
Maternal and obstetric risk factors associated with preterm delivery at a referral hospital in northern-eastern Tanzania
2017-01-03 11:23TheresiaTemuGileadMasengaJosephObureDominicMoshaMichaelMahande
Theresia B Temu, Gilead Masenga, Joseph Obure, Dominic Mosha, Michael J Mahande*
1Department of Epidemiology and Biostatistics, Institute of Public Health, Kilimanjaro Christian Medical University College, Moshi, Tanzania
2Department of Obstetrics and Gynaecology, Kilimanjaro Christian Medical Centre, Moshi, Tanzania
Maternal and obstetric risk factors associated with preterm delivery at a referral hospital in northern-eastern Tanzania
Theresia B Temu1, Gilead Masenga2, Joseph Obure2, Dominic Mosha1, Michael J Mahande1*
1Department of Epidemiology and Biostatistics, Institute of Public Health, Kilimanjaro Christian Medical University College, Moshi, Tanzania
2Department of Obstetrics and Gynaecology, Kilimanjaro Christian Medical Centre, Moshi, Tanzania
ARTICLE INFO
Article history:
Received 2016
Received in revised form 2016
Accepted 2016
Available online 2016
Risk factors
Objective:Preterm delivery is the second most leading cause of under-five deaths in the world and has been associated with poor neonatal outcomes especially in developing countries where management of severe and extreme preterm new-born is a challenge. This study aimed to determine maternal and obstetric factors associated with preterm delivery among women who delivered at Kilimanjaro Christian Medical Centre.Methods:This was unmatched case-control study conducted at the Kilimanjaro Christian Medical Centre between April and May, 2014. A total of 1 143 women were recorded to have delivered during the study period. Of these, 162 had preterm delivery which comprised the case group while controls were selected from women who had term birth (n = 209) making a final sample size of 371 women. All participants were interviewed using a standard questionnaire to determine factors associated with preterm delivery. Additional data were extracted from maternal clinic cards and hospital records. Data analysis was performed using statistical package for social science version 20.0. Odds ratios with 95% CI for factors associated with preterm delivery were estimated in a multivariate logistic regression models. A P value of less than 0.05 was considered statistically significant.Results:The prevalence of preterm birth was 14.2%. Numerous factors were associated with preterm delivery including living alone (AOR 5.26, 95% CI: 1.1011–25.14), no formal education (AOR 1.2, 95% CI: 3.55–4.06), heavy physical works during pregnancy (AOR 3.13, 95% CI: 1.44–6. 81), being a peasant (AOR 2.24, 95% CI: 1.16–4.33), business women (OR 2.88, 95% CI: 1.44–5.74), and history of still birth (OR 4.93; 95% CI: 1.59–15.35). Furthermore, history of miscarriage (OR 1.84, 95% CI: 1.02–3.31), preeclampsia (OR 6.83, 95% CI: 2.92–15.96), placenta previa (OR 7.54, 95% CI: 1.65–34.51), abruption placenta (OR 4.04, 95% CI: 1.08–15.17), Caesarean section delivery (OR 1.60, 95% CI: 1.06–2.43), inadequate ANC visits < 4 (OR 3.25, 95% CI: 2.04–5.19), multiple pregnancy (OR 2.75, 95% CI: 1.15–6.61), low birth weight (OR 34.27, 95% CI: 15.93–73.7) and UTIs during pregnancy (OR 1.678, 95% CI: 1.064–2.649) were also independently associated with preterm delivery.Conclusion:The risk factors for preterm delivery identified in this study are consistent with previous studies. Clinicians and other health care providers should routinely assess women at high risk of preterm delivery during prenatal care to prevent the occurrence of preterm delivery and associated adverse perinatal outcomes.
1. Introduction
Preterm delivery refers to childbirth occurring at less than 37 completed weeks of gestational age. It contributes to about 11% of annual birth worldwide[1]. It is the leading cause of neonatal morbidity and mortality; and the second most leading cause of under-five death in the world[2, 3]. A previous hospital based study in North-Eastern Tanzania reported prevalence of preterm birth of 14.3% which was higher compared with that reported in developing countries [4].
Previous studies have reported risk factors for preterm delivery including extreme maternal age (<20 or ≥35 years), living without partner, living in rural area, stress, heavy physical work, low education level, underweight, overweight and obesity[2,5].In addition, poor attendance to ANC, antepartum haemorrhage, diabetes, preeclampsia, foetal growth retardation, preterm premature rupture of membranes, multiple pregnancy, and maternal infections have also been associated with an increased risk of preterm delivery [4-7].
There is limited information on risk factors and causes of preterm delivery in Tanzania. This study aimed to determine maternal and obstetric factors associated with preterm delivery among women who delivered in the department of obstetrics and Gynecology at Kilimanjaro Christian Medical Centre (KCMC). The study findings are critical in identifying women at risk of preterm delivery, developing prevention and management plans to help reduce the adverse outcomes associated with preterm deliveries. The interventions may help to improve new-born’ survival rates in our setting.
