
Dexamethasone prevents vascular damage in earlystage non-freezing cold injury of the sciatic nerve
2016-12-01 12:37:47HaoLiLeiZhangMinXu
中国神经再生研究(英文版) 2016年1期
Hao Li, Lei Zhang, Min Xu
1 Department of Neurology, the First People’s Hospital of Yibin, Yibin, Sichuan Province, China
2 Department of Pharmacy, the First People’s Hospital of Yibin, Yibin, Sichuan Province, China
3 Department of Neurology, Xuanwu Hospital Capital Medical University, Beijing, China
RESEARCH ARTICLE
Dexamethasone prevents vascular damage in earlystage non-freezing cold injury of the sciatic nerve
Hao Li1,*, Lei Zhang2, Min Xu3
1 Department of Neurology, the First People’s Hospital of Yibin, Yibin, Sichuan Province, China
2 Department of Pharmacy, the First People’s Hospital of Yibin, Yibin, Sichuan Province, China
3 Department of Neurology, Xuanwu Hospital Capital Medical University, Beijing, China
Graphical Abstract
orcid: 0000-0002-5061-5113 (Hao Li)
Non-freezing cold injury is a prevalent cause of peripheral nerve damage, but its pathogenic mechanism is poorly understood, and treatment remains inadequate. Glucocorticoids have anti-inflammatory and lipid peroxidation-inhibiting properties. We therefore examined whether dexamethasone, a synthetic glucocorticoid compound, would alleviate early-stage non-freezing cold injury of the sciatic nerve. We established Wistar rat models of non-freezing cold injury by exposing the left sciatic nerve to cold (3-5°C) for 2 hours, then administered dexamethasone (3 mg/kg intraperitoneally) to half of the models. One day after injury, the concentration of Evans blue tracer in the injured sciatic nerve of rats that received dexamethasone was notably lower than that in the injured sciatic nerve of rats that did not receive dexamethasone; neither Evans blue dye nor capillary stenosis was observed in the endoneurium, but myelinated nerve fibers were markedly degenerated in the injured sciatic nerve of animals that received dexamethasone. After dexamethasone administration, however, endoneurial vasculopathy was markedly improved, although damage to the myelinated nerve fiber was not alleviated. These findings suggest that dexamethasone protects the blood-nerve barrier, but its benefit in non-freezing cold injury is limited to the vascular system.
nerve regeneration; peripheral nerve injury; sciatic nerve; hypothermia; blood-nerve barrier; non-freezing cold injury; dexamethasone; neural regeneration
Introduction
Cold injury occurs when human tissue is exposed to extreme cold. There are two main types of cold injury: (1) freezing injury, caused by exposure to temperatures below 0°C; and (2) non-freezing cold injury, caused by exposure to temperatures of 0-10°C in a wet environment, including frostbite, trench foot, and immersion foot. Non-freezing cold injury of peripheral nerves has been studied since the time of Hippocrates, and in particular during military campaigns such as the Second World War and the Korean War, which saw a high incidence of trench foot (Smith et al., 1915; Greene, 1941; Ungley and Durh, 1942; Blackwood, 1944; Lewis and Moen, 1952). Even during peacetime, non-freezing cold injury affects mountaineers (Marcus, 1979; Imray and Oakley, 2005; Imray et al., 2009), fishermen (Mills and Mills, 1993; Cattermole, 1999), homeless persons in winter (King et al., 1958; Cattermole, 1999) and alcohol abusers (Brändström et al., 2014). During the China snowstorms in 2008, the incidence of non-freezing cold injury reached 12.78% in Ningbo city, accounting for 67.28% of all types of injury (Ying et al.,2009). Despite extensive research, however, the pathological mechanism underlying non-freezing cold injury remains poorly understood. In some regions of China, it is wrongly believed that cold injury can be alleviated by drinking alcohol, heating with fire, and rubbing with snow (Zhu et al., 2008). Improper treatment methods such as these increase the rate of disability arising from cold injury to 92.8% (Liu et al., 2007). It was recently reported that non-freezing cold injury of the peripheral nerve damages the blood-nerve barrier and vascular endothelial cell layer, causing endoneurial edema, and increasing blood vessel permeability and local hydrostatic pressure, and may lead to cellular hypoxia (Li et al., 2015).
