
从足癣患者趾间皮损处分离出黏膜毛孢子菌1例
2016-12-24 02:02胡文英许凤妮冉玉平代亚玲庄凯文
中国真菌学杂志 2016年2期
胡文英 许凤妮 冉玉平 代亚玲 庄凯文
(1.四川大学华西医院皮肤性病科,成都 610041;2.四川大学华西医院实验医学科,成都 610041)
·病例报告·
从足癣患者趾间皮损处分离出黏膜毛孢子菌1例
胡文英1许凤妮1冉玉平1代亚玲2庄凯文1
(1.四川大学华西医院皮肤性病科,成都 610041;2.四川大学华西医院实验医学科,成都 610041)
报道由黏膜毛孢子菌感染所致的足癣1例。患者因“双足趾间及足底脱屑伴瘙痒6个月”就诊,查体见双足趾间及足底白色鳞屑,双趾间潮湿,右足大拇趾有数个跖疣。取趾间皮屑直接镜检见大量分隔菌丝;真菌培养及分子鉴定为黏膜毛孢子菌。临床诊断为足癣、跖疣。分别予抗真菌及冷冻等治疗后治愈。
毛孢子菌;黏膜毛孢子菌;足癣
[Chin J Mycol,2016,11(2):117-118]
1 临床资料
患者女,26岁,因“双足趾间及足底脱屑伴瘙痒6个月”就诊。6个月前无明显诱因双足趾间及足底出现白色脱屑,伴瘙痒,自行局部外用药物 (具体不详)无明显好转,患者双足有多汗症。平素体健,职业为导游,喜穿运动鞋。家族及同事中无类似病史。
体格检查:双足趾间及足底白色脱屑,双足趾间潮湿,右足大拇趾见数个跖疣 (见图1)。皮肤镜 (江苏省捷达科技发展有限公司)检查:双足趾间红斑及脱屑明显 (见图2)。实验室检查:刀片刮取趾间鳞屑涂片,经美兰染色后在显微镜下观察见分隔菌丝 (见图3)。将鳞屑接种于含氯霉素及放线菌酮的沙氏培养基中,32℃培养,6 d后可见少量白色酵母样菌落生长 (见图4)。将菌株转种至含氯霉素及放线菌酮的马铃薯培养基中,14 d后在皮肤镜下观察见潮湿放射状黄白色酵母样菌落 (见图5)。小培养 (棉兰染色)见毛孢子菌典型的分隔及关节菌丝结构 (见图6)。用DNA提取试剂盒 (广州苏玛生物科技有限公司)提取培养菌落的DNA,按Sugita[1]的方法以引物26SF (5'-ATCCTTTGCAGACGACTTGA-3')及5SR (5'-AGCTTGACTTCGCAGATCGG-3')扩增 (Intergenic spacer,基因间隔序列,IGS)区域后送PCR产物测序,测序结果登陆GenBank 进行BLAST比对,与编号EU934806.1的黏膜毛孢子菌 (Trichosporonmucoides)株的同源性100%。GenBank序列号:KP453832。
诊断:足癣、跖疣。
治疗:镜检阳性后予盐酸特比萘芬250 mg,1次/d,10%聚维酮碘溶液泡足后外用1%萘替芬-0.25%酮康唑乳膏。跖疣予冷冻治疗及咪喹莫特乳膏外用。培养阳性并鉴定为黏膜毛孢子菌后将盐酸特比萘芬更换为伊曲康唑胶囊200 mg,2次/d,口服 (牛奶送服)2周。患者自行停药3个月后复诊时双足趾间及足底已无脱屑 (见图7~8),瘙痒减轻。镜检及培养均为阴性。继续服药3周后停药。随访半年无复发。
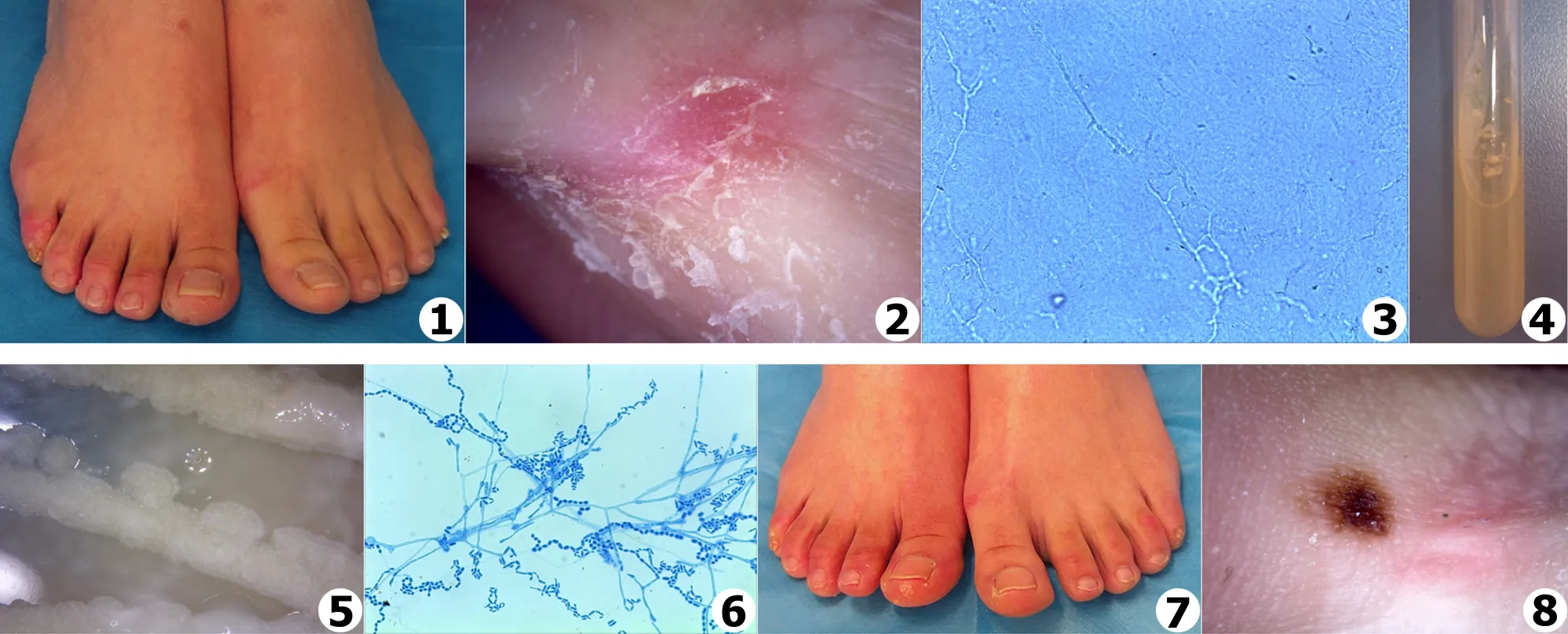
图1 治疗前皮损 图2 皮肤镜下观察趾间脱屑明显 图3 皮屑内菌丝 (美兰染色×400) 图4 沙氏培养基6 d 图5 将菌种接种于马铃薯培养基,32℃培养14 d,皮肤镜下见潮湿放射状黄白色酵母样菌落 (在皮肤镜下放大观察) 图6 小培养镜下见典型关节菌丝 (棉兰染色×400) 图7 治疗3个月后皮损缓解 图8 皮肤镜下观察趾间脱屑消失