2. Materials and methods
2.1. Study design and setting
This was unmatched case-control study which was conducted from April to May 2014. The study was carried out in the department Obstetrics and Gynecology at KCMC which is one of the referral hospitals located in the north-eastern Tanzania. The hospital serves over 5 million people (Tanzania National census 2012)[8]. Majority of patients comes from Kilimanjaro region which is the main catchment area of KCMC and other neighbouring regions. The hospital has approximately annual delivery rate of 4 000 deliveries.
2.2. Study population
The study sample included all women with a known gestation age who delivered at KCMC in the Obstetrics and Gynecology department. The gestational age was estimated based on the date of the beginning of last normal menstrual date and abdominal ultra sound in first trimester. A total of 1 143 women were recorded to have delivered during the study period. Of these, 162 had preterm delivery and met study criteria for being the case group while controls were selected from women who had term birth with gestational age of 38, 39, and 40 weeks (n= 209).
2.3. Study variables
The main outcome was preterm delivery. Preterm was defined as delivery of a live neonate before 37 gestational weeks. The independent variables included area of residence, maternal age, marital status, education level, occupation, heavy physical activities during pregnancy, and alcohol use in pregnancy and parity. Obstetric characteristics included attendance to antenatal care during the present pregnancy, history of still birth, history of miscarriage, history of abortion, ectopic pregnancy, and previous history of preterm delivery, mode of delivery, sex of the baby, birth weight, chronic hypertension, pregnancy induced hypertension, placenta previa, abruption placenta, uterine rupture, and fibroid. Medical characteristics included presence of tuberculosis, diabetes mellitus and urinary tract infections during pregnancy.
