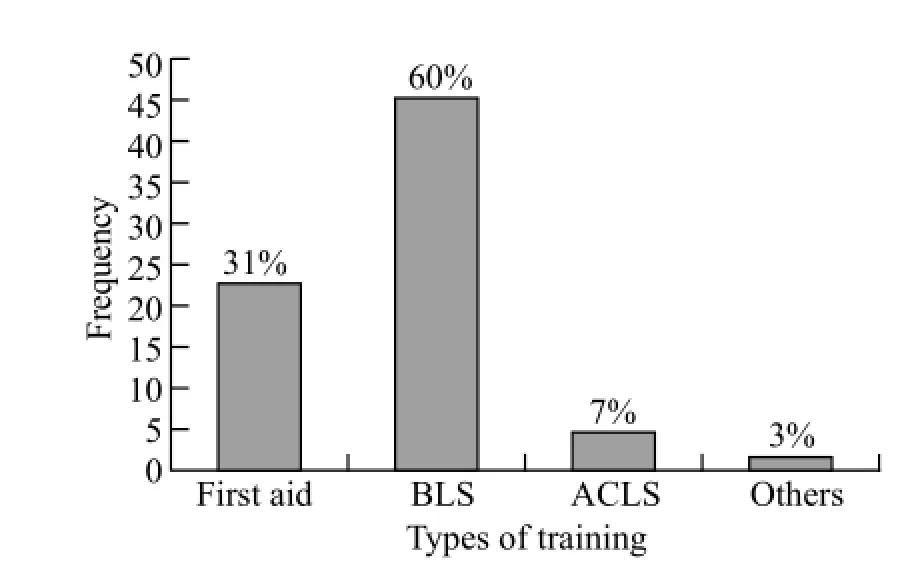
Figure 1. Types of training among participants who received CPR training within the last 2 years (n=75).

Table 2. Attitude and experience of the participants towards cardiopulmonary resuscitation (CPR)
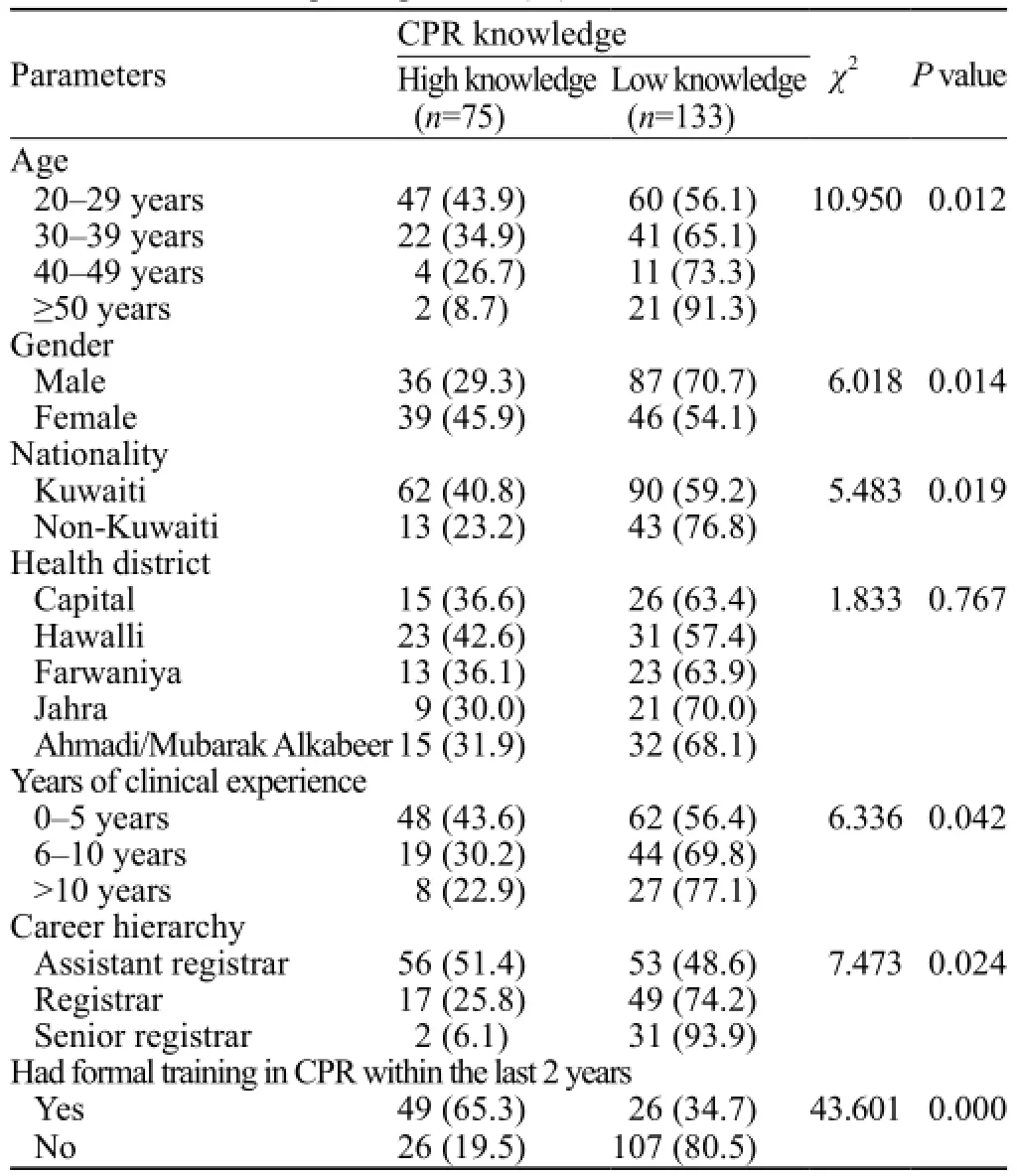
Table 4. Correlation of the CPR knowledge in relation to the different characteristics of the participants,n(%)
Concerning CPR knowledge, the mean score for the participants was 4.07 with a median score of 4, ranged 0 to 8 for 8 questions. Only 36% of general dentists in this study showed high knowledge in CPR, while 64% demonstrated low knowledge. Frequency and percentage of positive responses to knowledge questions are listed in Table 3.
Correlations
As shown in Table 4, a significant declining trend in CPR knowledge was found with increasing dentist's age (P=0.012). Male dentists had significantly lower scores than female dentists (P=0.014). Nationality had a significant association as Kuwaitis showed higher knowledge scores compared to non-Kuwaitis (P=0.019). Moreover, assistant registrars seemed to have significantly more knowledge about CPR compared to registrars and senior registrars (P=0.024). The participants with less than 5 years' clinical experience had higher knowledge scores in comparison to the more experienced ones, this difference was of statistical signif cant (P=0.042). In addition, the knowledge scores were significantly higher in those who received CPR training within the last 2 years than those who did not (P=0.00). On the contrary, no statistically significant difference was found with regards to the health district.
DISCUSSION
To the best of our knowledge, this is the first research in Kuwait that evaluates the knowledge and attitude towards CPR among general dentists. It was demonstrated by the present study that the general dentists had inadequate CPR knowledge. This finding is in accordance with other studies,[12,14,17,18]which concluded that the knowledge and experience of CPR need to be improved and updated. Only 36% of the participants in this study had proper theoretical knowledge on CPR. Similar results were found by Gonzaga[14]and Kavari[17]for Brazilian and Iranian dentists respectively. Regarding self-judgement in being competent in performing CPR, the f ndings of the current research were similar to the literature,[12,14,17,18]showing an average just above 50%.