Fig.1 Tinea pedis before treatment Fig.2 Scales between the toes under dermoscopy Fig.3 Hyphae inside the scales (×400) Fig.4 Colonies on Sabouraud dextrose agar after 14 d at 32℃ Fig.5 Colonies on potato dextrose agar under dermoscopy Fig.6 Slide culture showed the typical septate hyphae and arthroconidia cells (×400) Fig.7 Lesions at 3 months after treatment Fig.8 Lesions under dermoscopy after treatment
2 讨 论
毛孢子菌属于担子菌门伞菌亚门银耳纲银耳目真菌,广泛存在于土壤、树木、河流等自然界中,部分毛孢子菌参与皮肤及黏膜定植[2]。临床上以非洲裔人群为主的毛结节病是毛孢子菌所致代表性浅部感染。而在患恶性肿瘤、HIV感染、使用免疫抑制剂等免疫缺陷人群中毛孢子菌则可引起侵袭性感染。日本报道毛孢子菌还与夏季超敏型肺炎相关[3]。
自1865年Beigel发现首例毛孢子菌头发感染的患者以来,现已发现毛孢子菌50余种,其中与临床相关的有阿萨希毛孢子菌 (T.asahii)、黏膜毛孢子菌 (T.mucoides)、皮瘤毛孢子菌 (T.inkin)等16种[4],而黏膜毛孢子菌为侵袭性感染的主要菌种之一[5]。Lacasse等[6]报道1例肝移植术后患黏膜毛孢子菌血症病例。该患者第2次肝移植术后血培养分离出黏膜毛孢子菌,抗真菌治疗 (泊沙康唑200 mg口服,3次/d)后转氨酶和血清肌酐下降,临床症状有所改善。Chen等[7]报道1例因连续流动式腹膜透析患毛孢子菌腹膜炎。该患者因狼疮肾炎致终末期肾病行腹膜透析4 a多后出现寒战、发热,在口服氟康唑前后的2次腹腔积液培养中均分离出黏膜毛孢子菌,静脉用氟康唑后仍无效,改为静脉用两性霉素B预后不详。黏膜毛孢子菌引起浅表感染非常少见。Sageerabanoo等[8]报道了1例由毛孢子菌引起甲真菌病的病例,进行药敏试验后该患者口服特比萘芬250 mg,1次/d,4个月后痊愈。此外黏膜毛孢子菌还可与皮瘤毛孢子菌共同引起毛结节病[9]。上述4例或未具体描述鉴定方法,或用形态及生化方法鉴定。黏膜毛孢子菌相关病例报告少见,其原因除了毛孢子菌感染的病例数不多外,也可能与菌种鉴定方法有关。自2002年Sugita等开始以IGS区对毛孢子菌做分子生物学分类鉴定以来,形态学及生化方法已不能满足毛孢子菌的分类鉴定需要,而大多数对毛孢子菌的鉴定仍然停留在该水平。
本例患者由临床表现及皮肤镜检查提示、真菌镜检初诊为“足癣”,因足癣是由皮肤癣菌所致,故予特比萘芬口服。当真菌培养、PDA小培养及分子测序确认为黏膜毛孢子菌后将特比萘芬更换为伊曲康唑口服,效果良好。
[1] Sugita T,Nakajima M,Ikeda R,et al.Sequence analysis of the ribosomal DNA intergenic spacer 1 regions ofTrichosporonspecies[J].J Clin Microbiol,2002,40(5):1826-1830.
