血清炎性生物标记物在子宫内膜异位症患者血清中的表达及意义
2017-01-04 01:12邓霭辉
河北医药 2016年24期
邓霭辉
·论著·
血清炎性生物标记物在子宫内膜异位症患者血清中的表达及意义
邓霭辉
目的 探讨炎性因子TNF-α、IL-1β、IL-6、IL-8及CA-125、MMP-3、VEGF在子宫内膜异位症患者血清中表达变化及其意义,分析其与患者EMs病变r-AFS临床分期及EMs患者痛经程度的相关性。方法采用酶联免疫法(ELISA)检测入组患者血清中TNF-α、IL-1β、IL-6、IL-8,CA-125、MMP-3、VEGF的浓度。分析EMs患者血清中TNF-α、IL-1β、IL-6、IL-8、CA-125、MMP-3、VEGF的浓度与正常对照人群的差异;分析不同分期EMs患者血清中上述标记物的浓度差异;分析EMs患者术前术后血清中上述标记物的表达变化情况;分析EMs患者血清中上述标记物与痛经评分的相关性。结果炎性相关因子TNF-α、IL-1β、IL-6、IL-8及CA-125、VEGF浓度在EMs患者血清中显著升高(P<0.05),并且随着EMs病变γ-AFS临床分期加重而增加,手术切除病灶后血清中上述指标浓度迅速回落;此外严重痛经EMs患者血清中TNF-α、IL-1β及IL-6的浓度较无痛经EMs患者高(P<0.05)。EMs患者血清中TNF-α、IL-1β及IL-6浓度与患者痛经严重程度呈正相关(P<0.05)。MMP-3在EMs患者血清中浓度显著升高(P<0.05),手术切除病灶后血清中MMP-3迅速下降,然而血清中MMP-3浓度与EMs患者r-AFS临床分期无显著性关联,血清中MMP-3浓度与EMs患者痛经严重程度亦无明显相关性(P<0.05)。结论测定EMs患者血清中TNF-α、IL-1β、IL-6、IL-8及CA-125、MMP-3、VEGF浓度对于EMs的临床诊断具有一定价值,并且可作为无创性辅助检查手段。
子宫内膜异位症;痛经;炎性细胞因子;糖类抗原-125;基质金属蛋白酶-3;血管内皮生长因子
子宫内膜异位症(endometriosis,EMs)的定义为具有活性的子宫内膜腺体或(和)间质在子宫腔以外部位出现,EMs是生育年龄女性的常见病和多发病,其典型临床症状是痛经、慢性盆腔疼痛、性交痛和不孕[1]。疼痛是EMs的特征性临床症状,给女性身心健康造成严重损害,并严重影响患者的生活质量,故EMs引起了越来越多人的重视。目前EMs患者疼痛的治疗方法多种多样,包括药物保守治疗和开腹或腹腔镜下多种手术治疗,但是停药后易复发或其疗效不显著,大多不能完全消除或仅能缓解患者的疼痛症状,故EMs是临床治疗的一个难点,详细探索其发病机制尤其是疼痛机制,对于选择更优的EMs疼痛治疗方法具有十分重要的社会意义。炎性因子在EMs引起疼痛过程中发挥了关键性作用[2],然而目前有关炎性因子与EMs引起疼痛的相关性研究尚未见详细报道。本研究拟在探讨血清中的TNF-α、IL-1β、IL-6、IL-8、CA-125、MMP-3、VEGF等表达水平与EMs的相关性,旨在寻找一种无创、低成本且能早期诊断EMs的血清标记物,探讨上述血清指标与疼痛的相关性,并评价其作为治疗效果评判指标的可行性。