2.4. Data collection
Women were recruited from obstetrics ward for the study between day 0 and 5 post deliveries, depending on whether she had complications or not. Informed consent was obtained prior interview. Women were asked to participate in a 25 min interview in which a pretested standardized questionnaire was used to obtain information from the study participants. Other information was extracted from delivery book, antenatal cards and hospital files for verification and to obtain additional information of the study participant.
2.5. Ethical consideration
This study was approved by the Kilimanjaro Christian Medical University College Research and Ethics committee. Permission to carry out the study was obtained from KCMC administrative authority. Informed consent was obtained from all the participants, prior to the interview.
2.6. Statistical analysis
Data analysis was performed using Statistical Package for Social Sciences version 20.0. Continuous variables were summarized using descriptive statistics such as mean with standard deviation (SD). Studentt-test was used to compare means between groups. Categorical variables were summarized using frequency and proportions. Chi square test was used to determine the statistical association between set of explanatory variables and preterm delivery during univariate analysis. Odds ratio (OR) with 95% confidence interval (CI) for factors associated with preterm delivery was estimated in a multiple logistic regression models while controlling for the confounders. APvalue of less than 0.05 was considered statistically significant.
3. Results
3.1. Social demographic characteristics of study participants
Socio-demographic characteristics of the study participants are summarized in Table 1. A total of 371 women were studied. The mean age for cases and controls were [(28.4±6.3) vs (28.8±6.9)] years respectively. Furthermore, cases had lower mean gestational age as compared to controls counter parts [(33.8 ± 2.8) vs. (39.0 ± 1.5)] weeks, respectively)]. Majority (88.1%) of participants were married or cohabiting; and nearly 2/3 (65.8%) reported never used alcohol in their life.
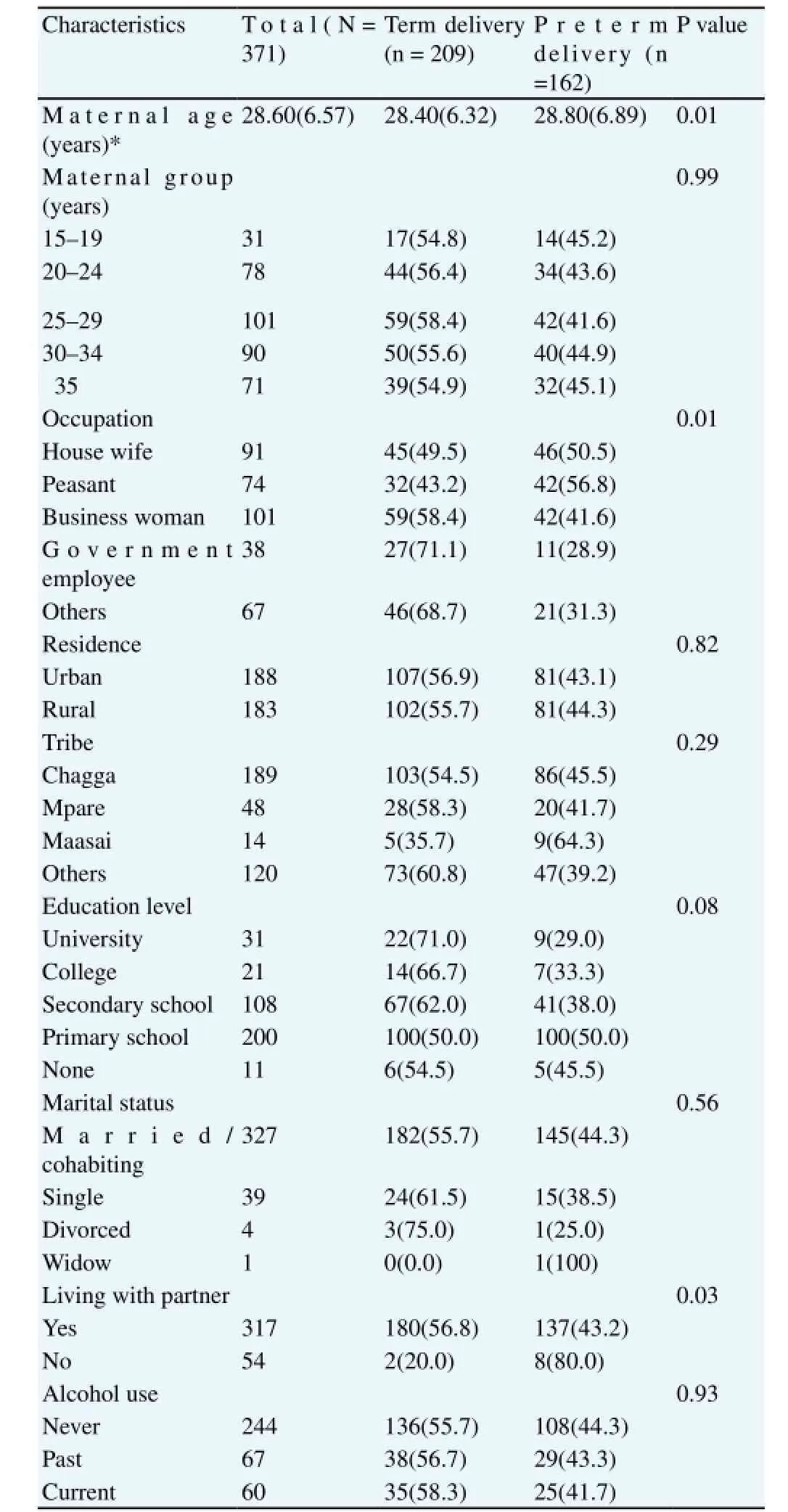
Table 1Characteristics of study participants in preterm delivery group and term delivery group (N=371).
3.2. Sociodemographic factors associated with preterm delivery
Some social and demographic characteristics were associated with increased risk of preterm delivery (Table 2). These include living without partner (OR 5.26, 95% CI: 1.1–25.14), no education (OR 1.2, 95% CI: 3.55–4.06), having hard physical works during pregnancy (OR 3.13, 95% CI: 1.44–6.81). Regarding of occupations, women who were involved in farming/peasant (OR 2.24, 95% CI: 1.16–4.33) and business (OR 2.88, 95% CI: 1.44–5.74) have increased odds of having preterm delivery. Marital status, tribe, area of residence and alcohol use during the index pregnancy were not significantly associated with preterm delivery.
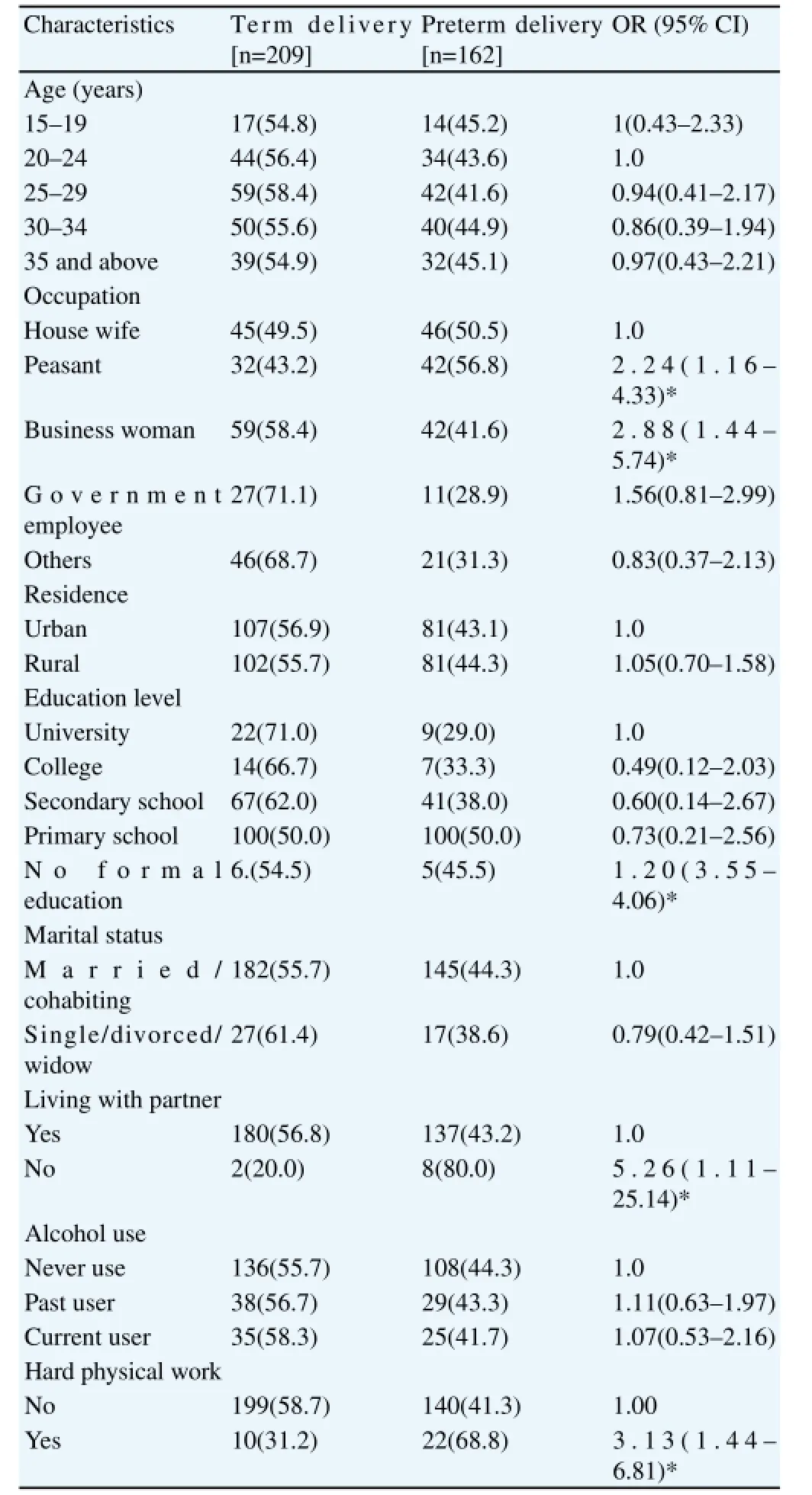
Table 2Maternal sociodemographic characteristics associated with preterm birth (N=371).
3.3. Obstetric and medical factors associated with preterm delivery
The obstetric factors associated with increased risk of preterm delivery have been presented in Table 3. Numerous factors were associated with increased odds of preterm delivery. These include previous history of still birth (OR 4.93; 95% CI: 1.59–15.35), history of miscarriage (OR 1.84; 95% CI: 1.02–3.31), pregnancy induced hypertension (OR 6.83; 95% CI: 2.921–15.96), placenta previa (OR 7.54; 95% CI: 1.65–34.51), abruption placentae (OR 4.04; 95% CI: 1.08–15.17), delivery by caesarean section (OR
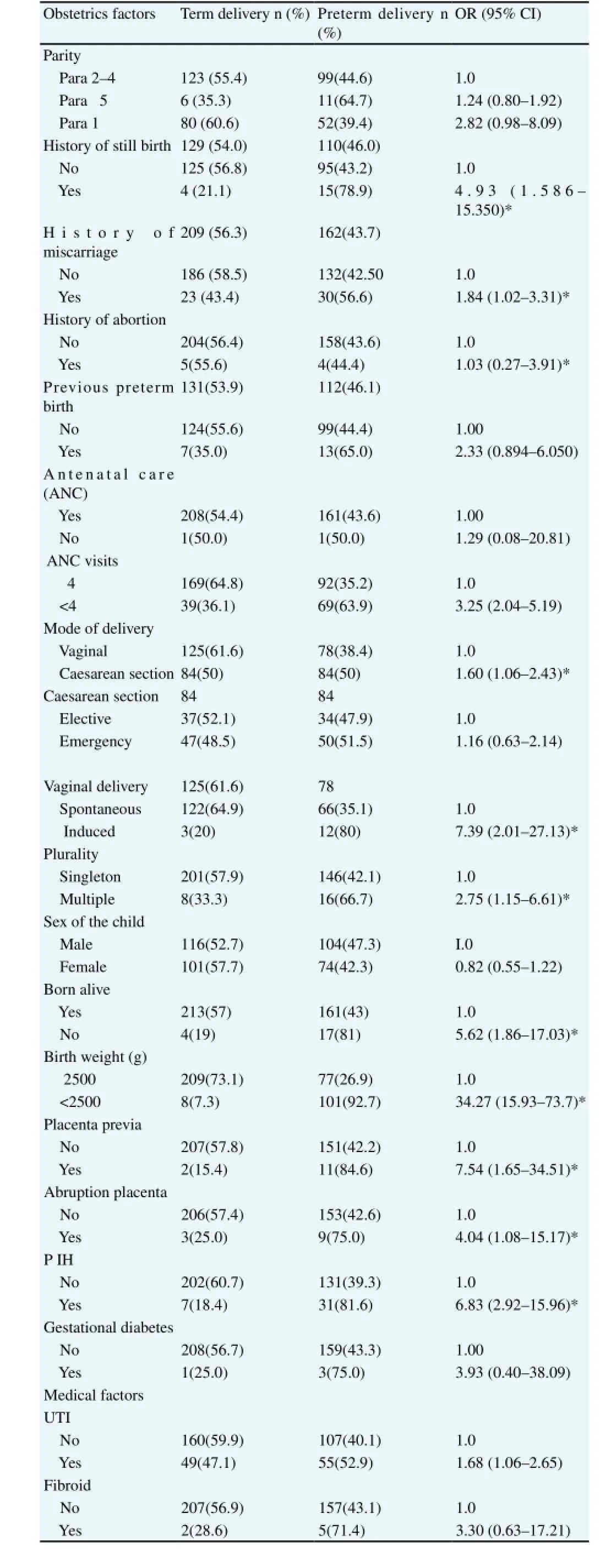
Table 3Obstetrics and medical factors associated with preterm delivery (N=371).