When CPR knowledge was correlated with gender, female general dentists had a significantly higher knowledge score than male general dentists. This observation was opposite to what was found in another study[18]conducted among Indian dental practitioners in which males showed higher knowledge score. Moreover, CPR training signif cantly inf uenced the CPR knowledge of the subjects. Those who had received training within the last 2 years obtained higher scores. This was in consistent with the result of Jamalpour's study,[14]which concluded that the level of CPR knowledge and skills of trained dentists were better than those of untrained ones. Interestingly, our study showed that younger aged participants with lower career hierarchy and less than 10 years' clinical experience had significantly higher knowledge scores in comparison to others. On the contrary, it was noticed in other studies[19,20]that subjects with more than 10 years' clinical experience had better CPR knowledge compared to the less experienced ones. This finding overemphasizes the importance of CPR training. In our study, only 36.1% of the general dentists received formal CPR training within the last 2 years. In fact, without sufficient training and practice, the significant amount of theoretical information will be forgotten after 12 months, and after 18 months there will not be any remained adequate practical skills.[21]In addition, as the guidelines are revised and updated, the importance of continuing training cannot be ignored.
Although only 9 out of 208 (4.3%) subjects in this preliminary study reported that they witnessed cardiac arrest in their dental practice, a f nding that is consistent with previous published reports[16,17], this should not be a reason for complacency. Dentists as health care providers should maintain a competence in resuscitation. This cannot be overemphasized by the fact that the population in our country is living longer with an increasing proportion of medically compromised persons in the general population.[21,22]Fortunately, almost all the participants (99%) thought that dental practitioners needed to be competent in performing CPR and showed a positive response towards attending continuing dental educational courses on CPR.
In addition to the potential limitations present in the cross-sectional and electronic survey-based study, other limitations of the current study include: 1) The small sample size that may limit the generalization of the results; 2) Assessing the theoretical knowledge without evaluating the practical training of the participants is insuff cient to assure CPR competence.
CONCLUSION
It was demonstrated by this study that general dental practitioners in Kuwait lack adequate knowledge on CPR, but they showed positive attitudes towards it. It also showed that CPR training significantly influenced the CPR knowledge of the participants. Therefore, training courses on CPR should be regularly provided to general dentists in the country.
Funding:None.
Ethical approval:The study proposal was approved by the ethical committee of the ministry of health in Kuwait (research project number: 264/2015).
Conflicts of interest:The authors declare that there are no conf icts of interest related to the publication of this paper.
Contributors:Alkandari SA proposed and designed the study, collected and interpreted the data, performed the statistical analysis, and wrote the manuscript. Alyahya L contributed to the acquisition and interpretation of data. Abdulwahab M critically revised the manuscript. All authors have read and approved the f nal manuscript.
REFERENCES
1 onow RO, Smaha LA, Smith SC Jr, Mensah GA, Lenfant C. World Heart Day 2002: the international burden of cardiovascular disease: responding to the emerging global epidemic. Circulation. 2002;106(13):1602–5.
2 Murray CJ, Lopez AD. Mortality by cause for eight regions of the world: Global burden of disease study. Lancet. 1997;349(9061):1269–76.
3 Michaud CM, Murray CJ, Bloom BR. Burden of disease—implications for future research. JAMA. 2001;285(5):535–9.
4 Futterman LG, Lemberg L. Cardiopulmonary resuscitation review: Critical role of chest compression. Am J Crit Care. 2005;14(1):81–4.
5 Cummins RO, Chamberlain DA, Abramson NS, Allen M, Baskett PJ, Backer L, et al. Recommended guidelines for uniform reporting of data from out-of-hospital cardiac arrest: The Utstein Style. Circulation. 1991;84(2):960–975.
6 Kleinman ME, Brennan EE, Goldberger ZN, Swor RA, Terry M, Bobrow BJ, et al. Part 5: Adult basic life support and cardiopulmonary resuscitation quality: 2015 American heart association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2015;132(18 Suppl 2): S414–S435.
7 Fredriksson M, Herlitz J, Nichol G. Variations in outcome in studies of out-of-hospital cardiac arrest: A review of studies conforming to the Utstein guidelines. Am J Emerg Med. 2003;2(4): 276–81.