1 资料与方法
1.1 一般资料 选取2013年12月至2014年8月期间因EMs在我院住院并接受腹腔镜手术者61例为试验组,所有患者均送组织病理检测,并且术后经病理检验均诊断为EMs。入选患者,年龄20~43岁,平均年龄(30.2±2.6)岁。EMs诊断标准参考人民卫生出版社第七版《妇产科学》。按照美国生殖协会1985年修订的r-AFS临床分期标准,Ⅰ~Ⅱ期患者25例,Ⅲ~Ⅳ期36例。所有患者术前行EMs痛经评分,评分标准参考等文献[3,4]。对照组选取2013年12月至2013年8月期间我院产科门诊孕前健康检查的育龄期女性36例。2组一般资料具有均衡性。
1.2 标本收集 术前及术后14 d抽取静脉血5 ml,以枸橼酸钠抗凝管储存室温下放置2 h,在我院实验中心高速低温离心机上以2 600 r/min离心5 min,取上清于EP管内并保存于-80°冰箱待测。
1.3 观察指标 本研究采用双抗体夹心ELISA方法检测EMs及正常对照人群血清中TNF-α、IL-1β、IL-6、IL-8、VEGF、CA-125、MMP-3的含量。
2 结果
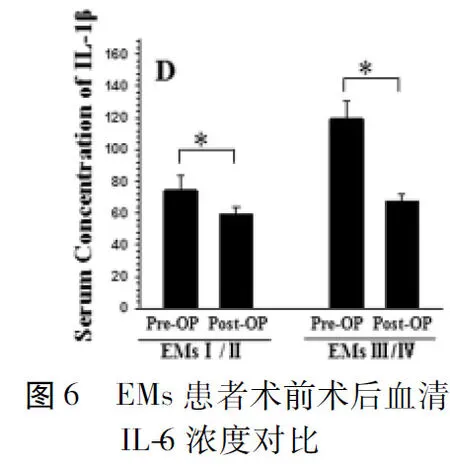
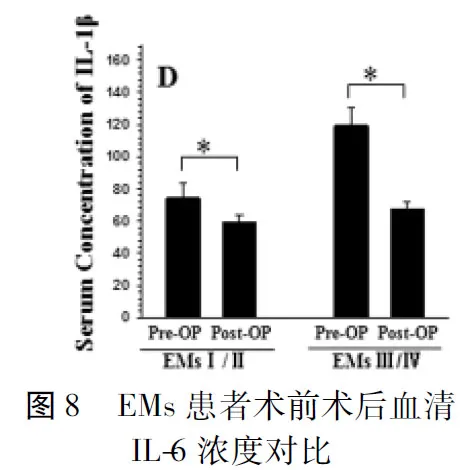
2.1 炎性因子在不同分期EMs患者及正常人群血清中表达水平比较 EMs患者血清中TNF-α浓度显著高于正常组,并且随着病情分期加重其表达水平越高,Ⅲ~Ⅳ期EMs患者血清中TNF-α浓度显著高于Ⅰ~Ⅱ期EMs患者(P<0.05);术后其血清中表达水平显著降低;EMs患者血清中IL-1β浓度显著高于正常组,并且随着病情分期加重其表达水平越高,Ⅲ~Ⅳ期EMs患者血清中IL-1β浓度显著高于Ⅰ~Ⅱ期EMs患者(P<0.05);术后其血清中表达水平显著降低;EMs患者血清中IL-6浓度显著高于正常组,并且随着病情分期加重其表达水平越高,Ⅲ~Ⅳ期EMs患者血清中IL-6浓度显著高于Ⅰ~Ⅱ期EMs患者(P<0.05);术后其血清中表达水平显著降低;EMs患者血清中IL-8浓度显著高于正常组,并且随着病情分期加重其表达水平越高,Ⅲ~Ⅳ期EMs患者血清中IL-8浓度显著高于Ⅰ~Ⅱ期EMs患者(P<0.05);术后其血清中表达水平显著降低。见图1~8。
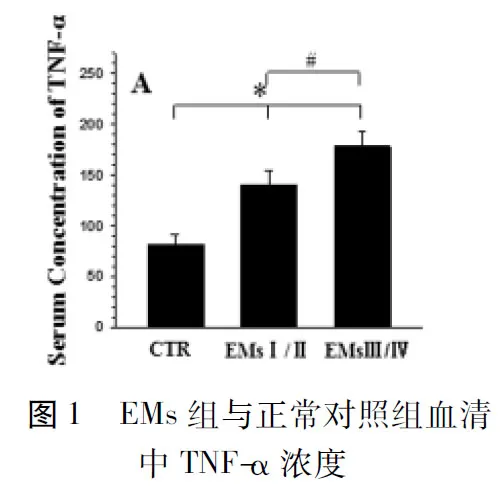

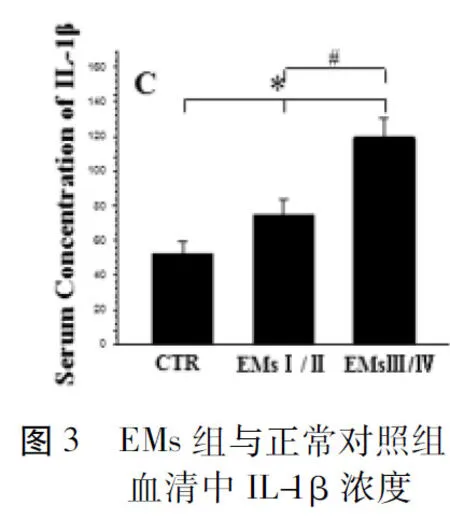

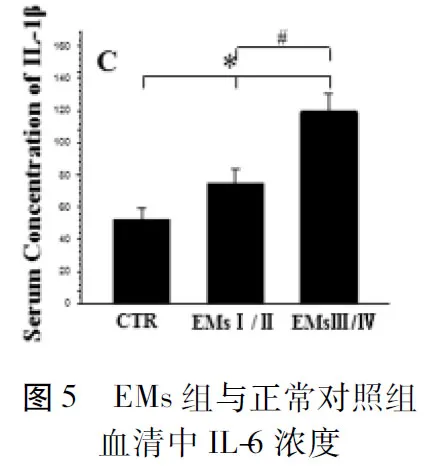
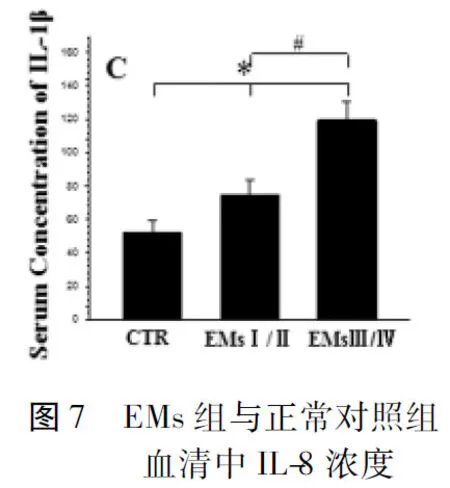
注:与对照组比较,*P<0.05;与Ⅰ~Ⅱ期比较,#P<0.05