Glucocorticoids are anti-inflammatory and are often used to alleviate tissue edema and trauma-induced inflammatory response. The mechanisms by which glucocorticoids treat nerve injury include inhibition of phospholipase A2 activity; prevention of granulocyte, mast cell and macrophage degranulation; inhibition of macrophage migration inhibitory factor, and stabilization of the lysosomal membrane (Suslu et al., 2013). Dexamethasone is a synthetic glucocorticoid, often used to alleviate trauma-induced nerve tissue edema. One possible mechanism by which dexamethasone inhibits nerve inflammation is its inhibition of CD3-positive inflammatory cell infiltration of local tissue (Feng and Yuan, 2015). In addition, dexamethasone can downregulate the expression of pro-inflammatory factors, such as tumor necrosis factor-α and interleukin-1β. These pro-inflammatory factors increase the expression of induced nitric oxide synthase in the injured region, leading to nitric oxide production and cell apoptosis (Regina et al., 2009). Upregulation of induced nitric oxide synthase and production of nitric oxide in nervous tissue are also involved in non-freezing cold injury of the peripheral nerve (Wu et al., 2009). Therefore, in the present study, we investigated the efficacy of dexamethasone as a treatment for early-stage non-freezing cold injury of the sciatic nerve.
Materials and Methods
Animals
Thirty-two male adult Wistar rats of specific-pathogen free grade, aged 3-4 months and weighing 300-400 g, were purchased from Beijing Vital River Laboratory Animal Technology Co., Ltd., Beijing, China (certificate No. SCXK (Jing) 2002-003). The rats were housed at 25°C and 50% relative humidity. All experimental procedures were approved by the Animal Ethics Committee of Beijing Capital Medical University, China.
Preparation of rat models of non-freezing cold injury
Models of non-freezing cold injury were established as described previously (Jia and Pollock, 1997). In brief, rats were anesthetized by intraperitoneal injection of 2% sodium pentobarbital (0.25 mL/100 g), and placed in the prone position. The skin was disinfected and the left sciatic nerve was fully exposed via a 3 cm mid-thigh incision. A cooling chamber was placed around the nerve (Li et al., 2015), and the nerve was subjected to 2 hours of hypothermia at 3-5°C before removal from the cooling chamber. The right (control) sciatic nerve was exposed in the same manner, but without hypothermia. The temperature of the nerve and circulating water in the cooling chamber was recorded once every 20 minutes with a digital temperature measurement system (UT325A type, Uni-trend Technology (China) Limited, Guangdong Province, China). Rectal temperature and heart rate were monitored throughout the modeling of non-freezing cold injury. Rectal temperature was maintained at 35°C using an electric heat blanket.
Experimental grouping and drug administration
The thirty-two rat models of non-freezing cold injury were randomly and equally allocated to an injury group and a treatment group. Rats in the treatment group received 3 mg/kg dexamethasone sodium phosphate intraperitoneally (approval No. 1410410-811; Jiaozuo Rongsheng Pharmaceutical Co., Ltd., Henan Province, China) immediately after injury.
Evans blue labeling
Twenty-three hours after injury, Evans blue-albumin solution [physiological saline containing 5% fetal bovine serum (Amresco, Solon, OH, USA) and 1% Evans blue (Sigma-Aldrich, Wuxi, Jiangsu Province, China)] was injected into eight rats from each group intravenously (l mL/100 g). One hour later, sciatic nerves were dissected out bilaterally, blotted dry, weighed, and placed in 1 mL formamide at 50°C for 24 hours. The optical density of Evans blue was measured by spectrometry (Shimadzu Corporation, Suzhou, Jiangsu Province, China; type UV-1800), and its tissue concentration was calculated according to a standard curve.