1.60; 95% CI: 1.06–2.43), less than four antenatal care visits (OR 3.25; 95% CI: 2.04–5.19), multiple pregnancy (OR 2.75; 95% CI: 1.15–6.61), still birth (OR 5.62; 95% CI: 1. 86–17. 03), induced vaginal delivery (OR 7.39; 95% CI: 2.02–27.13), low birth weight (OR 34.27; 95% CI: 15.93–73.7) and urinary tract infection (OR 1.68; 95% CI: 1.06–2.65). Other known risk factors such as history of pregnancy termination, previous history of preterm delivery, emergency caesarean section, and primigravida and parity ≥5 were not significantly associated with increased risk of preterm delivery in this study.
When obstetrics factor were adjusted for some possible confounders; pregnancy induced hypertension/preeclampsia, placenta previa, placenta abruption, caesarean section, multiple pregnancy, stillbirth in the index pregnancy, induced vaginal delivery and urinary tract infection were significantly associated with increased odds of preterm delivery (Table 4).
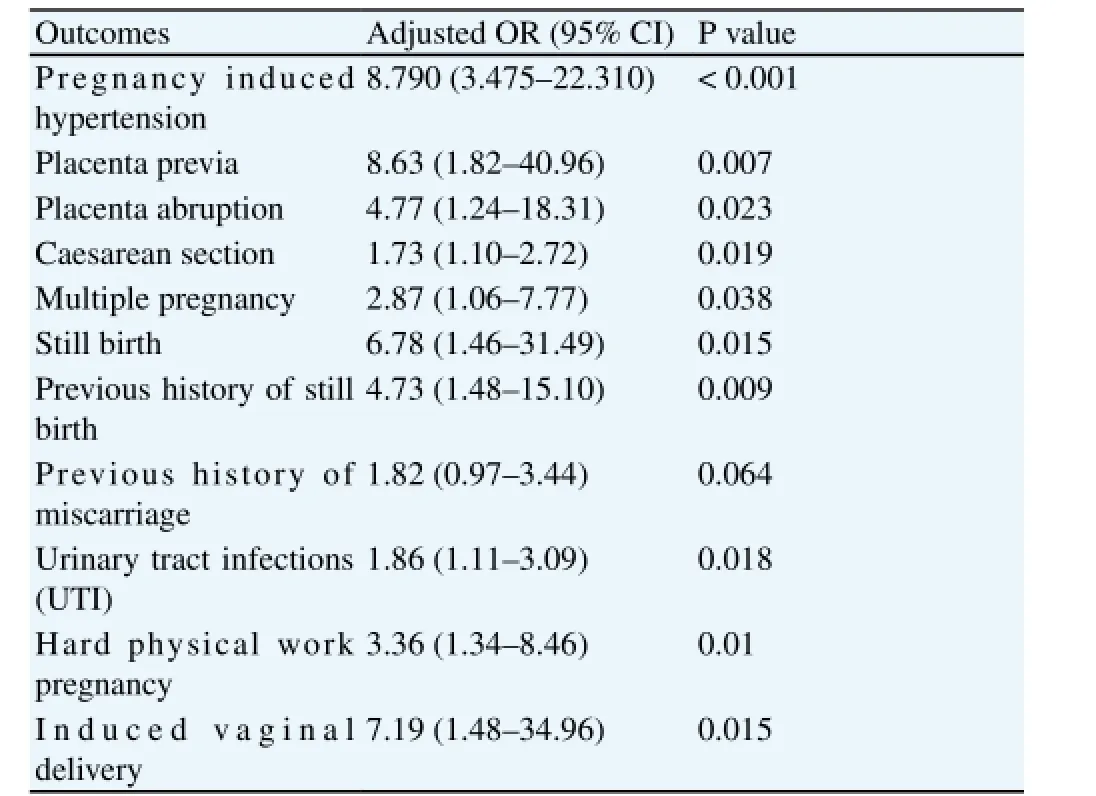
Table 4Obstetrics and medical factors associated with preterm delivery (N=371).