2.2 VEGF、CA-125、MMP-3在不同分期EMs患者及正常人群血清中表达水平比较 EMs患者血清中VEGF浓度显著高于正常组,并且随着病情分期加重其表达水平越高,Ⅲ~Ⅳ期EMs患者血清中VEGF浓度显著高于Ⅰ~Ⅱ期EMs患者(P<0.05);术后其血清中表达水平显著降低;EMs患者血清中CA-125浓度显著高于正常组,并且随着病情分期加重其表达水平越高,Ⅲ~Ⅳ期EMs患者血清中CA-125浓度显著高于Ⅰ~Ⅱ期EMs患者(P<0.05);术后其血清中表达水平显著降低;EMs患者血清中MMP-3浓度显著高于正常组,并且随着病情分期加重其表达水平越高,Ⅲ~Ⅳ期EMs患者血清中MMP-3浓度与Ⅰ~Ⅱ期EMs患者无显著性差异(p=0.41);术后其血清中表达水平显著降低。见图9~14。


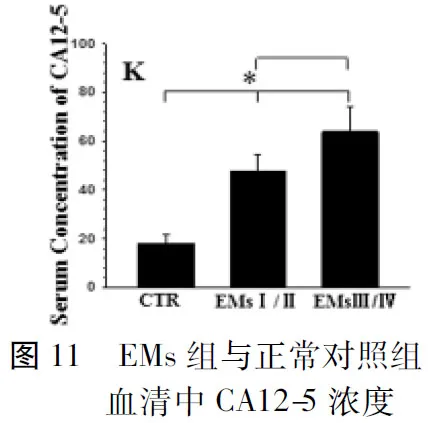
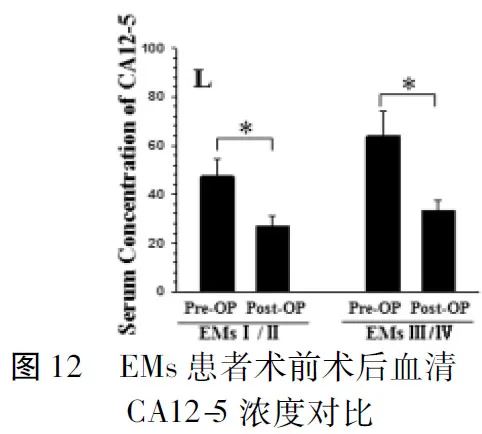

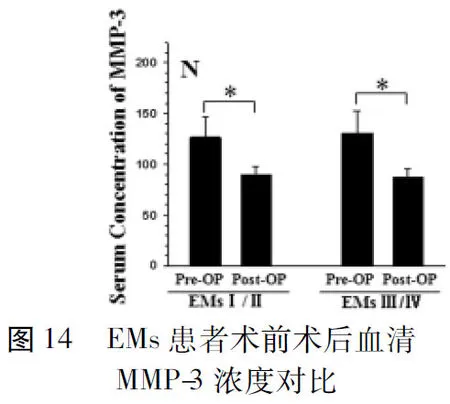
注:与对照组比较,*P<0.05
2.3 EMs患者不同疼痛程度分组血清中TNF-α、IL-1β、IL-6、IL-8、VEGF、CA-125、MMP-3浓度比较 各组EMs患者血清中TNF-α、IL-1β、IL-6、IL-8、VEGF、CA-125、MMP-3浓度与EMs患者痛经评分的关系;结果显示轻度疼痛组血清中TNF-α水平显著高于无痛组(P<0.05);中度疼痛组血清中TNF-α、IL-1β、IL-6水平显著高于轻度疼痛及无痛组(P<0.05);中度疼痛组血清中CA-125水平显著高于轻度疼痛组(P<0.05);重度疼痛组血清中TNF-α、IL-1β、IL-6水平显著高于轻度疼痛及无痛组;重度疼痛组血清中TNF-α水平显著高于中度疼痛组(P<0.05)。见表1、2。月经疼痛评分0分=无痛,1分=轻度疼痛,2分=中度疼痛,3分=重度疼痛。见表1、2。
2.4 EMs患者血清中TNF-α、IL-1β、IL-6、IL-8、VEGF、CA-125、MMP-3表达水平与痛经严重程度的相关性分析 采用Pearson相关性分析EMs患者血清中TNF-α、IL-1β、IL-6、IL-8、VEGF、CA-125、MMP-3浓度与EMs患者痛经评分的关系,结果显示血清中TNF-α浓度与EMs患者痛经程度呈正相关(r=0.94,P<0.01);血清中IL-6浓度与EMs患者痛经程度呈正相关(r=0.56,P<0.01);血清中IL-1β浓度与EMs患者痛经程度呈正相关(r=0.60,P<0.01);血清中IL-8浓度与EMs患者痛经程度无显著性关系(r=0.24,P=0.053);血清中VEGF浓度与EMs患者痛经程度无显著性关系(r=0.20,P=0.109);血清中CA-125浓度与EMs患者痛经程度无显著性关系(r=0.22,P=0.078);血清中MMP-3浓度与EMs患者痛经程度无显著性关系(r=0.01,P=0.928)。见表1、2。