In four further rats per group, the sciatic nerves were isolated, cut into lengths of 5 mm, embedded in Tissue-Tek Optical Cutting Temperature Compound (Sakura Finetek, Torrance, CA, USA), frozen in liquid nitrogen, and stored at −80°C until use. The segments were cut into transverse sections 10 µm thick, mounted with glycerol-saline (1:1, v/v), and observed under a fluorescence microscope to determine the distribution of Evans blue in the nerve.
Toluidine blue staining and electron microscopy
Twenty-four hours after non-freezing cold injury, the remaining four rats per group were anesthetized with an intraperitoneal injection of phenobarbital sodium (50 mg/kg), and the sciatic nerves were removed bilaterally. The tissue was fixed in 2% paraformaldehyde with 2.5% glutaral for 2 hours at 4°C, rinsed three times with 0.1 M PBS for 10 minutes each time, and fixed using osmium tetroxide. It was then dehydrated with ethanol, embedded in epoxy resin Epon812, cut into sections 1 µm thick, stained with toluidine blue, and observed under an optical microscope (Eclipse 50i POL; Nikon, Melville, NY, USA). The sections were then cut into 5 nm ultrathin sections, stained with uranyl acetate and lead citrate, and observed under a transmission electron microscope (EM208s; Royal Philips, Eindhoven, the Netherlands).
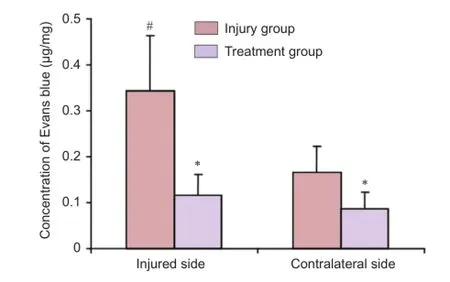
Figure 1 Effect of dexamethasone on the concentration of Evans blue in the sciatic nerve after non-freezing cold injury.
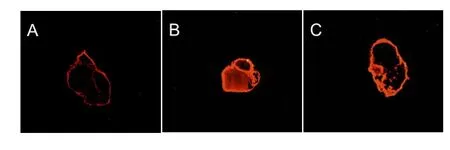
Figure 2 Representative cross-sections of sciatic nerves (Evans blue staining, × 40) 1 day after non-freezing cold injury.
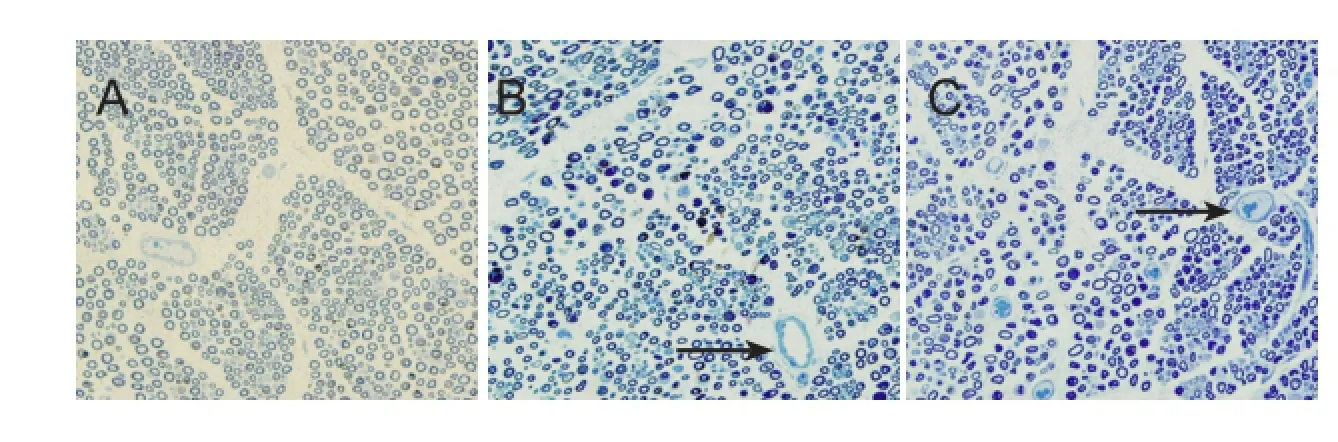
Figure 3 Effects of dexamethasone on the morphology of the sciatic nerve 1 day after non-freezing cold injury (toluidine blue staining, × 400).