4. Discussion
In this study we found a high prevalence of preterm delivery of 14.2%. This is consistent with previous study which was conducted on similar setting using hospital birth registry data[4]. The estimated prevalence of preterm delivery in our study is higher than the previous report in Tanzania as well as global estimates of 12% and 11%, respectively [9,10]. The higher prevalence of preterm delivery in our study may be explained by the referral nature of the study setting where women with high risk of medical and obstetrics complications are referred to deliver for advance management and care. This is important caveat to the referral and tertiary hospitals in developing countries that calls for well-equipped neonatal units that are capable to support preterm newborns.
Maternal age was not associated with increased risk of preterm delivery according to present study. In contrast to other studies, maternal age below 19 years and advanced maternal age were associated with increasing risk of preterm delivery[11-13]. Lack of association between extreme maternal age and preterm delivery inour study may be explained by high level of management of these group to prevent the risk of preterm birth as clinicians consider that these women is a high risk group. The small number of cases in this group may also be the possible reason to explained insignificant findings.
Women residing in urban area during pregnancy have been shown to have a less likelihood of having preterm delivery[3]. Similarly, in the present study women who were living in rural areas during pregnancy were 5% more likely to have preterm delivery compared to those living in urban area. This is probably due to the reason that there is an easy accessibility to health facilities in urban area than in rural area which can play an important part in the prevention of preterm delivery. Also women who are living in rural are more likely to be subjected to hard physical works like farming which increases the risk of preterm delivery particularly to women with other risk factors for preterm delivery.
Illiteracy which is more in rural area as opposed to urban area is an important risk factor for preterm delivery[4,14]. In the present study mothers who did not attend school had 20% odd of preterm delivery compared to mothers who reached primary education level or higher, which is due to limited access to services, information and knowledge on different health prevention skills. In our study women who were involved in hard physical work during pregnancy had more than three folds increased odds of preterm delivery even after adjusting for the confounders. This is consistent with previous studies[2,15,16]. The high risk of preterm delivery in this group may be explained by increased stress which triggers premature labor which leads to preterm delivery.
Business women, peasants and government employees had at least two folds increased odds of preterm delivery as compared to house wife. This is consistent to previous studies reported the association between maternal occupation and increased risk of preterm delivery. The study done in Korea by Park,et al.[14] revealed that laborer women had 20% increased risk of preterm delivery as compared to legislators and managers. Peasants and business women are associated with increased risk of preterm delivery probably due to working hard in the farms and for their business which trigger early labor and hence lead to preterm birth.
Alcohol use was not significantly associated with preterm delivery in our study. This was in contrast with previous studies which reported an association between alcohol use during pregnancy and increasing risk of preterm delivery[17,18]. We also found that living without partner increased women’ likelihood of preterm delivery by five folds compared with living with partner. Similar finding was reported by previous investigators[13]. This is probably due to lack of someone, to whom they could explain their problems, advice, moral support and provide family care with regard to their health which may increase stress and thereby increase the likelihood of having preterm delivery.
Women with previous history of preterm delivery, stillbirth and miscarriage had increased risk of preterm delivery more than two folds. This corresponds with previous studies in Tanzania and China [2,4]. The observed increased odds of preterm delivery associated with previous history of preterm delivery, stillbirth and miscarriage in our study is lower than that reported with previous studies and the most recent study[2,7]. This may be due to differences in recall bias between studies. In the other hand the high risk of preterm delivery in women with previous preterm delivery may be explained by the persistence of the causes of previous preterm delivery in subsequent pregnancy hence leading to recurrence of preterm delivery.
In this study, we found no significant association between history of pregnancy termination and preterm delivery in subsequent pregnancy. This is in contrast with the previous investigations[19] that reported 11% increased risk of preterm delivery in women with history of pregnancy termination as compared to those who had no history of pregnancy termination. However, some investigators have found that women who had pregnancy termination with misoprostol were less likely to have preterm delivery[20]. It is worth noting that pregnancy termination due to non-medical reasons is illegal in Tanzania and associated with significant stigma, therefore some women may not disclose such information which may lead to underreporting of previous pregnancy termination as well as spontaneous abortion.
Pregnancy induced hypertension was strongly associated with preterm delivery in this study even after adjusting for the confounders. Women who had pregnancy induced hypertension/ preeclampsia were nearly seven folds more likely to have preterm delivery as compared to normotensive women. This is consistent to other studies [2,7]. Hypertension decreases the uteroplacental blood floor which lead to intrauterine growth restriction that cause preterm delivery.
We found that women who had placenta previa were seven times more likely to have preterm delivery as compared to those who had no placenta previa. This is compatible with previous studies who reported high risk of preterm delivery among women with placenta previa as compared to those without[6,21]. This could be explained by the abnormal position of placenta where by uterine contraction can lead to heavy bleeding of which require immediate delivery or pregnancy termination.
Abruption placenta has been associated with increased risk of preterm delivery by previous investigators[2]. This agrees with our finding. We found mothers who had abruption placenta were 4 times more likely to have preterm delivery as compared to mothers who had no abruption placenta. This may be explained by separation of a normally implanted placenta from the uterine wall before term which can cause vaginal bleeding, haemorrhagic shock, and foetal death which lead to emergency hospital indicated delivery even before term.