疼痛评分TNF-αIL-1βIL-6IL-8无(n=5)122.2±2.0584.6±3.8539.4±6.3551.0±20.7轻度疼痛(n=14)138.5±8.86*71.7±9.0441.64±5.9250.6±19.9中度疼痛(n=26)165.2±8.43*#110.8±24.32*#60.5±13.1*#67.8±21.7重度疼痛(n=16)191.6±7.15*#△115.6±9.63*#59.31±8.38*#63.4±18.7 F值158.721.115.12.6
注:与无痛比较,*P<0.05;与轻度疼痛比较,#P<0.05;与中度疼痛比较,△P<0.05


疼痛评分VEGF(ng/L)CA-125(U/ml)MMP-3(ng/ml)无(n=5)170.6±22.3550.2±7.19118.8±19.56轻度疼痛(n=14)170.9±15.9349.4±6.23130.9±17.69中度疼痛(n=26)191.8±33.963.7±14.13*132.5±24.21重度疼痛(n=16)183.6±18.155.4±12.11125.1±17.73 F值4.066.530.86
注:与轻度疼痛比较,*P<0.05
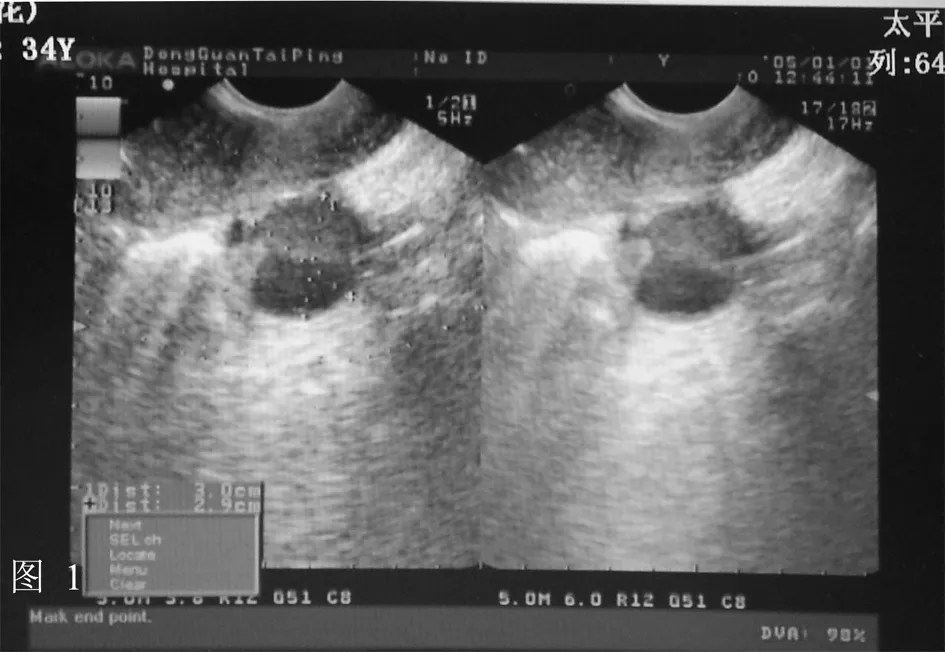
2.5 典型病例展示 患者女,34岁,因“间断下腹胀痛1年余,加重1周”入院,术前B-us显示双侧附件无回声暗区,考虑囊肿,右侧大小约55 mm×47 mm,左侧约24 mm×21 mm。术中发现右侧卵巢囊肿,给予分离并完整切除。术后病理显示镜下所见: 送检物可见囊壁样组织内含黄体细胞,另见含铁血黄素沉着及少量残存的子宫内膜腺体;符合:(双侧卵巢)子宫内膜异位症。见图1~3。


3 讨论
腹腔镜是诊断EMs的金标准,本研究对所有EMs患者均行了腹腔镜手术,术中取病理组织,行病理检查以明确诊断。盆腔疼痛是EMs的主要临床症状之一,同时异位内膜周期性的生长和局部的炎性反应可以引起盆腔各处的粘连。近年来大量研究证实EMs异位病灶内反复出血会导致局部无菌性炎性反应,诸多炎性因子、细胞因子和免疫细胞参与其中;此外病灶内亦会长入神经纤维,炎性反应导致周围和中枢神经疼痛过敏化,EMs的疼痛为炎症伤害性及神经病理性疼痛,此为EMs慢性盆腔痛的主要发生机制之一[5]。
在众多因子中本研究选取了TNF-α、IL-1β、IL-6、IL-8,及CA-125、MMP-3、VEGF,究其原因为炎性因子尤其是TNF-α、IL-1β是目前研究最多的因子,既往研究也显示TNF-α、IL-1β参与了多种慢性疼痛的疾患[6];CA-125及VEGF是目前研究较多与EMs疾病发展相关的因子[7];MMP-3是众多MMPs中在功能最全的基质降解酶,并且能够诱发其他MMPs高表达形成瀑布效应[8]。本研究显示炎症相关因子TNF-α、IL-1β、IL-6、IL-8在EMs患者血清中显著高表达,并且随着EMs并且加重而升高,此外有较为严重痛经的EMs患者血清中TNF-α及IL-6较无痛经患者显著升高。