Figure 4 Effects of dexamethasone on the ultrastructure of the sciatic nerve after non-freezing cold injury (toluidine blue staining, transmission electron microscope).
Statistical analysis
All measurement data were analyzed using a completely randomized analysis of variance (SPSS 13.0 software; SPSS, Chicago, IL, USA) and are expressed as the mean ± SD. Paired t-tests were used for pairwise comparisons. P < 0.05 was considered statistically significant.
Results
Dexamethasone prevented the non-freezing cold injury-induced increase in Evans blue concentration in the sciatic nerve
The concentration of Evans blue in the hypothermia-injured sciatic nerve one day after injury was significantly greaterthan that in the control sciatic nerve (P < 0.05) in rats that did not receive dexamethasone. But, this significant difference could not be observed in the rats that received dexamethasone (P > 0.05; Figure 1).
Dexamethasone inhibited the dispersion of Evans blue in the sciatic nerve after non-freezing cold injury
One hour after Evans blue administration, red fluorescence in the cross-section of the contralateral sciatic nerve was limited to the endoneurial vascular cavity; no leakage of fluorescence was observed outside the blood vessel. One day after hypothermia-induced injury, diffuse red fluorescence appeared across most of the cross-section of the hypothermia-injured sciatic nerve. In dexamethasone-treated rats, a very small amount of fluorescence was observed outside the endoneurial vessels (Figure 2).
Dexamethasone improved the morphology of the sciatic nerve after non-freezing cold injury
Toluidine blue staining of the sciatic nerve on the contralateral side revealed few damaged myelinated nerve fibers with empty or dark axons, and endoneurial microvessels appeared normal (Figure 3A). One day after injury, degeneration was observed, characterized by large, empty, atrophic, or dark axons, in a large number of myelinated sciatic nerve fibers; stenosis of the endoneurial microvessel was observed, caused by swelling of the endothelial cells (Figure 3B). After dexamethasone administration, myelinated nerve fibers still showed axonal degeneration, but stenosis of the endoneurial microvessels and vascular endothelial cell swelling were not observed (Figure 3C).
Dexamethasone alleviated damage to the ultrastructure of the sciatic nerve after non-freezing cold injury
Transmission electron microscopy 1 day after injury revealed that a small number of myelinated fibers in the control sciatic nerve showed a slightly loose sheath layer; unmyelinated nerve fibers and endoneurial microvessels appeared normal. In the injured nerve, however, myelinated nerve fibers showed severe lesions, identified by loose, or completely absent, myelin sheath layers and axonal microfilaments (manifesting as “empty” axons), in addition to endoneurial microvessel stenosis, and proliferation of vascular endothelial cells. Tight junctions were not destroyed, however, and no platelet activation or red cell stasis was observed. Unmyelinated nerve fibers appeared normal. After dexamethasone administration, no vascular endothelial cell proliferation was observed, and the endoneurial microvessel cavity was normal; however, myelinated nerve fiber lesions were not improved. Unmyelinated nerve fibers were normal, and tight junctions were intact (Figure 4).
Discussion
Jia and Pollock (1997) reported that ischemia/reperfusion of the sciatic nerve in non-freezing cold injury leads to oxidative damage. Geng et al. (2008, 2009) showed that in the rewarming stage of non-freezing cold injury, production of oxygen free radicals in the sciatic nerve is markedly increased. Oxygen free radicals damage the peripheral nerve by damaging microvascular endothelial cells and thereby destroying the blood-nerve barrier, leading to endoneurial edema (Liu, 1998). Excessive endoneurial liquid leads to a rapid elevation of endoneurial pressure (Myers et al., 1981), resulting in increased vascular resistance, and aggravating endoneurial hypoxia. This type of blood-nerve barrier lesion is also likely to be associated with vasoactive amine release by degranulation of endoneurial mast cells: vasoactive amines can destroy the microvessel barrier, increasing permeability, indicating that inflammation is involved in this process (Olsson, 1968).