We found that mothers with multiple pregnancies had had more than two folds increasing likelihood of having preterm delivery as compared to mothers with singleton even after adjusting for the confounders. Similar finding was reported among Nigerian and Finnish population[16,22]. In the present study, women with multiple gestations had 29.6% increased odds of preterm delivery compared with singleton. This is probably due to over distension of the uterus by multiple pregnancies which stimulate early labour leading to preterm delivery[23].
In our study delivery by caesarean section was strongly associated with preterm delivery even after adjusting for confounders, which was similar to previous research findings[24]. This may be due to the reason that mothers who deliver by caesarean section have other pregnancy complications such as foetal distress which is an indication for emergency caesarean section. Induced vaginal delivery was associated with increased risk of preterm delivery. This can be explained by the reason that induced vaginal delivery may also be done to pregnant women who have pregnancy complications even before term so as to rescue their life and of foetus.
Maternal poor ANC attendance was associated with increased risk of preterm delivery in this study. We found that women who attended ANC less than four times were three times more likely to have preterm delivery as compared to women who attended ANC four times. This is consistent with previous studies [2,4]. This could be explained by the fact that women who have regular attendance to ANC are more likely to be detected with severely diseases orobstetrics complications and hence may facilitate appropriate case management which can prevent preterm delivery.
Our findings indicate that female sex was associated with lower risk of preterm delivery. Female babies were less likely to be born premature compared to male babies. This is similar to previous investigators[14] who found that female sex was a preventive factor for preterm delivery. Our study findings are also reflected in a study conducted among Libyan women and revealed that male sex infant were two times more likely to be born preterm as compared to female counterparts[25].
Stillbirth has been found to be associated with preterm delivery in our study. This is consistent with previous studies[16,26]. The shared most common etiological pathways between stillbirth and preterm birth may explain the observed association[27].
Our study shows that women who had urinary tract infections were more likely to have premature delivery. This is consistent with previous study in Iran[7]. This could be explained by the fact that infections trigger release inflammatory mediators such as prostaglandins and matrix degrading enzymes which stimulate uterine contraction hence preterm delivery.
Although the association between hypertension and increased risk of preterm delivery has been reported elsewhere[12], our study findings could not establish this relationship when adjusted for other confounders.
This study demonstrated that preterm delivery is still a challenging maternal health problem in the study area and may be the case in other similar settings. Some obstetric and medical factors were associated with preterm delivery. Early identification of these factors during prenatal care may prevent the risk of preterm delivery. This calls upon to reinforce antenatal care and services for better birth outcomes.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Acknowledgments
We really appreciate to all women who volunteer to provide their information making this study possible. We also thank all doctors‘and nurses at KCMC who helped us in one way or another during conducting this study.
[1] Lasiuk GC, Comeau T, Newburn-Cook C. Unexpected: an interpretive description of parental traumas’ associated with preterm birth.BMC Pregnancy Childbirth2013;13(Suppl 1):S13. DOI: 10.1186/1471-2393-13-S1-S13
[2] Zhang Y, Liu X, Gao S, Wang J, Gu Y, Zhang J, et al. Risk factors for preterm birth in five maternal and Child Health hospitals in Beijing.PloS One2012;7(12): e52780.
[3] Chang HH, Larson J, Blencowe H, Spong CY, Howson CP, Cairns-Smith S, et al. Preventing preterm births : trends and potential reductions with current interventions in 39 very high human development index countries.Lancet2013;381(9862):223–34. doi: 10.1016/S0140-6736(12)61856-X.
[4] Mahande MJ, Daltveit AK, Obure J, Mmbaga BT, Masenga G, Manongi R, et al. Recurrence of preterm birth and perinatal mortality in northern Tanzania: registry-based cohort study.Trop Med Int Health2013;18(8): 962-967.
[5] Ngowa JDK, Jean DK, Ngassam A, Dohbit JS, Nzedjom C, Kasia JM. Pregnancy outcome at advanced maternal age in a group of African women in two teaching hospitals in Younde, Cameroon.Pan Afr Med J2013;14: 134.
[6] Zhang Q, Cande VA, Zhu Li, Smulian JC. Maternal anaemia and preterm birth : a prospective cohort study.Int J Epidemiol2009;38(5):1380–1389. doi: 10.1093/ije/dyp243. .
[7] Alijahan R, Hazrati S, Mirzarahimi M, Pourfarzi F, Ahmadi Hadi P. Prevalence and risk factors associated with preterm birth in Ardabil, Iran.Iran J Reprod Med2014;12: 47–56.
[8] National Bureau of Statistics (NBS) (Tanzania), ICF Macro. Tanzania Demographic and Health Survey 2010, Dar es Salaam, Tanzania: NBS and ICF Macro; 2011. [Online]. Available from: http://www.nbs.go.tz/. [Accessed on January 12, 2015).