TNF-α具有调控免疫应答、促进细胞生长分化等多种生物学功能,参与了多种炎症反应和神经相关慢性疼痛[9,10]。Iba等[11]研究发现TNF-α能促进异位内膜和间皮细胞间形成粘连,促进基底部新生血管形成,还可增加胶原蛋白、纤维粘连蛋白等细胞外基质的产生,促进异位子宫内膜组织与周围组织粘连从而是异位内膜成功种植,因而TNF-α在EMs发病过程中发挥了重要作用。研究证明EMs患者血清及腹腔液中TNF-α水平显著升高,并且TNF-α表达程度与EMs疾病严重程度成正比[12]。本研究发现炎症相关因子TNF-α在患者血清中显著高表达,并且随着EMs病情加重而升高,此外有较为严重痛经的EMs患者血清中TNF-α水平较无痛经患者显著升高,与既往研究类似。
IL-1β主要由单核巨噬细胞分泌,是调控免疫炎症反应的重要细胞因子之一,具有广泛的生物学活性[13]。研究发现EMs中异位内膜组织中IL-1β表达明显高于正常内膜组织和在位内膜,而巧克力囊肿中IL-1β浓度亦高于腹腔内其他部位[14]。Liveborn等[15]研究发现IL-1可能通过诱导EMs中异位内膜细胞产生血管内皮生长因子和IL-6从而诱发内膜异位部位出现新生血管。本研究发现炎症相关因子IL-1β在EMs患者血清中显著高表达,并且随着EMs病情加重而升高,手术切除病灶后期血清中IL-1β迅速回落,S但仍较正常人群稍高;并且IL-1β表达水平与EMs患者痛经严重程度呈显著正相关,提示其可能参与了EMs患者疼痛行为学过程。
IL-6是机体内诸多细胞产生的一种具有广泛生物学活性的刺激因子[16]。Tsudo等[17]研究显示血清和腹腔液中IL-6浓度和表达水平随着EMs严重程度加重而升高,并与患者r-AFS评分呈正相关。Schistad等[18]研究发现EMs患者血清中IL-6表达水平显著高于正常人群,并且IV期EMs患者血清中IL-6水平显著高于Ⅰ/Ⅱ期EMs患者。本研究亦发现严重痛经的EMs患者血清中IL-6水平较无痛经患者显著升高,即IL-6的表达水平与EMs患者疼痛呈正相关性,其具体机制有待进一步研究。
IL-8是一种具有很强促进血管生成作用的细胞因子[19],新生血管的生成可以促进异位子宫内膜组织增殖和浸润至腹膜组织内。Carmona等[20]发现EMs异位子宫内膜患者血清中IL-8浓度显著升高,并且与子宫内膜异位组织浸润程度呈正相关。而Kobayashi等[21-24]认为IL-8促进异位内膜基底部新生血管形成是逆流入腹腔的子宫内膜碎片种植成功并且生长增殖的关键。本研究发现炎性相关因子IL-8在患者血清中显著高表达,并且随着EMs病情加重、疾病分期增加而升高,然而血清中IL-8的浓度似乎与EMs患者痛经严重程度无相关性。总体来说IL-8能促进异位内膜局部血管生成、增强异位内膜细胞的粘附、浸润能力,从而在EMs发病过程中发挥了重要作用。