8 Jacobs I, Nadkarni V, Bahr J, Berg RA, Billi JE, Bossaert L, et al. Cardiac arrest and cardiopulmonary resuscitation outcome reports: Update and simplification of the Utstein templates for resuscitation registries. A statement for healthcare professionals from a task force of the international liaison committee on resuscitation (american heart association, european resuscitationcouncil, australian resuscitation council, new zealand resuscitation council, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation councils of southern africa). Circulation. 2004; 110(21):3385–3397.
9 Hunter PL. Cardiac arrest in dental surgery. Br Dent J. 1991;170(8):284.
10 Becker L, Eisenberg M, Fahrenbruch C, Cobb L. Cardiac arrest in medical and dental practices: Implications for automated external defibrillators. Arch Intern Med. 2001; 161(12):1509–1512.
11 Girder NM, Smith DG. Prevalence of emergency events in British dental practice and emergency management skills of British dentists. Resuscitation. 1999;41(2):156–67.
12 Champman PJ. Medical emergencies in dental practice and choice of emergency drugs and equipment: A survey of Australian dentists. Aust Dent J. 1997;42(2):103–8.
13 Chapman PJ. A questionnaire survey of dentists regarding knowledge and perceived competence in resuscitation and occurance of resuscitation emergencies. Aust Dent J. 1995;40(2):98–113.
14 Jamalpour MR, Asadi HK, Zarei K. Basic life support knowledge and skills of Iranian general dental practitioners to perform cardiopulmonary resuscitation. Niger Med J. 2005;56(2):148–152.
15 Gonzaga HF, Buso L, Jorge MA, Gonzaga LH, Chaves MD, Almeida OP. Evaluation of knowledge and experience of dentists of San Paulo state, Brazil about cardiopulmonary resuscitation. Braz Dent J. 2003;14(3):220–222.
16 Berg RA, Hemphill R, Abella BS, Aufderheide TP, Cave DM, Hazinski MF, et al. Part 5: Adult basic life support: 2010 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2010; 122(18 Suppl 3):S685–705.
17 Kavari SH, Chohedri AH. Cardiopulmonary resuscitation: knowledge and personal experience in Iranian dentists. Pak J Med Sci. 2007;23(2):296–7.
18 Singh K, Bhat N, Ramesh N, Sharda A, Asawa K, Agrawal A, et al. Cardiopulmonary resuscitation: Knowledge and personal experience among dentists in Udaipur, India. J Dent Sci. 2011;6(2):72–5.
19 Boddu S, Prathigudupu RS, Somuri AV, Lingamaneni KP, Rao P, Kuchimanchi PK. Evaluation of knowledge and experience among oral and maxillofacial surgeons about cardiopulmonary resuscitation. J Contemp Dent Pract. 2012;13(6):878–81.
20 Narayan DP, Biradar SV, Reddy MT, Sujatha BK. Assessment of knowledge and attitude about basic life support among dental interns and postgraduate students in Bangalore city, India. World J Emerg Med. 2015;6(2):118–22.
21 Jabbour M, Osmond MH, Klassen TP. Life support courses: Are they effective? Ann Emerg Med. 1996;28(6):690–8.
22 El-Shazly M, Makboul G, El-Sayed A. Life expectancy and cause of death in the Kuwaiti population 1987–2000. East Mediterr Health J. 2004;10(1–2):45–55.
Received May 12, 2016
Accepted after revision November 10, 2016
Sarah A. Alkandari, Email: sarahalkandari@live.com
World J Emerg Med 2017;8(1):19–24
10.5847/wjem.j.1920–8642.2017.01.003
 World journal of emergency medicine2017年1期
World journal of emergency medicine2017年1期
- World journal of emergency medicine的其它文章
- Comparison of extracorporeal and conventional cardiopulmonary resuscitation: A meta-analysis of 2 260 patients with cardiac arrest
- The association of layperson characteristics with the quality of simulated cardiopulmonary resuscitation performance
- Simplif ed point-of-care ultrasound protocol to conf rm central venous catheter placement: A prospective study
- Clinical and historical features of emergency department patients with pericardial effusions
- Comparison of neurological clinical manifestation in patients with hemorrhagic and ischemic stroke
- A comparison of perspectives on costs in emergency care among emergency department patients and residents