[9] Watson JD, Weiss HA, Changalucha JM, Todd J, Gumodoka B, Bulmer J, et al. Adverse birth outcomes in United Republic of Tanzania--impact and prevention of maternal risk factors.Bull World Health Organ2007;85(1): 9-18.
[10] Kinney MV1, Lawn JE, Howson CP, Belizan J. 15 Million preterm births annually: what has changed this year?Reprod Health2012;9: 28.
[11] Mumghamba E, manji KP. Maternal oral health status and preterm low birth weight at Muhimbili National Hospital, Tanzania : a case-control study.BMC oral Health2007;12: 1-12.
[12] Croteau A, Marcoux S, Brisson C. Work activity in pregnancy, preventive measures, and the risk of preterm delivery.Am J Epidemiol2007;166(8): 951-965.
[13] López PO, Paulina O, Bréart G. Sociodemographic characteristics of mother’s population and risk of preterm birth in Chile.Reprod Health2012;10: 26.
[14] Park M, Son M, Kim Y, Paek D. Social inequality in birth outcomes in Korea, 1995-2008.Korea Med Sci2013;28: 25-35.
[15] Steer, PJ. The epidemiology of preterm labour--why have advances not equated to reduced incidence?BJOG2006;113(Suppl): 1-3.
[16] Räisänen S, Mika G, Juho S, Michael K, Heinonen S. Contribution of risk factors to extremely, very and moderately preterm births-registerbased analysis of 1 390 742 singleton births.PloS One2013;8(4): e60660.
[17] Arash M, Dolatian M, Forouzan AS, Sajjadi H, Majd HA, Mahmoodi Z. Path analysis associations between perceived social support, stressful life events and other psychosocial risk factors during pregnancy and preterm delivery.Iran Red Crescent Med J2013;15(6): 507-514.
[18] Camilla N, Alwan NA, Greenwood DC, Simpson NA, Hay AW, White KL, et al. Maternal alcohol intake prior to and during pregnancy and risk of adverse birth outcomes: evidence from a British cohort.J Epidemiol Community Health2014;68(6): 542-549.
[19] Scholten BL, Page-christiaens GCM, Franx A, Hukkelhoven CW, Koster MP. The influence of pregnancy termination on the outcome of subsequent pregnancies: a retrospective cohort study.BMJ Open2013;3: e002803.
[20] Chen A, Yuan W, Meirik O, Wang X, Wu S, Zhous L, et al. Mifepristoneinduced early abortion and outcome of subsequent wanted pregnancy.Am J Epidemiol2004;160(2): 110-117.
[21] Offer E, Novack L, Klaitman V, Erez-Weiss I, Beer-Weisel R, Dukler D, et al. Early preterm delivery due to placenta previa is an independent risk factor for a subsequent spontaneous preterm birth.BMC Pregnancy Childbirth2012;12(1): 1.
[22] Kullima AA, Audu BM., Geidam AD. Outcome of twin deliveries at the University of Maiduguri Teaching Hospital: a 5-year review.Niger J Clin Pract2011;14(3): 345-348.
[23] Kurdi AM, Mesleh RA, Al-Hakeem MM, Khashoggi TY, Khalifa HM. Multiple pregnancy and preterm labor.Saudi Med J2004;25(5): 632-637.
[24] Muglia LJ, Michael K. The enigma of spontaneous preterm birth.N Engl J Med2010;362(6): 529-535.
[25] Khalil MM, Alzahra E: Fetal gender and pregnancy outcomes in Libya: a retrospective study.Libyan J Med2013;8: doi: 10.3402/ljm.v8i0.20008.
[26] Ancel P, Goffinet F. EPIPAGE 2 writing group. Epipage 2: a preterm birth cohort in France in 2011.BMC Pediatrics2014;14: 97.
[27] Getahun D, Lawrence JM, Fassett MJ, et al. The association between stillbirth in the first pregnancy and subsequent adverse perinatal outcomes.Am J Obstet Gynecol2009;201: 378.e1-6.
ment heading
10.1016/j.apjr.2016.07.009
*Corresponding author: Michael J Mahande, Department of Epidemiology and Biostatistics, Institute of Public Health, Kilimanjaro Christian Medical University College, Moshi, Tanzania
E-mail: jmmahande@gmail.com
Preterm delivery
Tanzania
 Asian Pacific Journal of Reproduction2016年5期
Asian Pacific Journal of Reproduction2016年5期
- Asian Pacific Journal of Reproduction的其它文章
- Heparin binding proteins and their relationship with vital sperm function tests visà-vis fertility of buffalo bull semen
- Conception rate in Holstein dairy cows having both normal sized follicles and cystic follicles at estrus
- Polymyxin B changes the plasma membrane integrity of cryopreserved bull semen
- Freezability of buffalo semen with TRIS extender enriched with disaccharides (trehalose or sucrose) and different glycerol concentrations
- Gum arabic improves semen quality and oxidative stress capacity in alloxan induced diabetes rats
- Ovarian hyperstimulation syndrome followed by ovarian torsion in premenopausal patient using adjuvant tamoxifen treatment for breast cancer