除炎性因子外,Garcia-Manero等[25]研究发现血管上皮生长因子VEGF-A在子宫内膜异位症患者的血清及腹腔液中显著升高,并且其浓度与EMs的严重程度相关,提示EMs中发挥了重要作用,然而其与EMs患者痛经程度无明显相关性。然而Kianpour等[26]研究显示EMs患者血清中VEGF浓度并未明显升高,EMs患者腹腔液中VEGF浓度显著高于正常人群,并且腹腔液中VEGF浓度显著高于血清。在本研究中,我们发现EMs患者血清中VEGF较正常人群显著升高,并且与EMs分期严重程度相关,手术切除异位子宫内膜后血清中VEGF迅速下降,提示VEGF参与了EMs的进程,是良好的血清标记物;然而血清中VEGF浓度与EMs患者痛经严重程度无明显相关性。
1986年barbreri等首次证实EMs患者血清中CA-125水平显著高于正常人群,并且血清中CA-125水平随着EMs病情加重、疾病分期升高而增加[27,28]。随后一系列研究发现CA-125与EMs存在密切关系,测定CA-125的值可以应用于EMs临床早期无创诊断、检测疗效[29],并且CA-125可以反映EMs病情严重程度,Ⅲ/Ⅳ期EMs患者血清和腹腔液中CA-125显著高于Ⅰ/Ⅱ期EMs患者,也高于正常人群[30]。本研究发现CA-125在EMs患者血清中显著高表达,并且随着EMs病情加重、疾病分期增加而升高,而手术切除病灶后血清中CA-125迅速回落,但仍较正常人群稍高,提示CA-125诊断EMs具有高敏感性和高特异性,是一种良好EMs生物检测标记物。
此外本研究尚探讨了基质金属蛋白酶在EMs疾病进程中的作用,研究结果显示MMP-3在EMs患者血清中显著高表达,然而与EMs病情轻重、疾病γ-AFS分期无显著性关系,此结果与既往研究类似。Krikun等[31]研究显示EMs患者外周血中MMP-3 mRNA表达水平显著升高,提示其可以作为EMs临床检验的分子标记物。研究发现EMs在位和异位子宫内膜中MMP-3表达均高于正常人群的子宫内膜组织,而TIMP-1、2、3表达则低于正常人群,提示MMP-3在EMs发生发展过程中发挥重要作用。
综上所述,炎性因子TNF-α、IL-1β、IL-6、IL-8、血管生成因子VEGF、基质降解相关酶MMP-3及CA-125在EMs的发生发展过程中发挥了重要作用,其血清学检测有助于EMs的无创性诊断,动态检测上述因子的血清学变化有助于掌握病情变化,检测疗效。此外炎症相关因子TNF-α、IL-1β及IL-6参与了EMs相关盆腹腔疼痛,详细探讨其具体机制有助于为将来研发EMs相关慢性疼痛的生物学疗法提高数据支持。
1 Kodaman PH.Current Strategies for Endometriosis Management.Obstet Gynecol Clin North Am,2015,42:87-101.
2 Borrelli GM,Abrao MS,Mechsner S.Can chemokines be used as biomarkers for endometriosis? A systematic review.Hum Reprod,2014,29:253-266.