In the present study, 1 day after non-freezing cold injury, the concentration of Evans blue in the sciatic nerve on the injured side was markedly higher than that on the contralateral side. Diffuse endoneurial distribution of Evans blue was observed, indicating that endoneurial microvessel permeability was increased compared with the control side, bloodnerve barrier function was impaired, and blood exuded from the vessels into the endoneurium. After dexamethasone administration, however, the concentration of Evans blue in the sciatic nerve was notably lower than that in the untreated injured nerve, and endoneurial Evans blue was only present in the microvessels, suggesting that dexamethasone improves endoneurial microvessel permeability and protects the blood-nerve barrier. However, transmission electron microscopy revealed that endoneurial vasculopathy, but not myelinated nerve fiber lesioning, is alleviated after dexamethasone administration. This suggests that dexamethasone treatment of non-freezing cold injury is limited to lesions of the vascular system.
Non-freezing cold injury of the peripheral nerve is considered to be an “ischemia plus” syndrome. The underlying mechanism involves many pathways (Jia et al., 1998; Li et al., 2010), including sodium ion channel impairments, inactivation of temperature-sensitive enzymes in active transport, nerve fiber phagocytosis by macrophages, and ischemia/ reperfusion injury, but the precise mechanism remains poorly understood. Dexamethasone only alleviates the inflammatory reaction and ischemia-reperfusion injury, but does not interact with other injury pathways, and therefore cannot completely repair nerve fiber lesions. The mechanism underlying non-freezing cold injury warrants further investigation. In the clinic, a multifaceted treatment approach is necessary for non-freezing cold injury.
Author contributions: HL collected the data and wrote the paper. LZ and MX designed the study and provided critical revision of the paper. All authors approved the final version of this paper.
Conflicts of interest: None declared.
Plagiarism check: This paper was screened twice using Cross-Check to verify originality before publication.
Peer review: This paper was double-blinded and stringently reviewed by international expert reviewers.
Blackwood W (1944) Studies in the pathology of human ‘immersion foot’. Br J Surg 31:329-350.
Brändström H, Johansson G, Giesbrecht GG, Ängquist KA, Haney MF (2014) Accidental cold-related injury leading to hospitalization in northern Sweden: an eight-year retrospective analysis. Scand J Trauma Resusc Emerg Med 22:6.
Cattermole TJ (1999) The epidemiology of cold injury in Antarctica. Aviat Space Environ Med 70:135-140.
Feng X, Yuan W (2015) Dexamethasone enhanced functional recovery after sciatic nerve crush injury in rats. Biomed Res Int 2015:627923.
Geng ZW, Zhang J, Tong XY, Liu J (2009) Investigation of oxygen free radical in locate temperature change of the sciatic nerve. Heilongjiang Yixue 33:493-496.
Geng ZW, Xu M, Wu Y, Li H, Jia JP (2008) The investigation of oxygen free radical in non-freezing cold injury of the sciatic nerve in the rat. Nao yu Shenjing Jibing Zazhi 16:598-601.
Greene R (1941) Frostbite and kindred ills. Lancet 238:689-693.
Imray C, Grieve A, Dhillon S, Caudwell Xtreme Everest Research Group (2009) Cold damage to the extremities: frostbite and non-freezing cold injuries. Postgrad Med J 85:481-488.
Imray CH, Oakley EH (2005) Cold still kills: cold-related illnesses in military practice freezing and non-freezing cold injury. J R Army Med Corps 151:218-222.
Jia J, Pollock M (1997) The pathogenesis of non-freezing cold nerve injury. Observations in the rat. Brain 120:631-646.
Jia J, Pollock M, Jia J (1998) Cold injury to nerves is not due to ischaemia alone. Brain 121:989-1001.
King RC, Parrish JA, Allibone A (1958) Trench-foot in peacetime England. Br Med J 1:1099-1102.
Lewis RB, Moen PW (1952) Experimental immersion leg. Am J Med Sci 224:529-539.
Li H, Jia JP, Xu M, Zhang L (2015) Changes in the blood-nerve barrier after sciatic nerve cold injury: indications supporting early treatment. Neural Regen Res 10:419-424.