[2] Silvestre AM,Miranda JrMAR,Camargo ZP.Trichosporonspecies isolated from the perigenital region,urine and catheters of a Brazilian population[J].Braz J Microbiol,2010,41(3):628-634.
[3] Sugita T,Ikeda R,Nishikawa A.Analysis ofTrichosporonisolates obtained from the houses of patients with summer-type hypersensitivity pneumonitis[J].J Clin Microbi,2004,42(12):5467-5471.
[4] Pagnocca FC,Legaspe MFC,Rodrigues A,et al.Yeasts isolated from a fungus-growing ant nest,including the description ofTrichosporonchiarelliisp.nov.,an anamorphic basidiomycetous yeast[J].Int J Syst Evol Microbiol,2010,60(6):1454-1459.
[5] Colombo AL,Padovan ACB,Chaves GM,et al.Current knowledge ofTrichosporonspp.and Trichosporonosis[J].Clin Microbiol Rev,2011,24(4):682-700.
[6] Lacasse A,Clevel KO.Trichosporonmucoidesfungemia in a liver transplant recipient:case report and review[J].Transpl Infect Dis,2009,11(2):155-159.
[7] ChenYT,Yang WC,Chen TW,et al.Trichosporonmucoidesperitonitis in a continuous ambulatory peritoneal dialysis patient[J].Perit Dial Int,2013,33(3):341-342.
[8] Sageerabanoo,Malini A,Oudeacoumar P,et al.Onychomycosis due toTrichosporonmucoides[J].Indian J Dermatol Venereol Leprol,2011,77(1):76-77.
[9] Tendolkar U,Shinde A,Baveja S,et al.TrichosporoninkinandTrichosporonmucoidesas unusual causes of white piedra of scalp hair[J].Indian J Dermatol Venereol Leprol,2014,80(4):324-327.
[本文编辑] 卫凤莲
Trichosporonmucoidesisolated from the toes in a tinea pedis patient
HU Wen-ying1,XU Feng-ni1,RAN Yu-ping1,DAI Ya-ling2,ZHUANG Kai-wen1
(1.DepartmentofDermatoverenology;2.DepartmentofLaboratoryMedicine,WestChinaHospital,SichuanUniversity,Chengdu610041,China)
Trichosporonmucoidesisolated from the toes in a tinea pedis patient was reported.The patient had a history of itching and scaling of feet for 6 months.Her toes were sweaty with white scaling,and her big toe of right foot had plantar warts.Direct microscopic examination of scale samples showed septate hyaline hyphae;fungal colonies developed on Sabouraud dextrose agar after inoculating for 2 weeks were identified asTrichosporonmucoidesby molecular identification.The diagnoses were tinea pedis and plantar warts.The lesions were completely cured by antifungals,cryotherapy and imiquimod cream.
Trichosporon;Trichosporonmucoides;tinea pedis
胡文英,女 (汉族),硕士研究生在读.E-mail:huwenying31@163.com
冉玉平,E-mail:ranyuping@vip.sina.com
R 379.9 R 756.3
A
1673-3827(2016)11-0117-02
2015-05-20
猜你喜欢
武警医学(2022年3期)2022-04-07
中国民间疗法(2020年22期)2021-01-07
科学生活(2019年7期)2020-01-01
自我保健(2019年4期)2019-08-02
中外医疗(2019年12期)2019-08-01
中国感染控制杂志(2015年7期)2015-12-13
科学大众(中学)(2015年9期)2015-10-12
中国医疗美容(2015年1期)2015-07-12
少儿科学周刊·少年版(2015年3期)2015-07-07
中国人兽共患病学报(2015年8期)2015-05-09