3 Yeung P.The Laparoscopic Management of Endometriosis in Patients with Pelvic Pain.Obstet Gynecol Clin North Am,2014,41:371-383.
4 Bourdel N,Alves J,Pickering G,et al.Systematic review of endometriosis pain assessment:how to choose a scale? Hum Reprod Update,2015,21:136-152.
5 Zhang G,Dmitrieva N,Liu Y,et al.Endometriosis as a neurovascular condition:estrous variations in innervation,vascularization,and growth factor content of ectopic endometrial cysts in the rat.Am J Physiol Regul Integr Comp Physiol,2008,294:R162-171.
6 Olmos G,Llado J.Tumor necrosis factor alpha:a link between neuroinflammation and excitotoxicity.Mediators of inflammation,2014,2014:861231.
7 Patacchiola F,D'Alfonso A,Di Fonso A,et al.New horizons in the non-invasive diagnosis of endometriosis.Clin Exp Obstet Gynecol,2013,40:524-530.
8 Momohara S,Yamanaka H.Immunological and serological tests for diagnosis of rheumatoid arthritis:MMP-3.Nihon rinsho Japanese journal of clinical medicine,2005,63:313-317.
9 Sasaki M,Hashimoto S,Sawa T,et al.Tumor necrosis factor-alpha induces expression of C/EBP-beta in primary afferent neurons following nerve injury.Neuroscience,2014,279:1-9.
10 Zhang XC,Kainz V,Burstein R,et al.Tumor necrosis factor-alpha induces sensitization of meningeal nociceptors mediated via local COX and p38 MAP kinase actions.Pain,2011,152:140-149.
11 Iba Y,Harada T,Horie S,et al.Lipopolysaccharide-promoted proliferation of endometriotic stromal cells via induction of tumor necrosis factor alpha and interleukin-8 expression.Fertil Steril,2004,82:1036-1042.
12 Li J,Chen Y,Wei S,et al.Tumor necrosis factor and interleukin-6 gene polymorphisms and endometriosis risk in Asians:a systematic review and meta-analysis.Annals of human genetics,2014,78:104-116.
13 Garlanda C,Dinarello CA,Mantovani A.The interleukin-1 family:back to the future.Immunity,2013,39:1003-1018.
14 Lambert S,Santulli P,Chouzenoux S,et al.Endometriosis:increasing concentrations of serum interleukin-1beta and interleukin-1sRII is associated with the deep form of this pathology.Journal de gynecologie,obstetrique et biologie de la reproduction,2014,43:735-743.
15 Lebovic DI,Bentzien F,Chao VA,et al.Induction of an angiogenic phenotype in endometriotic stromal cell cultures by interleukin-1beta.Mol Hum Reprod,2000,6:269-275.
16 Erta M,Quintana A,Hidalgo J.Interleukin-6,a major cytokine in the central nervous system.Int J Biol Sci,2012,8:1254-1266.
17 Tsudo T,Harada T,Iwabe T,et al.Altered gene expression and secretion of interleukin-6 in stromal cells derived from endometriotic tissues.Fertil Steril,2000,73:205-211.
18 Schistad EI,Espeland A,Pedersen LM,et al.Association between baseline IL-6 and 1-year recovery in lumbar radicular pain.Eur J Pain,2014.
19 Singh JK,Simoes BM,Howell SJ,et al.Recent advances reveal IL-8 signaling as a potential key to targeting breast cancer stem cells.Breast cancer research:BCR,2013,15:210.
20 Carmona F,Chapron C,Martinez-Zamora MA,et al.Ovarian endometrioma but not deep infiltrating endometriosis is associated with increased serum levels of interleukin-8 and interleukin-6.Journal of reproductive immunology,2012,95:80-86.
21 Kobayashi H,Higashiura Y,Shigetomi H,et al.Pathogenesis of endometriosis:the role of initial infection and subsequent sterile inflammation (Review).Molecular medicine reports,2014,9:9-15.
22 van der Linden PJ.Theories on the pathogenesis of endometriosis.Hum Reprod,1996,11:53-65.
23 Nisolle M,Casanas-Roux F,Donnez J.Early-stage endometriosis:adhesion and growth of human menstrual endometrium in nude mice.Fertil Steril,2000,74:306-312.