Li H, Xu M, Geng ZW, Jia JP, Wu Y, Liu FY, Song JX (2010) The analysis of macrophages in non-freezing cold Injury of the sciatic nerves. Nao yu Shenjing Jibing Zazhi 18:432-435.
Liu JY (1998) The role of oxygen free radicals in the pathogenesis of frostbite. Jiefangjun Yufang Yixue Zazhi 16:72-74.
Liu YH, Yang WN, Yang GY, Chen XY (2007) Analysis on related factors of 200 cases’frostbite resulting in disability in cold highland areas. Linchuang Junyi Zazhi 35:94-95.
Marcus P (1979) “Trench foot” caused by the cold. Br Med J 1:622-622. Mills WJ, Mills WJ (1993) Peripheral non-freezing cold injury: immersion injury. Alaska Med 35:117-128.
Myers RR, Powell HC, Heckman HM, Costello ML, Katz J (1981) Biophysical and pathological effects of cryogenic nerve lesion. Ann Neurol 10:478-485.
Olsson Y (1968) Mast cells in the nervous system. Int Rev Cytol 24:27-70.
Regina G, Angiletta D, Impedovo G, Robertis GD, Fiorella M, Carratu MR (2009) Dexamethasone minimizes the risk of cranial nerve injury during CEA. J Vasc Surg 49:99-102.
Smith JL, Ritchie J, Dawson J (1915) Clinical and experimental observations on the pathology of trench frostbite. J Pathol Bacteriol 20:159-190.
Song B, Zhang YQ (2008) Analysis of frostbite in the north island recruits training. Bethune Juyi Xueyuan Xuebao 6:363-364.
Suslu H, Altun M, Erdivanli B, Turan Suslu H (2013) Comparison of the effects of local and systemic dexamethasone on the rat traumatic sciatic nerve model. Turk Neurosurg 23:623-629.
Ungley CC, Durh MD (1942) Peripheral vasoneuropathy after chilling“immersion foot and immersion hand”. Lancet 240:447-451.
Wu Y, Jia JP, Xu M, Geng ZW, Liu FY, Song JX, Li H (2009) Role of nitric oxide in pathogenesis of cold nerve injury. Zhonghua Yi Xue Za Zhi 89:2214-2220.
Ying YY, Zhu YC, Xu R, Dong HJ, Shi NF, Xu LR, Cai YB, Ma X, Ping JM, Xu GZ (2009) Epidemiological investigation of disaster caused by damage and frozen in Ningbo area in 2008. Weisheng Yanjiu 38:463-464.
Zhu YC, Ying YY, Xu R, Ping JM, Ma X, Xu GZ (2008) Survey on injury and KAP level of anti-frostbite among farmers during the snowstorm disaster in Ningbo of Zhejiang province, 2008. Jibing Jiance 23:777-779.
Copyedited by Slone-Murphy J, Robens J, Yu J, Li CH, Song LP, Zhao M
10.4103/1673-5374.175064
How to cite this article: Li H, Zhang L, Xu M (2016) Dexamethasone prevents vascular damage in early-stage non-freezing cold injury of the sciatic nerve. Neural Regen Res 11(1)∶163-167.
Funding: This study was supported by grants from “Shihuida” Scientific Research Program of Sichuan Province Medical Association of China, No. SHD12-21; and Medical Scientific Research Program of Health Bureau of Yibin City in China.
http://www.nrronline.org/
Accepted: 2015-08-14
*Correspondence to: Hao Li, lihao_1981@163.com.
- 中国神经再生研究(英文版)的其它文章
- Vascular endothelial growth factor: an attractive target in the treatment of hypoxic/ischemic brain injury
- Angiogenesis in tissue-engineered nerves evaluated objectively using MICROFIL perfusion and micro-CT scanning
- Cerebrolysin improves sciatic nerve dysfunction in a mouse model of diabetic peripheral neuropathy
- A novel bioactive nerve conduit for the repair of peripheral nerve injury
- Treatment with analgesics after mouse sciatic nerve injury does not alter expression of wound healingassociated genes
- Time representation of mitochondrial morphology and function after acute spinal cord injury