24 Nishida M,Nasu K,Narahara H.Role of chemokines in the pathogenesis of endometriosis.Frontiers in bioscience (Scholar edition),2011,3:1196-1204.
25 Garcia-Manero M,Alcazar JL,Toledo G.Vascular endothelial growth factor (VEGF) and ovarian endometriosis:correlation between VEGF serum levels,VEGF cellular expression,and pelvic pain.Fertil Steril,2007,88:513-515.
26 Kianpour M,Nematbakhsh M,Ahmadi SM,et al.Serum and peritoneal fluid levels of vascular endothelial growth factor in women with endometriosis.International journal of fertility & sterility,2013,7:96-99.
27 Barbieri RL,Niloff JM,Bast RC,et al.Elevated serum concentrations of CA-125 in patients with advanced endometriosis.Fertil Steril,1986,45:630-634.
28 Kafali H,Artuc H,Demir N.Use of CA125 fluctuation during the menstrual cycle as a tool in the clinical diagnosis of endometriosis; a preliminary report.Eur J Obstet Gynecol Reprod Biol,2004,116:85-88.
29 王志萍,蔡星香.血清CA125检测在妇科疾病临床应用中的评价.海峡医学,1995,17:61-63.
30 戚瑞珍,李亚里.CA125在子宫内膜异位症中的临床意义.中国妇幼保健,2007,22:3644-3645.
31 Krikun G.Endometriosis,angiogenesis and tissue factor.Scientifica,2012,2012:306830.
Expression and significance of inflammatory biological markers in serum of patients with endometriosis
DENGAihui.
TaipingPeople’sHospitalofDongguanCity,Guangdong,Dongguan523905,China
Objective To investigate the the changes and significance of serum levels of inflammatory cytokines including TNF-α,IL-1β,IL-6,IL-8,CA-125,MMP-3,and VEGF in serum of patients with endometriosis (EMs),and to analyze the correlation between the changes and pathological changes of EMs, γ-AFS clinical staging and dysmenorrhea degree of patients.Methods A total of 61 patients with endometriosis (observation group) and 36 healthy women (control group) were enrolled in the study.The serum levels of TNF-α,IL-1β,IL-6,IL-8,CA-125,MMP-3,and VEGF in both groups were detected by immunosorbent assay (ELISA),and the differences between the two groups were analyzed.Moreover the differences of the serum levels of these factors in patients with EMs at different stages were observed before operation and after operation.The correlation between these factors and dysmenorrhea scores of patients were analyzed.Results The serum levels of TNF-α,IL-1β,IL-6,IL-8,CA-125 and VEGF in observation group were significantly higher than those in control group (P<0.05),moreover,which were increased with the aggravation of pathological changes of Ems and γ-AFS clinical staging,however, which were decreased rapidly after resection of ectopic endometrium.Moreover the serum levels of TNF-α,IL-1βand IL-6 of patients with severe dysmenorrhea were significantly higher than those of patients without dysmenorrhea (P<0.05). The serm levels of TNF-a,IL-1βand IL-6 in patients with EMs were positively correlated to the severity of dysmenorrhea of patients.The serum levels of MMP-3 in serum of patients with EMs were significantly increased (P<0.05). After resection of ectopic endometrium the serum levels of MMP-3 were decreased quickly,however, the serum levels of MMP-3 were not closely correlated to r-AFS clinical staging of patients with EMs,moreover, which were not closely related with the severity of dysmenorrhea of patients.Conclusion The detection of serum levels of TNF-α,IL-1β,IL-6,IL-8,CA-125,MMP-3 and VEGF has a certain value in the diagnosis of endometriosis,moreover, which can be regarded as noninvasive auxiliary examination method.
endometriosis;dysmenorrhea;inflammatory cytokines;carbohydrate antigen-125;matrix metalloproteinase-3;vascular endothelial growth factor
10.3969/j.issn.1002-7386.2016.24.001
523905 广东省东莞市太平人民医院
R 711.71
A
1002-7386(2016)24-3685-06
2016-06-18)
猜你喜欢
今日畜牧兽医(2022年10期)2022-12-23
中华养生保健(2020年9期)2021-01-18
中国生殖健康(2019年3期)2019-02-01
临床医药文献杂志(电子版)(2017年11期)2017-05-17
中外医疗(2016年15期)2016-12-01
国外医药(抗生素分册)(2016年1期)2016-07-10
中华老年多器官疾病杂志(2016年9期)2016-04-28
中国继续医学教育(2015年4期)2016-01-07
中国当代医药(2015年31期)2015-03-01
郑州大学学报(医学版)(2015年1期)2015-02-27